
Total knee arthroplasty (TKA) is a commonly performed surgical procedure to improve mobility and reduce pain in patients with advanced knee joint disease [1]. Despite its benefits, effective postoperative pain management remains a clinical challenge. Optimal pain control is crucial to facilitate early mobilization, reduce the length of hospital stay, and enhance functional recovery [2]. Regional anesthesia techniques have gained significant attention for their ability to provide targeted analgesia while minimizing the side effects associated with systemic opioid use [3].
The iPACK (infiltration between the popliteal artery and capsule of the knee) block combined with an adductor canal block (ACB) has emerged as a promising strategy for managing pain following TKA [4]. The iPACK block targets the articular branches of the tibial nerve and the posterior branch of the obturator nerve, providing posterior knee analgesia without motor blockade [5]. When combined with the ACB, which anesthetizes the saphenous nerve (a sensory branch of the femoral nerve), this approach effectively covers the anterior and me-dial aspects of the knee [5]. This combination aims to provide comprehensive analgesia while preserving quadriceps strength, which is essential for early postoperative mobilization [6].
On the other hand, the lumbar erector spinae plane block (L-ESPB) at the L2 level has gained interest due to its potential to provide extensive anal-gesic coverage. The L-ESPB involves the deposition of local anesthetic into the fascial plane between the erector spinae muscle and the transverse processes of the vertebrae. At the L2 level, this block can spread cephalad and caudad, affecting spinal nerves’ dorsal and ventral rami [7]. This spread can extend to encompass the lumbar plexus and, to a certain extent, the sacral plexus, providing coverage for both the anterior and posterior aspects of the knee joint [8, 9]. The mechanism involves diffusion of the anesthetic through the paravertebral and epidural spaces, potentially blocking multiple neural pathways involved in knee innervation [10].
This study is justified by the need to evaluate and compare these two analgesic efficacy and safety techniques. While both the iPACK with ACB and L-ESPB have demonstrated potential individually, limited data compare their efficacy head to head in TKA.
This randomized, double-blinded, controlled trial aimed to compare the analgesic efficacy and motor-sparing characteristics of the L-ESPB with the combination of IPACK and ACB in patients undergoing TKA. Our primary objective was to evaluate postoperative pain relief, opioid consumption, stress response expressed by the neutrophil-tolymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), and motor function preservation between these two approaches to determine whether the L-ESPB can serve as an effective alternative to the widely used IPACK+ACB combination.
This study could provide valuable insights into optimizing regional anesthesia techniques for TKA, potentially streamlining pain management while enhancing patient recovery and satisfaction.
METHODS
This double-blinded and prospective randomized controlled trial (RCT) was conducted in a single center in Poland. The trial was registered on January 22, 2024, at ClinicalTrials.gov (NCT06233630). The Poznan University of Medical Sciences Bio-ethics Committee and its chairman, Maciej Krawczyński, approved the study on March 7, 2024, protocol number 107/24. Enrollment occurred from 30.03.2024 to 16.08.2024. Written informed consent was obtained from all patients for these scientific contributions. The study was conducted following the Declaration of Helsinki.
Patient recruitment
Enrollment was proposed before surgery to patients scheduled for TKA under spinal anesthesia, aged > 18 years < 100 years old, and American Society of Anesthesiologists physical status I, II, or III.
Patients were not included in this study if they refused to participate, had a history of bleeding diathesis, took anticoagulant therapy, had a history of chronic pain before surgery, had multiple traumas, could not assess their pain, had been operated on under general anesthesia, had an infection in the area, or did not accept the procedure.
Randomization and concealment
Computer software randomly assigned patients 1 : 1 : 1 to receive ultrasound-guided iPACK block with ACB, L-ESPB, or the control group using a randomization list generated by the nQuery Advisor program (Statistical Solutions, Boston, MA, USA).
The double-blinding in this study was accomplished via the strict design of the work tasks for the researchers, who were unaware of each other’s final scores. The first researcher, who was blinded to group allocation and study design, prepared sealed opaque envelopes for each patient. The consultant anesthesiologist opened the envelopes on the morning of surgery and assigned each patient accordingly. Before surgery, another anesthesiolo-gist performed the spinal anesthesia followed by iPACK with ACB or L-ESPB in the pre-anesthesia room. As a result, the anesthesia team, surgeons, operating room staff, and patients were blinded to the study group assignment. The group blinding was unmasked after completion of the statistical analysis. Two investigators collected all the data.
All patients underwent knee surgery under spinal anesthesia performed by one surgical team at the Orthopaedical Hospital at Poznan University of Medical Sciences.
The patients underwent at least two days of active follow-up after surgery. An independent researcher gathered the primary and secondary outcomes during in-patient hospital visits.
Pain reporting and management
One investigator, blinded to group allocation and study design, trained subjects to report pain levels using an NRS (Numeric Rating Scale) ranging from 0 to 10 (0 = no pain, and 10 = extreme pain). Mild pain was defined as an NRS of 1–3 points. The trainer explained the causes and mechanisms of incisional and bone pain, using an approach that considered the subject’s educational background and sex. The trainer also explained how analgesic drugs control pain, common adverse reactions to analgesics, and how they were treated and prevented.
Procedures
Thirty minutes before surgery, subjects were admitted to the pre-anesthesia room and monitored for continuous electrocardiography, pulse oximetry, and noninvasive blood pressure, with supplemental oxygen delivery via a nasal cannula. In all groups, the patients received midazolam 7.5 mg p.o. a half hour before the surgery as part of the multimodal pre-emptive analgesia protocol. All patients received standardized spinal anesthetic management under mild sedation as standard practice in our hospital. Mild sedation was performed with continuous propofol infusion at 5 mg kg–1 h–1, which was continued throughout the entire surgery. Spontaneous ventilation was maintained with an oxygen mask at 2 L min–1. Spinal anesthesia (L3/4, Sprotte needle 27 G, 90 mm, PAJUNK, Geisingen, Germany) was performed with 4 mL of 0.5% ropivacaine. There was no surgeon-delivered periarticular infiltration during surgery. Two anesthesiologists performed the blocks. Both had at least five years of experience in post-specialty clinical expertise focused on regional anesthesia.
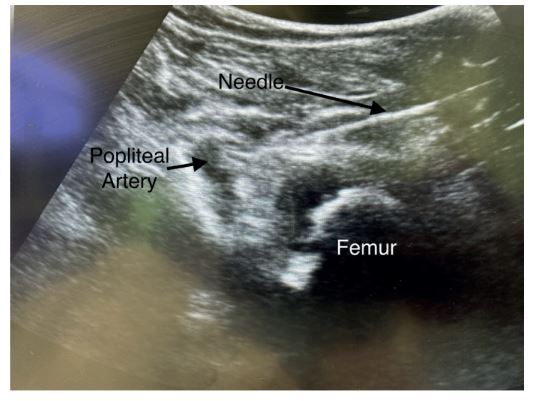
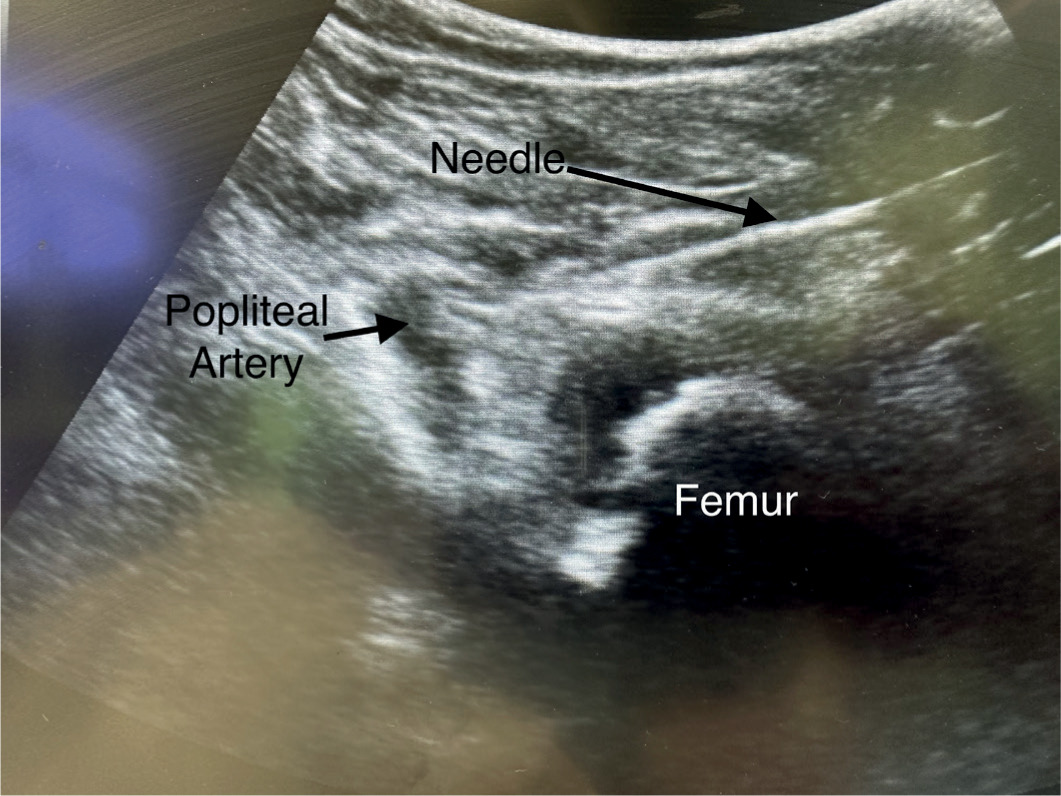
iPACK block procedure (Figure 1)
After the spinal anesthesia and before the surgical incision, the iPACK block was performed. The patient was placed in the supine position. We used a linear, high-frequency 4–8 MHz sono-graphic ultrasound probe and a 22-gauge needle (Stimuplex Ultra 360, 80 mm, Melsungen, Germany). The transducer was placed transversely over the medial aspect of the knee, 2–3 cm above the patella. The transducer was slid proximally to identify the distal femoral shaft and popliteal artery. The needle was inserted in-plane, from the anteromedial facet of the knee, into the space between the femur and popliteal artery. When the posterior part of the popliteal artery was reached, hydro-location positioning was performed with 2 mL of 0.9% isotonic saline. After the negative aspiration, 20 mL of 0.2% ropivacaine was placed between the posterior knee capsule and the popliteal artery.
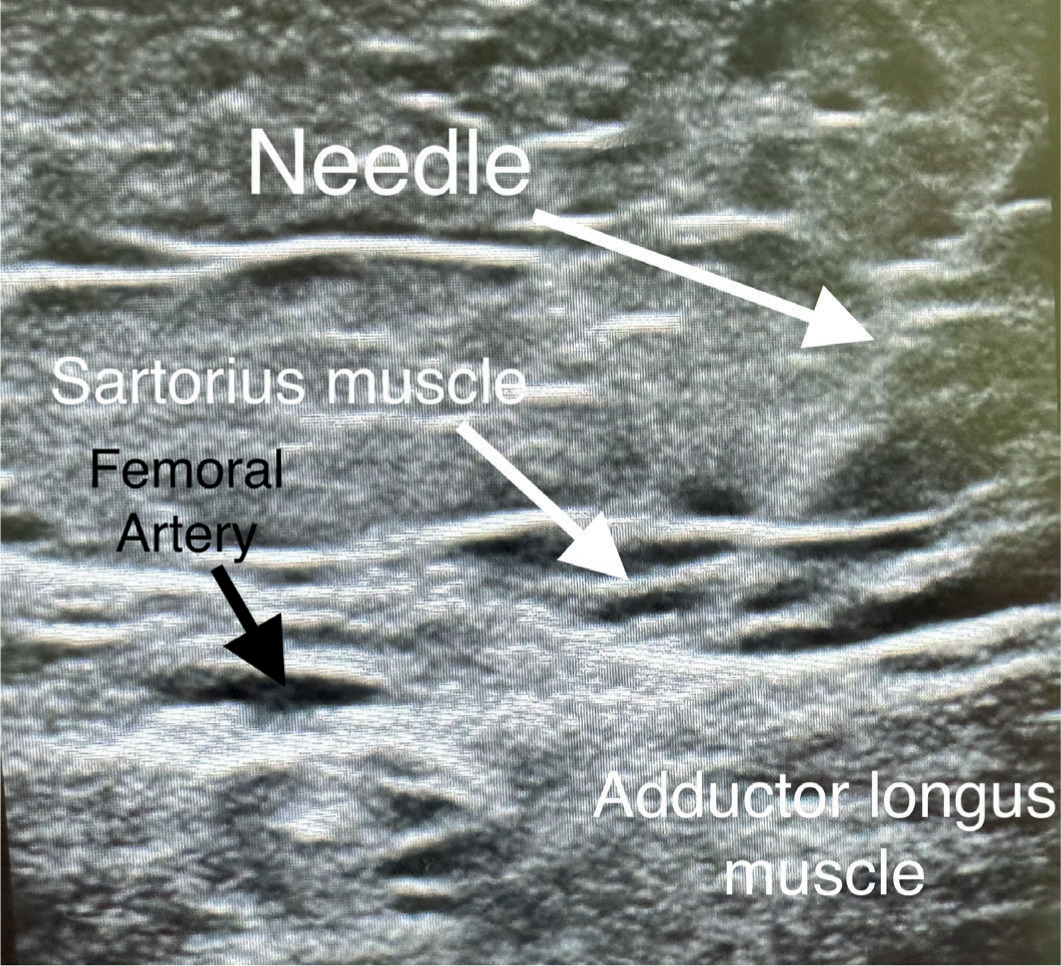
Adductor canal block (Figure 2)
The transducer was placed in a transverse orientation at the middle level of the middle third of the thigh. The femoral artery, sartorius, adductor longus, and vastus medialis muscle were identified. The limits of the femoral triangle and adductor canal were determined by scanning up and down until the medial border of the sartorius muscle meets the medial border of the adductor longus. The scanning distally continued until the adductor longus muscle became shorter in the ultrasound image, and the artery was located in the middle of the sartorius muscle. The needle was inserted in-plane in a lateral to medial direction and advanced towards the femoral artery and saphenous nerve. To reduce the risk of intravascular injection or hematoma, we identified the position of the femoral vein by applying and releasing the transducer pressure as it opens and closes the femoral vein. After the negative aspiration, 1 mL of local anesthetic was injected to confirm the proper injection site. A total of 10 mL of 0.5% ropivacaine was administered.
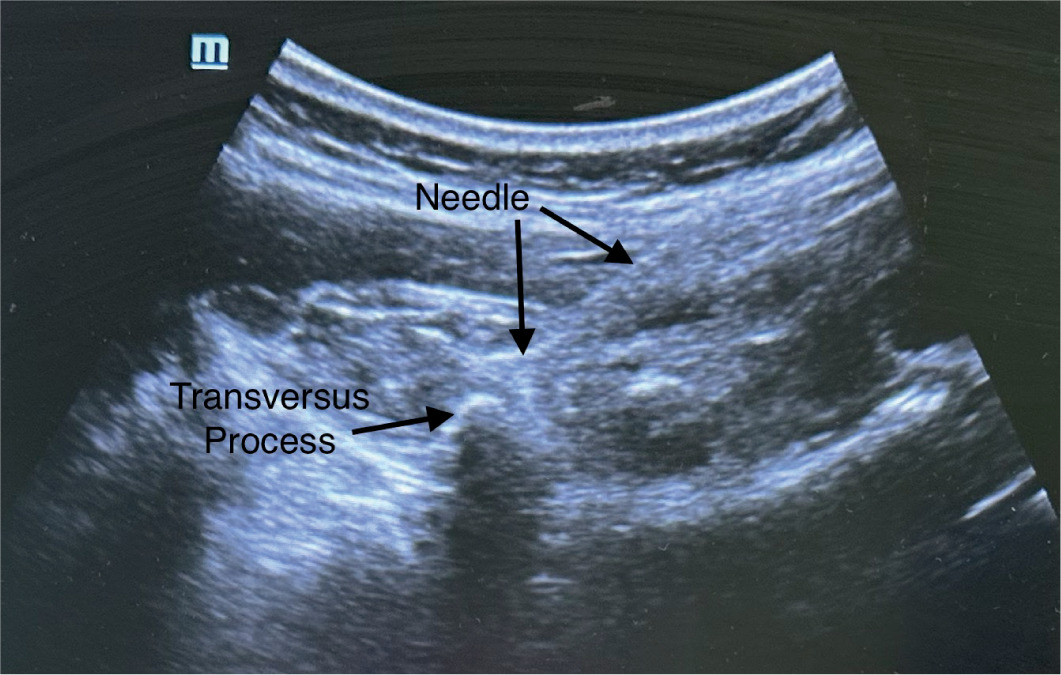
Lumbar erector spinae plane block procedure (Figure 3)
After the spinal anesthesia and before the surgical incision, the erector spinae plane block (ESPB) was performed at the L2 vertebral level. The patient was placed in the lateral position with the operated side up. We used a linear, high-frequency 4–8 Hz probe and a 22-gauge needle (Stimuplex Ultra 360, 50 mm). The transducer was placed in a paramedian sagittal orientation at the level of spinous processes. The needle was inserted in-plane from a cranial to caudal direction until the tip contacted the transverse process. We injected 0.5 mL of 0.9% isotonic saline to confirm the proper injection plane by visualizing the spread deep to the erector spinae muscles and superficial to the transverse process. After the negative aspiration, 0.5 mL kg–1 of 0.2% ropivacaine was placed to ensure the fascial plane between the transverse process and the erector spinae muscle.
Total knee arthroplasty
To minimize the risk of bias associated with varying invasiveness of surgical procedures performed in knees with different types of deformations, only patients with primary osteoarthritis who qualified for a cemented cruciate retaining (CR) TKA were enrolled. The surgeons were blinded to the type of anesthesia used in each case and were instructed to perform a standard TKA procedure. A tourniquet was applied for each surgery, followed by a mid-line incision and parapatellar capsulotomy. Next, the Hoffa fat pad was excised, and osteophyte removal was conducted. Intramedullary guides were used to perform bony cuts for CR-type implants, according to the mechanical alignment technique. The knee kinematics were evaluated using trial components, and if the surgeon was satisfied with joint function, jet lavage was performed before fixing the final implants with bone cement. Once the cement had cured, the joints were flushed with saline, and the wounds were closed. After the dressing was applied, the tourniquet was released. Patellar resurfacing was not performed, and the same type of implant (Stryker Triathlon) was used in all knees. Patients who required an intraoperative decision to convert to a higher level of implant constraint or who underwent ligament releases were excluded from the study. Postoperatively, patients began a passive range of motion exercises and were allowed to walk with weight bearing as tolerated the following day. Typically, they were discharged after three days of rehabilitation.
Postoperative analgesia management
All groups received 1.0 g of acetaminophen, 1.0 g of metamizole, and 400 mg of ibuprofen at the knee closure. Postoperative analgesia included the administration of acetaminophen 1.0 g every 6 hours, metamizole 1.0 g every 6 hours, and ibuprofen 400 mg every 8 hours. Additionally, if the patient’s NRS score was 4 or above, a 5 mg oxycodone bolus injection was administered for rescue analgesia.
Rescue analgesia was administered in the form of intravenous 5 mg oxycodone boluses, rather than patient-controlled analgesia (PCA), for two reasons: to ensure uniformity and control of opioid dosing across all participants, and due to institutional practice standards at the time of study initiation.
Pain was assessed at predefined intervals (4, 8, 12, 16, 20, and 24 hours postoperatively); however, patients were also instructed to report any significant pain between these intervals. Therefore, rescue anal-gesia was available at any time upon patient request.
Trained ward nurses, available 24/7 and operating under standardized analgesia protocols, administered all rescue doses. While we acknowledge the possibility of variability in staff workload, the nurse-to-patient ratio remained constant throughout the study period, minimizing the risk of bias related to delays in rescue analgesia administration.
Outcome measures
Primary outcome
The total opioid consumption within 48 hours after surgery, expressed in milliequivalents of intravenous morphine, was accessed at the orthopedic wards by the residents and fellows, who were blinded to the study.
Secondary outcomes
At all postoperative time points (3, 6, 12, 18, 24, 48 hours after surgery), the pain score was assessed using the NRS score (0 meaning no pain and 10 meaning the worst pain imaginable). Two independent physicians evaluated the subject during the examination. The final score was agreed upon at the end of the examination. The quadriceps strength score was assessed using the Medical Research Council (MRC) Scale for Muscle Strength, where grade 5 means normal muscle strength, grade 4 means movement against gravity and resistance, grade 3 means movement against gravity over (almost) the entire range, grade 2 means movement of the limb but not against gravity, grade 1 means visible contraction without movement of the limb (not existent for hip flexion), and grade 0 means no visible contraction. Two independent physicians evaluated the quadriceps muscle strength during the examination, and the final score was agreed upon at the end of the examination. Blood samples for PLR and NLR were obtained 24 and 48 hours after surgery by nurses who were blinded to the study. Two researchers blinded to the group allocation assessed the outcomes.
Statistical analysis
Statistical analysis was performed using Graph-Pad Prism 10.1.1 (270) software (GraphPad Software Inc. San Diego, CA, USA). The parametric distribution of numerical variables was evaluated using the Shapiro-Wilk normality test. The ANOVA or Kruskal-Wallis test with post hoc Tukey’s or Dunn’s test assessed group differences. Categorical variables were compared with the Kruskal-Wallis test, and an analysis of contingency was compared with Fisher’s exact test. A P-value < 0.05 was considered statistically significant.
Sample size calculation
The sample size was based on our primary hypothesis that the iPACK block with ACB improves pain management compared to the lumbar ESPB and no-block analgesia. The total opioid consumption 48 hours after surgery was the primary outcome variable. Based on our hospital’s retrospective analysis of unpublished data, we assumed a mean total opioid consumption over 48 hours after surgery of 3.0 ± 1.24 (mean ± SD) in the iPACK block with the ACB group and 6.5 ± 3.35 (mean ± SD) in the L-ESPB group. With Bonferroni correction, we calculated a minimal sample of 84 patients for a type I error of 0.05 and a type II error of 0.1, translating to 95% power to detect the difference. Ninety (30 × 3) patients were recruited to facilitate block randomization and account for potential dropouts.
RESULTS
Summary of participation
Of the 110 patients assessed for eligibility, 15 did not meet the inclusion criteria, and 5 refused to participate. The remaining ninety were randomly allocated to three groups and analyzed, as seen in Figure 4. No subjects were lost to follow-up. No clinically relevant differences were apparent from group characteristics, as shown in Table 1.
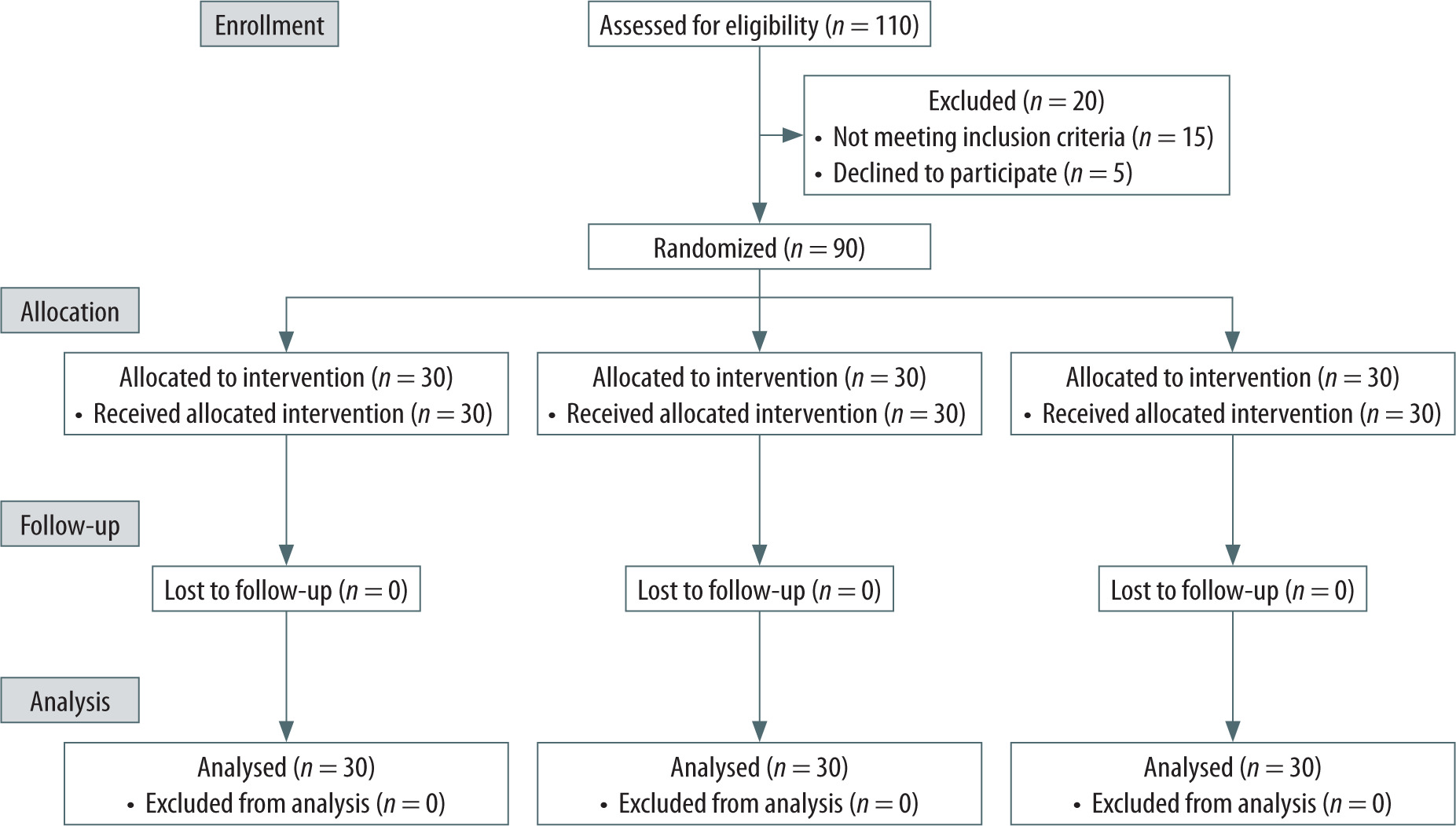
TABLE 1
Baseline characteristics
Primary outcome
The total opioid consumption within 48 hours after surgery, expressed in milliequivalents of intravenous morphine, was significantly lower in the iPACK+ACB group compared to the control group (3.0 ± 3.3 vs. 18.2 ± 4.0, P < 0.001) and in the L-ESPB group compared to the control group (6.8 ± 3.8 vs. 18.2 ± 4.0, P < 0.001). Also, total opioid consumption was lower in the iPACK+ACB group compared to the L-ESPB group (P = 0.0442), as seen in Table 2 and Figure 5.
TABLE 2
Primary and secondary outcomes
Values are mean (SD) or median [IQR]. aP-value compares all three groups. bANOVA or Kruskal-Wallis tests with posthoc Tukey’s or Dunn’s test used to compare means between groups. cP-value compares the control group to the iPACK+ACB group. dP-value compares the control group to the lumbar ESPB group. eP-value compares the iPACK+ACB group to the lumbar ESPB group
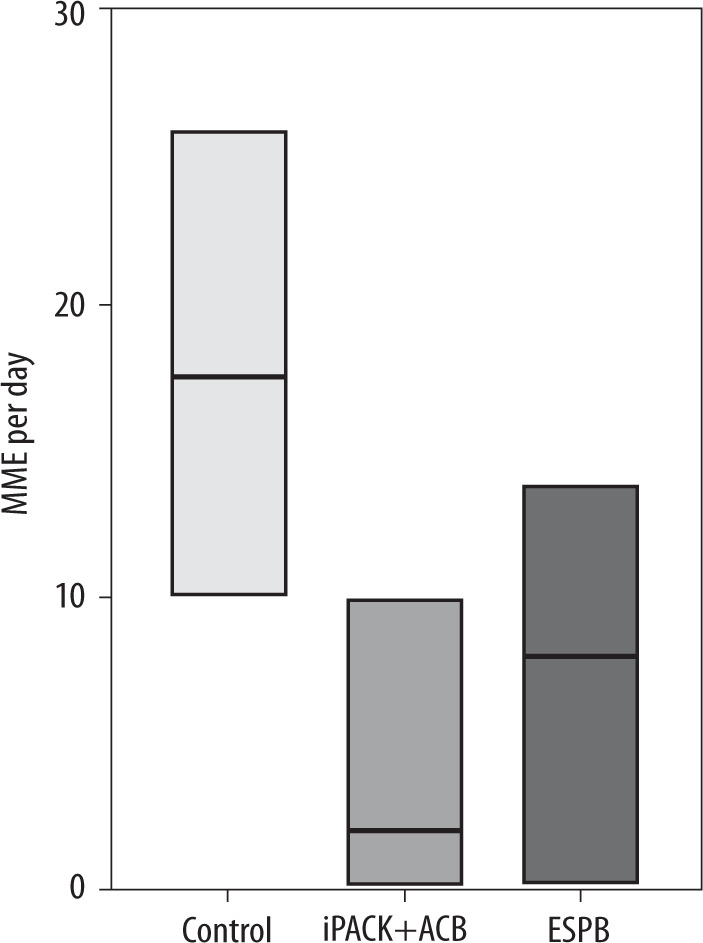
Also, 14 patients in the iPACK+ACB group did not require opioids after surgery, compared to the control group, where all the patients needed opioids postoperatively (P < 0.001), and to the L-ESPB, where only four patients did not require opioids postoperatively (P = 0.01).
Secondary outcomes
The time to first rescue opioid analgesia was significantly lower in the iPACK+ACB group (12.0 ± 1.9) and the L-ESPB group (9.2 ± 1.9) compared to the control group (4.3 ± 1.1) (P < 0.001). The time to first rescue analgesia was lower in the iPACK+ACB block group compared to L-ESPB (P < 0.001).
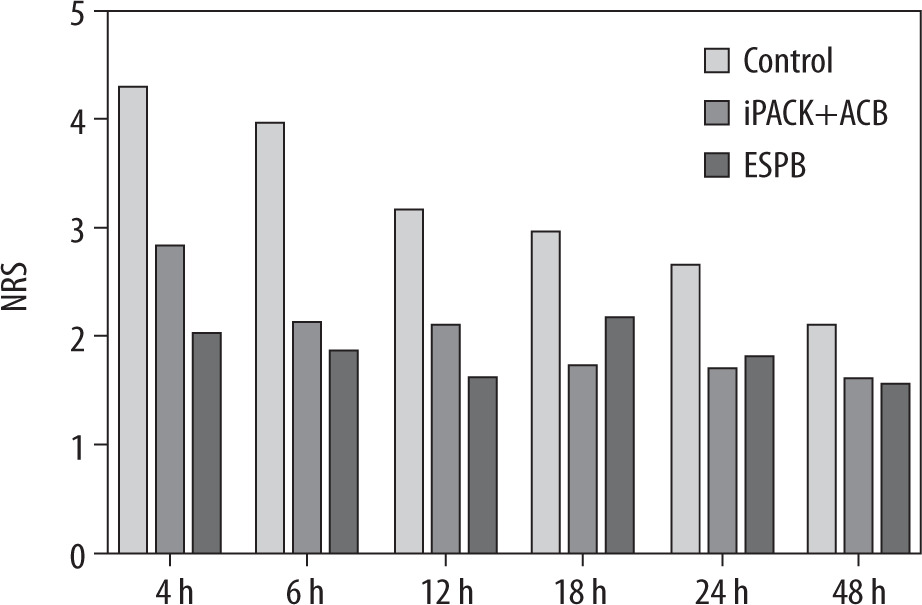
The iPACK+ACB and L-ESPB group patients had lower NRS scores at all time points (4, 8, 12, 16, 20, and 24 hours after surgery) than the control group. The NRS scores 4 hours after the surgery were lower in the L-ESPB group compared to the iPACK+ACB group. The NRS scores did not differ between the iPACK+ACB and the L-ESPB groups at the remaining time points (8, 12, 16, 20, and 24 hours after surgery), as seen in Figure 6.
The NLR and PLR levels did not significantly differ between all three groups at all time points (P > 0.05).
The quadriceps muscle strength measured by the knee extension and hip adduction did not differ between all three groups at all time points (3, 6, 12, and 24 hours after surgery).
DISCUSSION
This double-blinded RCT demonstrated that the ultrasound-guided iPACK block combined with ACB significantly improves pain management following TKA compared to the L-ESPB and a control group receiving no regional block. This is the first study to directly compare the analgesic efficacy of the L-ESPB and the iPACK block with ACB in the context of TKA, addressing a critical gap in the existing literature.
Given the limited evidence available on the effectiveness of L-ESPB in TKA, we sought to investigate its analgesic efficacy by comparing it to a control group without regional anesthesia and to one of the most established pain management techniques in TKA – the combination of the iPACK block with ACB [11, 12]. The rationale for including the iPACK+ACB group was based on its known ability to provide comprehensive analgesia, targeting both anterior and posterior knee pain while minimizing motor blockade [13]. By comparing L-ESPB to this combination, we aimed to assess whether L-ESPB could offer comparable analgesic benefits with a more straightforward and potentially more efficient technique [14].
We chose the endpoint of 48-hour opioid consumption for several reasons. First, opioid consumption is widely accepted in the literature as an indirect but objective measure of postoperative pain management efficacy [15]. It is also a highly relevant clinical outcome, as reducing opioid use is a critical goal in contemporary pain management strategies due to the risks associated with opioids, including addiction, respiratory depression, and other side effects [16]. In addition, the 48-hour window was selected because it typically covers the most intense period of postoperative pain following TKA, when patients are most likely to rely on opioids for pain control. Beyond this time frame, patients may transition to non-opioid analgesics as the acute phase of pain subsides [17].
Our study demonstrated that combining the iPACK block with the ACB resulted in a four-fold reduction in total opioid consumption compared to the control group. Additionally, this technique significantly prolonged the time to the first request for rescue analgesia, extending it up to 12 hours postoperatively, which aligns with findings from previous studies investigating the efficacy of the iPACK block with ACB in TKA [18, 19]. Notably, nearly 50% of the patients in the iPACK+ACB group did not require any opioids following surgery. Furthermore, total opioid consumption was lower in the iPACK+ACB group compared to the L-ESPB group. These findings are consistent with prior studies that have evaluated the analgesic benefits of the iPACK block in combination with the ACB for TKA [5], further supporting its efficacy in reducing opioid requirements and enhancing postoperative pain management.
Our study demonstrated that the L-ESPB at the L2 level resulted in a two-fold reduction in total opioid consumption compared to the control group and significantly prolonged the time to first opioid rescue analgesia, extending it to a median of nine hours. Given the lack of prior studies specifically investigating L-ESPB in TKA, we compared our findings to those from studies evaluating L-ESPB in total hip arthroplasty (THA). Our results regarding extending time to first rescue analgesia are consistent with most trials examining L-ESPB in THA [20, 21]. However, it is essential to note that some studies have reported a lack of efficacy of L-ESPB in THA. For instance, Lennon et al. [22], in a randomized trial involving 64 patients receiving ultrasound-guided L-ESPB with ropivacaine or saline, found no significant differences in pain scores between the groups. Similarly, Chan et al. [23] did not observe a clear analgesic benefit of L-ESPB following THA. These contrasting findings highlight the variability in outcomes associated with L-ESPB and underscore the need for further research to clarify its role in perioperative pain management across different surgical contexts [24].
The innervation of the knee joint is complex, arising from both the lumbar and sacral plexuses. According to Lim et al. [25], the spread of local anes thetic following a single injection of the ESPB covers an average of 1.7 spinal levels in cadaveric models and up to 4.7 levels in healthy volunteers, with a mean sensory coverage of 5.4 spinal levels. Given this, it is likely that the L-ESPB administered at the L2 spinal level does not provide complete coverage of both the lumbar and sacral plexuses, which could explain the suboptimal pain control observed in comparison to the iPACK block combined with the ACB in our study following TKA. This incomplete blockade may limit the efficacy of L-ESPB in fully addressing the complex innervation of the knee joint, suggesting that further research on two-level ESPB techniques is needed to optimize postoperative analgesia in TKA [3].
Additionally, our study found that neither the iPACK block with ACB nor the L-ESPB adversely affected quadriceps muscle function, in contrast to other regional anesthesia techniques such as the femoral nerve block or fascia iliaca block [26, 27]. This preservation of motor function is critical for promoting early mobilization and functional recovery following TKA. The iPACK block with ACB and L-ESPB appears to facilitate postoperative rehabilitation, a finding that aligns with previous research on the iPACK block with ACB [18]. Our results are similar to those of other studies regarding the iPACK block with ACB [13] and L-ESPB in THA [20, 21]. However, to our knowledge, no studies to date have specifically evaluated the impact of L-ESPB on pain management or functional recovery in TKA patients. This highlights the need for further clinical trials to establish the efficacy and role of L-ESPB in the context of TKA.
Our study demonstrated that the iPACK block with ACB and the L-ESPB have a comparable impact on modulating the surgical stress response. These findings are consistent with previous studies investigating the effects of regional anesthesia on the physiological stress response to surgery [28, 29]. As highlighted in earlier research, both ESPB and the iPACK block with ACB reduce the stress response induced by surgery and opioid administration [30]. Regional anesthesia techniques are known to attenuate the perioperative sympathetic and inflammatory responses triggered by increased vascular permeability, elevated blood flow, and leukocyte aggregation [31]. Markers such as NLR and PLR, derived from complete blood count parameters, are reliable indicators of systemic inflammation. These ratios have prognostic significance in assessing inflammation and predicting mortality and morbidity [32]. Our results confirm that regional anesthesia plays a role in mitigating the inflammatory response to surgical stimuli, as reflected by reductions in NLR and PLR, compared to general anesthesia, which has been associated with a more pronounced inflammatory response [30, 33]. This reduction in inflammation suggests that by modulating the body’s stress response, regional anesthesia may improve postope rative outcomes and recovery.
LIMITATIONS
Our results should be interpreted cautiously, considering several limitations of the study. First, we used a relatively large volume of local anes thetic, which may increase the risk of local anesthetic systemic toxicity (LAST). However, no cases of LAST were observed in this trial. Second, we followed participants for 48 hours postoperatively, based on evidence from multiple studies indicating that postoperative pain typically peaks during this period. Nevertheless, a longer follow-up duration may be required to capture all aspects of recovery, such as longer-term pain management and functional outcomes.
Additionally, we did not monitor key parameters beyond 48 hours, such as longitudinal measurements of the NLR and PLR, sensory block characteristics, block duration, or common adverse effects, including nausea, vomiting, constipation, and pruritus. We also did not evaluate hospital discharge times, which could provide insights into the broader impact of regional anesthesia on recovery.
Future research should address these limitations by exploring the optimal dosing of long-acting local anesthetics and the most effective spinal level for L-ESPB in TKA. Such studies are necessary to identify the best analgesic strategies that balance efficacy, safety, and recovery outcomes in this patient population.
CONCLUSIONS
Based on our findings, the ultrasound-guided iPACK block combined with the ACB provides superior postoperative analgesia to the ultrasound- guided L-ESPB at the L2 level. Both the iPACK block with ACB and the L-ESPB were associated with reduced total opioid consumption and a prolonged time to first rescue opioid administration. Additio nally, as motor-sparing techniques, both blocks facilitate early mobilization and promote functional recovery.
However, further research is warranted to optimize the use of L-ESPB in patients undergoing TKA, specifically in determining the most effective spinal level and local anesthetic dosage to maximize anal-gesic efficacy while minimizing adverse effects.