
Dear Editor,
Polytrauma represents a global health crisis, accounting for up to 35% of emergency department admissions and standing as the leading cause of long-term disability. Furthermore, inadequate management of critically ill polytrauma patients ranks as the third most common cause of mortality [1]. These critically ill patients often require general anesthesia and systemic opioids to provide analgesia and ensure patient comfort during and after surgical treatments. However, regional anesthesia may play a role in managing these complex scenarios by enhancing perioperative analgesia [2].
In thoracic trauma, posterior rib fractures are common and painful, impairing respiratory function and often requiring admission to intensive care. In these cases, regional anesthesia combined with multimodal systemic analgesia has consistently demonstrated reduced pain and improved oxygenation. Strategies for managing analgesia in chest wall trauma include epidural, intercostal, and paravertebral blocks; additionally, single-shot or continuous fascial plane blocks such as the serratus anterior plane (SAP) block have shown optimal results for post-traumatic chest wall analgesia [3–5].
Femoral fracture is a very common finding in major trauma. Though there is no uniformity within the current published evidence, it has been widely demonstrated that the early surgical reduction of femoral fractures reduces short- and long-term complications. Furthermore, the regional anesthesia approach for such a procedure may eliminate the risks associated with surgery under general anesthesia [6]. Fem-oral nerve block (FNB), obturator nerve block (ONB), and sciatic nerve block are the most widely used analgesic techniques for this type of fracture [7]. Of additional importance, the regional approach makes it potentially possible to shorten the time of the operation, while also accepting clinical conditions that would make general anesthesia a suboptimal choice [6].
Additionally, regional anesthesia significantly reduces the intensity of acute pain in traumatic injuries [1] and improves long-term outcomes through reducing the intensity of acute pain, which is a major predictive risk factor of chronification of traumatic pain. Currently, opioid misuse is reported in nearly one-third of patients with chronic pain [8]. Opioid-free anesthesia (OFA) allows adequate anesthesia without administering intraoperative opioids. In contrast, opioid-sparing anaesthesia is a technique that, through the use of multimodal analgesia nonopioid adjuncts and perioperative regional anesthesia, can consistently reduce opioid consumption [9].
We report a case of successful application of multiple, combined regional anesthesia techniques for intraoperative anaesthesia and postoperative analgesia in a polytrauma patient. Written consent for the publication of this case report has been obtained from the patient.
A 22-year-old man suffered poly-trauma after a traffic accident and was brought to our institution’s (University Hospital Campus Bio-Medico, Rome, Italy) emergency department by the emergency services. Upon arrival, the patient was alert and cooperative (CCS 15) and reported pain in the thoracic spine and left lower limb. He was hemodynamically stable and breathing easily. The abdomen was non-tender. Urgent hematological and chemical examinations were ordered; they showed a hemoglobin level of 14.4 g dL–1, leukocytosis, normal coagulation profile (INR 1.14), and elevated hepatic enzyme levels.
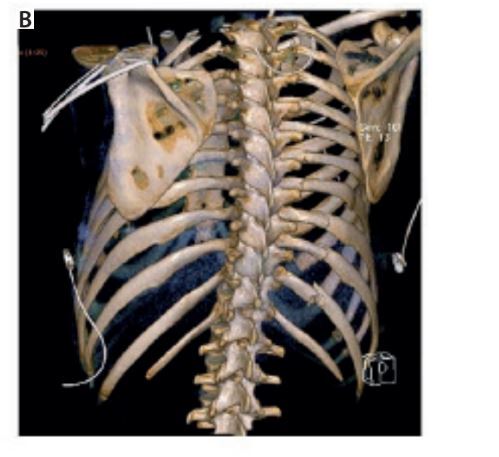
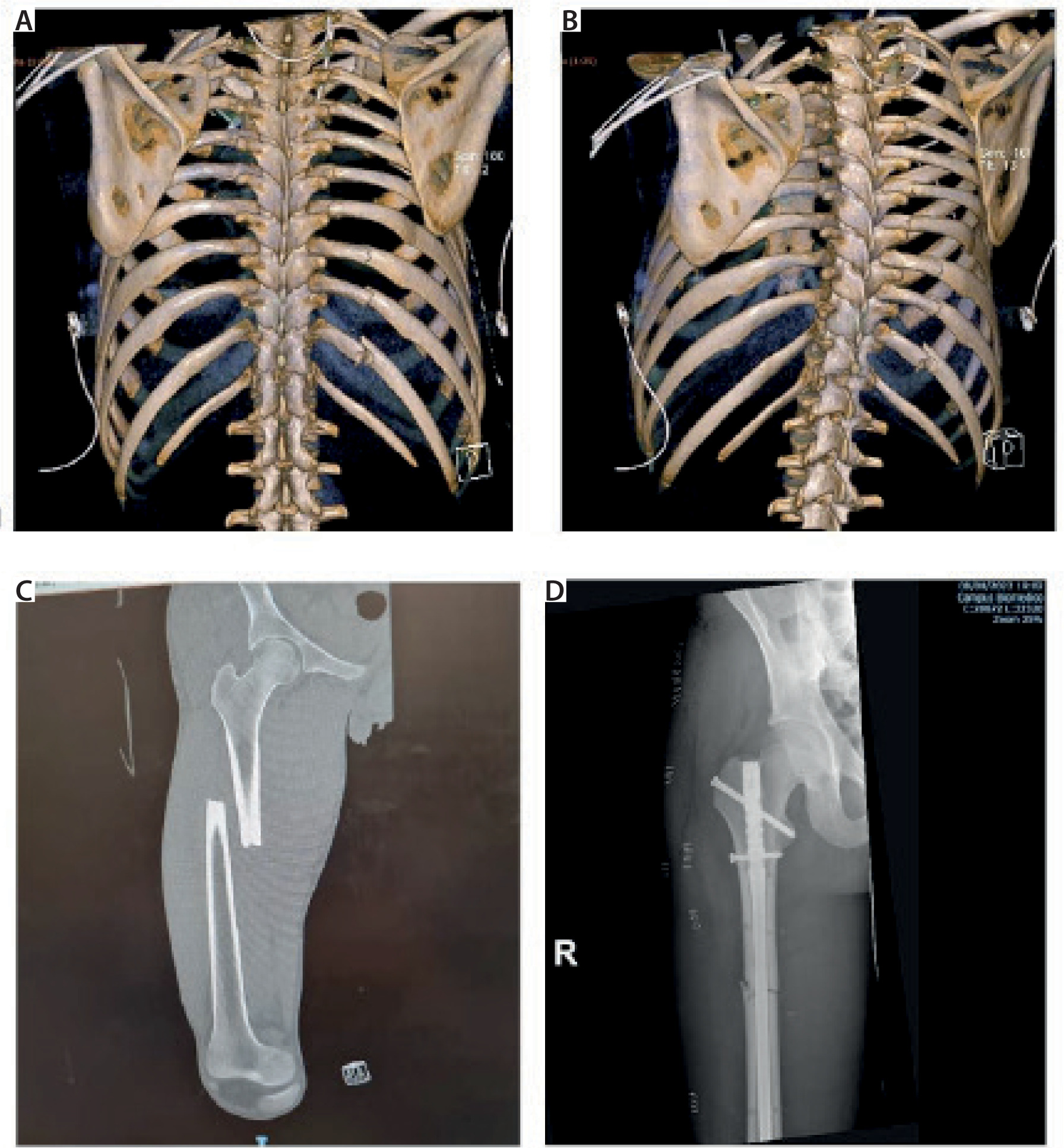
The initial computed tomography (CT) scan revealed: a severe pneumomediastinum; a large right-sided pneumothorax with partial collapse of the lung, small pneumothorax on the left in the apical and anterosuperior region; multiple rib fractures bilaterally, specifically ribs I, II, III, and IV on the left and ribs II, III, IV, VI, VII, and XII on the right (Figures 1A and 1B); fracture of the upper third of the right scapula and right sternoclavicular subluxation; a hepatic subcapsular hematoma at segment VI (approximately 13 × 6 mm); evidence of suspected right renal hematoma; a compound fracture of the left transverse process (Th1); and a fracture of the middle third of the right femoral diaphysis (Figure 1C).
FIGURE 1
A, B) 3D chestcomputed tomography reconstruction with 2 perspectives showing posterior rib fractures. C, D) X-ray of femur fracture on admission to the emergency room and after surgical reduction (one week later)
We consulted several specialists. The thoracic surgeons placed a right chest drain at the level of the third intercostal space at the midclavicular line to drain the apical pneumothorax, and orthopedic surgeons recommended mandatory supine decubitus, skin traction of the right lower limb, antithrombotic prophylaxis, and reduction and synthesis of the right femoral diaphysis fracture.
However, over the subsequent days, the patient developed progressive anemia, and general anesthesia was required for abdominal surgery (hepatic packing) to treat the ra pidly expanding hepatic hematoma. The patient was admitted to the intensive care unit (ICU) to manage hemodynamic instability, and had multiple units of concentrated blood products transfused.
Eight days after hospital admission, he underwent femur fracture fixation through the placement of an intramedullary rod (Figure 1D). Regional anesthesia was performed for both anesthetic and analgesic purposes. The patient was premedicated with 0.1 mg of fentanyl i.v. and received the following ultrasound-guided blocks: FNB and subgluteal sciatic nerve block, both using a mixture of 0.75% ropivacaine and 2% mepivacaine in 10 mL doses, as well as ONB with 5 mL of the same mixture. Additionally, an SAP block was administered at the fourth intercostal space using 20 mL of ropivacaine 0.25%. The patient underwent the procedure in a supine position on a rigid traction table, which caused significant pain before the block (NRS score of 8) but was noted to be significantly less painful following the block (NRS score of 2). Throughout the surgery, the patient was under deep sedation with a continuous intravenous infusion of propofol and maintained spontaneous breathing using a Venturi mask (FiO2 0.5).
At the end of the surgery, the patient returned to and was discharged from the ICU on the same day and was subsequently transferred to the Emergency Medicine ward of our hospital for further treatment. We obtained written consent from the patient for the publication of this case report.
Management of polytrauma requires a multimodal approach with prioritized therapeutic interventions aimed at preventing the worsening of clinical conditions [10]. Adequate pain control can be difficult to establish in the acute injury patient [11]. The priorities in trauma patient management are resuscitation, assessment, and treatment of life-threatening injuries [12]. However, pain associated with injury is often under-treated, which leads to increased discomfort and unnecessary suffering [13]. Musculoskeletal injuries are common in trauma patients, and a regional analgesic approach can reduce the use of opioids and sedatives, decreasing associated side effects and hospitalization length [14]. Surgical procedures in patients who are not fully optimized are frequently postponed due to reasonable concern for complications associated with general anesthesia and possible difficulties in airway management and weaning from mechanical ventilation. Appropriate management of regional anesthesia can avoid these complications and allow for expedited care. Use of several nerve blocks has been well established for the treatment of single injuries, such as SAP block for multiple rib fractures, FNB combined with obturator nerve block (OBN) for anal-gesia of femoral head fractures, and inter-scalene brachial plexus block for humerus fractures [15–17].
Recent high-level guidance – namely the joint ASRA-ESRA recommen dations on antithrombotic mana gement for regional anaesthesia, the ESAIC- ESRA evidence-based guideline on regional techniques in surgical patients, and the 2025 ESTES European polytrauma consensus – collectively endorses a multimodal, guideline-driven analgesic strategy and stresses meticulous patient selection when multiple ultrasound-guided blocks are contemplated; concordantly, contemporary adult case series document that simultaneous peripheral nerve blocks (e.g., combined erector spinae, serra-tus anterior, and femoral catheters) can deliver safe, opioid-sparing analgesia across multiple injury sites without increasing the risk local-anesthetic systemic toxicity [18–20].
Our intention is to demonstrate that the combination of several nerve blocks can allow for safe and effective management of the polytrauma patient. This approach was chosen to make the surgical reduction of the femur fracture possible while avoiding general anesthesia for the third time in the span of a few days. The patient had benefited in at least two ways by avoiding another general anesthesia: first of all, for this last surgery, involving the femur, it eliminated the need for mechanical ventilation (beneficial in the context of recent multiple rib fractures) [21]; secondly, it eliminated the need for opioid analgesia, potentially reducing the risks associated with its prolonged use [22]. This case thus exemplifies how locoregional techniques can contribute to lower use of opioids [23, 24]. Furthermore, the main problem with this operation was the management of the patient’s ventilation, as the traction bed for surgical reduction of the femur forces an awkward and constricted position, not facilitating ventilation in an already compromised respiratory condition. Using a combination of two regional techniques, the pain control and preservation of respiratory function outcomes were excellent and there were no complications.
A large volume of anesthetic was not used for lower limb anesthesia, and the band block was performed only on one side of the thorax. Using relatively small doses of local anesthetics helped minimize the risk of local anesthetic systemic toxicity (LAST). Although rare, LAST is a critical event that can lead to adverse outcomes.
Because this case report concerns a young and cooperative trauma patient without comorbidities or coagulopathy, who was managed in a high-volume tertiary center with advanced regional-anesthesia expertise, the external validity of this multi-modal block strategy is intrinsically narrow; its routine application should therefore be approached with caution – particularly in elderly, hemodynamically unstable, or coagulopathic patients, for whom alternative anesthetic plans may be safer and more reliable. At the same time, it must be emphasized that the last surgery was limited to the femur, so if there were multiple sites involved (multiple fractures), general anesthesia would have been more appropriate for the patient’s comfort.
In conclusion, it is clear that much work must be done in the future to understand the best anesthetic management method for complex poly-trauma patients, and further research is needed to determine its optimal use. Regional anesthesia was undoubtedly a valuable aid in managing poly-trauma of a young, collaborative, and non-comorbid patient who underwent orthopedic surgery at a highly specialized center. Further prospective studies or multicenter trials are warranted to define the safety profile, optimal block combinations, and patient- selection criteria for extensive regional- anesthetic strategies in multi-injury adult trauma.