
Thanks to anesthesia, surgical procedures can be performed. However, as detailed mechanisms of anesthetic activity are not yet fully understood, there is ongoing debate about their neuroprotective and neurotoxic effects. Both of them can be assessed by cognitive testing and neuromarkers. Postoperative neurocognitive disorders (PND) are a serious problem in patients undergoing both elective and emergency surgery with local and general anesthesia, including postoperative delirium, which is the most severe and life-threatening representation of PND. A very interesting summary of the state of the art in this topic was provided by Pecorella et al. [1], who outlined the broad pathophysiological and diagnostic background. One of the interesting issues presented in this analysis was the discussion on the possible superiority of the type of anesthesia chosen for the patient. The general conclusion drawn from these comparisons is that in the case of anesthesia for surgery with ischemia-reperfusion pathology, sevoflurane-based anesthesia seems to be superior, whereas in terms of PND occurrence, propofol-based procedure may provide better cognitive outcomes. Despite years of gathering clinical experience, the quality of the anesthesiological approach remains crucial for optimization of patients’ well-being in the immediate postoperative period.
Changes in patients’ cognition may be tested using various clinical tests. For the purpose of our study we chose the Montreal Cognitive Assessment (MoCA). The MoCA assesses the following cognitive domains: attention and concentration, executive functions, memory, language, visual constructional skills, conceptual thinking, calculations, and orientation. The MoCA has already been used in young [2] and older populations [3]. It is considered to be a better tool for cognitive assessment than the Mini-Mental State Examination (MMSE), which is used more extensively [3].
In our study, the MoCA results were related to the markers of neuroinjury: glial fibrillary acidic protein (GFAP), neurofilament light chain (NFL), tau protein (tau), and ubiquitin C-terminal hydrolase L1 (UCH-L1). These proteins were chosen because they had already been successfully used as disease markers in patients with numerous neurological pathologies.
GFAP is a type-III intermediate filament expressed in mature astrocytes in the gray and white matter, the cerebellum, the subventricular and subgranular zones, and Müller cells in the retina. The astrocytes in the central nervous system (CNS) are responsible for the proper functioning of the blood-brain barrier, maintaining metabolic homeostasis. In traumatic brain injury, blood GFAP levels correlate with clinical severity. It may be used for predicting multiple sclerosis (MS) progression and in subtle injuries of the CNS [4]. Gattringer et al. [5] suggested the serum GFAP was an indicator of acute rather than chronic pathology after they had tested its usage in small subcortical infarcts and investigated the correlation with the size of the cerebral lesion. It shows some potential for Alzheimer’s disease (AD) screening and future cognitive status prediction [6].
NFL is a promising marker of neuraxial injury, which may be detected in both cerebrospinal fluid and blood. Its usefulness was observed in MS, in which the marker correlated with relapses and disability. Although Aktas et al. [7] found no clear relation to cognition and neuropsychiatric symptoms in stable MS, Bergman et al. [8] considered NFL to be a valuable sensitive and specific marker of white matter axonal injury. NFL outperforms other neuromarkers, e.g. plasma amyloid β and total tau, in differentiating AD patients from healthy subjects [9].
Tau is a microtubule-associated protein in neurons helping to maintain their stable construction. Its abnormal phosphorylation results in self- aggregation with reduced microtubule stability. This leads to neuronal apoptosis, observed e.g. in AD and tauopathies. It is less known that tau protein in dendrites is responsible for hippocampal synaptic plasticity [10].
UCH-L1 is a widespread protein, mainly found in the healthy brain tissue and in several forms of cancer, and it requires the maintenance of axonal integrity. The dysfunction of this enzyme with the loss of its solubility and its further aggregation with the subsequent reduction of its enzymatic activity is observed in neurodegenerative diseases, e.g. AD and Parkinson’s diseases [11].
The set of these markers covers both neuraxial and glial injury. The inflammatory reaction seems to be a connecting link between PND and AD.
As age is a considerable risk factor for the cognitive impairment in the general population [12] and postoperatively [13], its role as a possibly influential factor responsible for the perioperative differences in the MoCA results and neuromarkers levels was evaluated.
The changes occurring in specific patient sub-populations subjected to particular types of surgical procedures are still less intensively studied issues in the current literature. This is especially important as the early postoperative period is gaining more interest among researchers due to the increasing number of one-day hospitalizations. In order to improve our knowledge in this field, we formulated the following study aims: 1) to compare the propofol and sevoflurane-based schemes of anesthesia in terms of the early perioperative MoCA performance and the levels of neuroinjury markers in women after gynecological laparoscopic procedures; 2) to investigate the possible influence of age on the MoCA and the levels of neuroinjury markers.
METHODS
Our study was approved by the Bioethics Committee at the Poznań University of Medical Sciences, consent number: 453/20.
Groups of patients
The patients scheduled for elective gynecological laparoscopic procedures were divided into two groups according to the type of anesthesia administered: propofol-based anesthesia (PBA) and sevoflurane-based anesthesia (SBA). The patients were randomly assigned to the PBA or SBA group during the pre-operative interview by means of the envelope method. They were tested in the preoperative period and within 24 hours after the surgery.
Qualifying criteria:
a) female, age > 18 years, eligible for laparoscopic gynecological procedures;
b) American Society of Anesthesiologists (ASA) physical status/risk category I, II, or III;
c) native speakers of Polish;
d) informed written consent to participate in the study;
e) at least 8 years of mandatory education;
f) Beck Depression Inventory (BDI) < 14 points [14].
The following exclusion criteria were adopted:
a) non-compliance with the inclusion criteria;
b) concomitant severe metabolic conditions, including: decompensated diabetes with a glycated hemoglobin level (HbA1c) of ≥ 7%; thyroid conditions with levels of thyroid hormones and thyroid-stimulating hormone above the normal range;
c) concomitant severe, unstable cardiovascular and pulmonary conditions;
d) concomitant anemia (hemoglobin and hematocrit levels below the normal range);
e) concomitant severe kidney and liver conditions (diagnosed and specified in medical documentation by internal medicine specialists);
g) a history of severe neurological incidents, including cerebrovascular incidents, CNS injury, cerebral tumor or cerebral tumor excision, meningitis and/or encephalitis;
h) addictions to:
– alcohol – conforming to the diagnostic criteria of alcohol use disorders (AUD) (in compliance with DSM-5) [15],
– narcotics,
– other psychoactive substances and medication;
i) diagnosed and treated mental conditions;
j) illiteracy;
k) unaided auditory or visual impairment;
l) pain at the 4+ level on the Numerical Rating Scale (NRS) scale at rest and > 5 points when coughing in the post-operative period.
Anesthesia protocol
Each of the patients had a pre-operative interview one day before the surgery. The patients were premedicated with oral midazolam (Dormicum, Roche Polska Sp. z o.o. Poland) at a dose of 0.1–0.15 mg kg–1. Anesthesia in both groups was induced intravenously with fentanyl (Fentanyl WZF, WZF Poland) at a dose of 2–3 μg kg–1 and with propofol (Propofol 1% MCT/LCT Fresenius, Fresenius Kabi Deutschland GmbH) at a dose of 1.0–2.5 mg kg–1. The patient was intubated orally after muscle relaxation with rocuronium bromide (Roqurum, Jelfa, Poland) at a dose of 0.6 mg kg–1. In the PBA group, anesthesia was maintained with further propofol infusion as follows: an initial intravenous infusion of 10 mg kg–1 h–1 for 10 minutes, followed by a 10-minute infusion of 8 mg kg–1 h–1, and finally an infusion of 4–6 mg kg–1 h–1. In the SBA group anesthesia was maintained with sevoflurane (Sevorane, AbbVie Polska Sp. z o.o., Poland) administered at a dose allowing for age-adjusted MAC 0.8–1.0. In both groups, additional doses of fentanyl and rocuronium bromide were administered according to the patients’ individual needs. During the anesthesia, the patients received volume-controlled ventilation, with individually adjusted parameters of tidal volume, breathing rate per minute and positive end-expiratory pressure. The tracheal tube was removed once the residual neuromuscular block had been reversed with neostigmine (Polstigminum, Teva Pharmaceuticals Polska Sp. z o.o., Poland) at 20 µg kg–1 i.v., after prior administration of atropine (Atropinum Sulfuricum WZF, WZF, Poland) at a dose of 0.5–1.0 mg i.v. Anesthesia was induced with Maquet Flow-I anesthesia machines (Getinge AB, Sweden).
The patients were monitored for the following parameters: electrical activity of the heart (ECG), non-invasive arterial blood pressure measured every 5 minutes, hemoglobin saturation with oxygen measured by pulse oximetry (SpO2), capnometry and capnography monitored continuously. Detailed ventilation parameters were measured with the spirometer system of a ventilator and gas sensors. Additionally, standard measurements were taken: body temperature (electronic thermometer), depth of anesthesia (Bispectral Index – BIS), which allowed for adequate titration of propofol and sevoflurane, to maintain the recommended range of 40–60, and muscle relaxation (train of four – TOF).
After the surgical procedure the patients were transferred to the recovery room for further monitoring and treatment. Once they had achieved at least 9 points on the 10-point Aldrete scale, they were transferred to the department to which they had initially been admitted.
Analgesia was initiated with a preoperative intravenous administration of 1.0 g of acetaminophen (Paracetamol B. Braun, B. Braun Melsungen AG, Germany), with subsequent intravenous administration of metamizole (Metamizole Kalceks, AS KALCEKS, Latvia) at a dose of 1.0 g. The postoperative wound was infiltrated by the operator with a 0.25% solution of bupivacaine administered at a dose of 30– 50 mg (Bupivacainum Hydrochloricum WZF 0.5%, WZF, Poland). Further doses of acetaminophen and metamizole were administered at minimum intervals of 6 hours. The patients who experienced pain exceeding NRS 4 points received oxycodone (Oxycodone Molteni, L. Mol-teni & C, Italy) intravenously in fractionated doses of 1–2 mg to alleviate the pain.
Laboratory tests
Blood was sampled from peripheral veins – first the day before the surgery, then 24 hours after surgery.
The blood count was analyzed with a Sysmex XN-1000 analyzer. C-reactive protein was analyzed with a Cobas C 501 device. In order to analyze the levels of blood neuromarkers, blood was sampled, and the acquired plasma was stored at 70°C for further analysis. The neuromarkers were detected with BIORBYT ELISA kits. The analyses were conducted according to the producers’ guidelines. The VICTOR3 automatic reader was used to read the results (Perkin Elmer, USA). The absorbance was read at a wavelength of 450 nm. A computer coupled with the reader using the KCJR program automatically plotted linear, logarithmic, or semi-logarithmic curves based on the light absorbance read from the tested wells and wells with known concentrations of standards, which were used to calculate the cytokine concentration in the tested samples.
Psychometric evaluation
This research employed screening scales devised to detect depression and alcohol addiction, as well as cognitive function tests. Pain levels were assessed with the NRS 0–10 points.
Depression screening
Patients with diagnosed depression were excluded from the study. The Polish version of the BDI was applied to screen the patients for potential undiag-nosed depression [14]. The inventory is composed of 21 questions, each with 4 answer options scored from 0 to 3 points. The patients were asked to select the option which best reflected their mental state. The lowest possible score in the inventory was 0 points, whereas the highest was 63 points. A score of ≥ 14 points indicated depression. The patients who scored ≥ 14 points were further diagnosed for depression and offered therapeutic interventions
Alcohol abuse screening
In order to detect any alcohol use disorders (AUD), the DSM-5 classification of mental disorders criteria was applied, which included eleven diagnostic criteria [15].
Neuropsychological testing
The cognitive tests were conducted by licensed psychologists in a quiet room, ensuring appropriate levels of safety, confidentiality, and anonymity for the patients. The neuropsychological tests were carried out on the day before the surgical procedure and within the first 24 hours following the surgery only if the patients stated that their pain was less than 4 points on the NRS. The tests were made several hours after blood sampling so that no potential emotional response triggered by it would affect their results.
The MoCA was applied in the study. The psychologist administering the MoCA was blinded to the type of anesthesia used in the study. The following cognitive functions can be assessed with this scale: short-term memory, visuospatial functions, executive functions, language functions, verbal fluency, attention and concentration, conceptual thinking, calculation skills, abstraction and allo-psychic orientation. The test takes approximately 10 minutes to complete. The maximum score is 30 points. A score of at least 26 points means the result is correct [16].
Statistical analysis
The normal distribution of the features analyzed in the study was checked with the Shapiro-Wilk test. Levene’s test was used to determine the homogeneity of variance. For the t-test with sample sizes n1 = 29 and n2 = 32, for a medium effect size (d = 0.5) the statistical power is 0.48, and for a large effect size (d = 0.8) the power is 0.87. The characteristics of the research groups were compared with the t-test for independent variables or the Mann-Whitney U test when the assumptions regarding the normal distribution or homogeneity of variances were not met. The power of the Mann-Whitney U test (n1=29 and n2=32) for a medium effect size (d = 0.5) is 0.46, and for a large effect size (d = 0.8) it is 0.85. The occurrence of prolonged bradycardia or hypo-tension was compared between the groups with the χ2 test, the power of which for a medium effect size (d = 0.3) is 0.54, and for a large effect size (d = 0.5) is 0.95. The likelihood ratio test (G-test) was applied to assess the relationship between the level of education and the variants of anesthesia, as in this case the assumptions for the χ2 test were not met [17]. The statistical significance of changes in the MoCA test values and the tested markers between the first and second measurements was evaluated with the Wilcoxon test. The power of this test for the effect size d = 0.5 was 0.82 and 0.85 for n1 = 29 and n2 = 32, respectively. Spearman’s correlation was used to assess the relationship between the patient’s age and changes in the values of the MoCA test and individual markers. The power of this test for a medium effect size (d = 0.3) was 0.34 (n1 = 29) and 0.37 (n2 = 32), and for a large effect size d = 0.5 was 0.78 (n1 = 29) and 0.82 (n2 = 32).
The calculations were performed using Statistica and G*Power software (Dell Inc. (2016). Dell Statistica (data analysis software system), version 13. soft-ware.dell.com.) [18].
RESULTS
Study participants
79 patients were invited to participate in the study. Of these, 61 patients met the inclusion criteria and were included in the study. Eighteen patients were excluded due to a high score on the BDI, suggesting the coexistence of depression. Seven patients were excluded due to a low score on the MoCA (2 patients with a low score on the BDI also had a low score on the MoCA). One patient was excluded due to baseline anemia. One patient withdrew her consent to participate in the research. Finally, 29 patients were included in the PBA group and 32 patients in the SBA group.
Demographic data
Age and body mass index
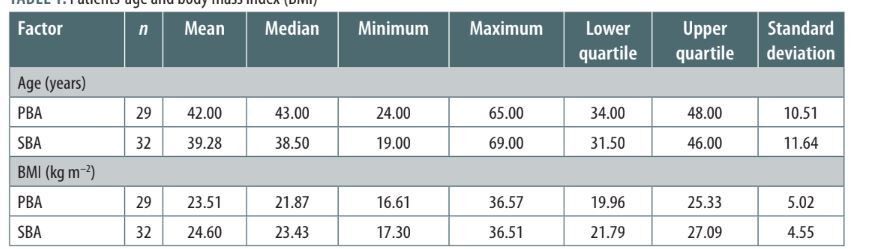
Mostly middle-aged patients with a normal mean body mass index (BMI) were tested. Details are presented in Table 1.
TABLE 1
Patients’ age and body mass index (BMI)
As the distribution in the groups was close to normal, the t-test was applied. Levene’s test showed that the condition of homogeneity of variances was also met (F = 0.088, P = 0.77 and F = 0.11, P = 0.75, respectively). The groups did not differ significantly in the patients’ average age and BMI (t = 0.95, P = 0.344 and t = –0.88, P = 0.380, respectively).
Education
Most of the patients had completed higher education (see Table 2).
TABLE 2
Patients’ education
| Group | Higher education | Secondary education | Primary education | Total |
|---|---|---|---|---|
| PBA | 18 | 8 | 3 | 29 |
| SBA | 23 | 9 | 0 | 32 |
| Total | 41 | 17 | 3 | 61 |
There was also no relationship between the level of education of the patients and their assignment to the investigated groups (G = 4.68, p = 0.096).
Episodes of bradycardia or hypotension
Episodes of bradycardia (< 60/min) or hypotension (mean arterial pressure [MAP] < 65) lasting 10 minutes during anesthesia were taken into account. Bradycardia was treated with single doses of 0.5 mg i.v. atropine (Atropinum Sulfuricum WZF, Poland). Hypotension was treated with single doses of 5 mg i.v ephedrine (Epfedrinum hydrochloricum WZF, Poland). Bradycardia occurred in 4 patients under PBA, and 7 patients under SBA (18% in the whole group). Only 4 patients had an episode of 10-minute hypotension in the SBA (6.56% in the whole group). The comparison of both schemes of anesthesia did not reveal significant differences in those factors (χ2 test, P > 0.05).
MoCA results
Descriptive statistics: in both types of anesthesia, the patients achieved high mean scores in the MoCA (see Table 3 for details).
TABLE 3
Perioperative MoCA results
Comparative statistics of the MoCA scores within and between the groups: changes in the MoCA within the PBA and SBA groups – in both groups a significant increase in the MoCA scores was noted (PBA: Z = 3.086, P = 0.002; SBA: Z = 2.800, P = 0.005).
The changes in the MoCA scores were compared between the PBA and SBA groups. The difference in the MoCA scores between time points 1 and 2 was determined for this purpose. The results of the Mann-Whitney test did not allow rejection of the hypo thesis of the equality of the MoCA changes in the PBA and SBA groups (Z = 0.63, P = 0.53).
Descriptive statistics for the neuroinjury markers NFL, UCH-L1, GFAP, and tau for both types of anesthesia are shown in Table 4.
TABLE 4
Perioperative levels of neuroinjury markers
Comparative statistics of neuromarker levels within and between groups: the results of the Shapiro-Wilk test for the difference in the GFAP, NFL, tau, and UCH-L1 values showed that their distribution was significantly different from normal (P < 0.001 in all cases). Therefore, the non-parametric Mann-Whitney test was applied to compare the investigated groups.
In the PBA group there were significant changes between the first and second measurement in the NFL (Z = 4.703, P < 0.001) and UCH-L1 (Z = 4.487, P < 0.001).
In the SBA group there were significant changes between the first and second measurement in the GFAP (Z = 2.730, P = 0.006), NFL (Z = 4.581, P < 0.001), and UCH-L1 (Z = 4.656, P < 0.001).
The test revealed significant differences in the distribution of GFAP changes between the study groups (Z = –2.579; P = 0.0099). No significant differences were found in the other markers’ changes between the groups (P > 0.05).
Correlation with neuroinjury markers
There were no significant relationships between changes in the MoCA test and changes in the markers in the study groups (P > 0.05).
There was no significant correlation between the difference in the MoCA test results between dates 1 and 2, patients’ age, and anesthesia groups (P > 0.05).
Age as a moderator of changes in the GFAP, NFL, tau, and UCH-L1 levels. No significant correlations were found between changes in the marker concentrations and the patients’ age in individual groups (P > 0.05).
DISCUSSION
The problem of cognitive alterations in the early postoperative period is still an important issue in the scientific discourse. Our research was conducted on a group of mostly well-educated middle-aged women, whose cognitive status and possible early alterations in selected neuromarkers were tested after exposure to two schemes of anesthesia. We observed a substantial postoperative increase in results of the cognitive test despite a detectable increase of the tested neuroinjury markers. Most researchers have conducted extensive tests on groups of elderly patients and focused on late sequelae evaluated months after the anesthesia and surgery [19]. Currently, a more common scheme of the surgical approach involves one-day hospitalization, and carrying out the postoperative follow-up observation becomes more challenging, sometimes even impossible, although we admit that additional postoperative assessment would bring deeper insights in the topic. Our group was relatively small, but demographically homogeneous, thus minimizing the potential influence of sex-related differences during cognitive testing.
The depth of anesthesia was strictly guided by the BIS of 40–50 in both groups of patients. Shu et al. [20] conducted a study on middle-aged gynecological patients and found that combined intravenous-inhalational anesthesia with propofol and sevoflurane (although they used the less sensitive MMSE for cognitive screening and the Trail Making Test assessing the working memory) within this BIS range resulted in a milder influence of anesthetics on the postoperative cognitive function of young and middle-aged laparoscopic patients [20].
Both schemes of anesthesia were characterized by comparable hemodynamic stability. There was no difference in prolonged bradycardia or hypotension between the groups. Hypotension may be one of the important factors contributing to cognitive disturbances in elderly patients in an early postoperative period. Wu et al. [21] analyzed a group of men (72) and women (40). The women’s mean age was 65.03 years, which was much higher than in our study, affecting the results. This difference in age may have caused postoperative neurocognitive disturbance. Apart from that, the occurrence of cognitive alterations was analyzed on the 7th day after the operation, not one day after the procedure, as in our study.
The MoCA is considered to be a relatively sensitive and effective tool for cognitive screening. It is more valuable than the popular MMSE for both regional and general anesthesia, including when applied 24 h after the surgery [22]. It is also a valuable tool for detecting mild cognitive impairment, including in the general Polish population [3]. The comparison of the MoCA in the pre- and postoperative periods revealed a significant increase in test results regardless the type of anesthesia. Our results were consistent with the results reported by Žura et al. [23], who tested the postoperative cognitive dysfunction (POCD) in patients after either laparoscopic or classical prostatectomy preoperatively and 48 h later. Although male patients were tested, they also achieved higher MoCA scores postoperatively regardless of the surgical technique used. The researchers attributed this effect to anxiety. On the other hand, in the study by Li et al. [24], on the first day after the surgery the rate of POCD (defined as a decrease in the MoCA by 1 SD) ranged from 8.6% to 19.9% depending on the rate of propofol infusion. On the one hand, similarly to our protocol, they also used the MoCA in the direct perioperative period in the laparoscopic surgery. Nevertheless, their groups of patients were much older (the mean age was 63–75 years) and included patients with a history of cerebral vascular incidents and with cardiac insufficiency (our study excluded such patients). No information on depressive syndromes was provided. In our study, a significant improvement in the MoCA results was observed not only in the PBA group but also in the SBA group directly after the surgery. When discussing the problem of cognitive testing, we should take into consideration the problem of immediate retesting. Multiple applications of the MoCA produce a very weak retest effect if alternative versions are used [25]. The multi-faceted nature of the test makes it difficult to achieve a significant learning effect in a short period of time [26]. Unfortunately, at the time of conducting the study, there were limitations regarding the number of validated parallel MoCA versions available in Polish for three measurements. Costa et al. [25] discussed the issue of parallel forms of MoCA and suggested that while they may reduce the learning effect, with short intervals between tests and when assessing clinical changes, the practice effect is usually small. Using a single, well-validated version was the pathway to achieve methodological consistency and data comparability, especially given the short intervals between measurements. There are also situations where alternative versions cannot be used (e.g. language versions without verified alternative forms) or where the test-retest MoCA can be run 4 or more times. In the meta-analysis by Scharfe, the retest effect in various cognitive tests with regard to the possible duration of the test-retest intervals was analyzed. The authors concluded that shorter intervals lead to a smaller total learning effect [27]. In summary, anesthesia and surgery – which could potentially abolish or reduce the test learning ability – did not cause this phenomenon, which reflects positively on the patients’ postoperative cognition.
In both groups there was a significant increase in the NFL and UCH-L1 levels soon after the anesthesia, and these values were comparable among the patients. Both neuromarkers are associated with axonal integrity and function.
NFL has already been assessed in terms of the correlation between the serum and cerebrospinal fluid concentrations and predicted an unfavorable neurological course of aneurysmal subarachnoid hemorrhage [28]. In another study, the plasma levels of phosphorylated tau and NFL enabled differentiation of AD patients from healthy control subjects [29]. Some of the studies on PND suggested a common pathophysiological pathway of AD and PND (e.g. significantly elevated Aβ deposition in the hippocampal CA3 region of ApoE4-KI mice on postoperative days 4 and 7 vs. control mice after exposure to propofol and surgery, significantly higher levels of Aβ42 and NFL in the cerebrospinal fluid in elderly patients with PND) [30, 31].
The increase in the UCH-L1 level was also associated with the occurrence of AD [11]. To the best of our knowledge, no prior studies have investigated the perioperative changes in the UCH-L1 level. Our study seems to be the first one providing such data. The statistical correlations observed in our study suggest the need for further research in this field.
Additionally, the GFAP level was also altered in the SBA group. However, the analysis of the means and medians of GFAP concentrations in the preoperative measurements showed that these results may have been accidental. Guo et al. [32] observed an altered GFAP value in the nucleus accumbens of rats exposed to open laparotomy, but only in the late period: 15 and 30 days after the operation. In patients after CABG off-pump cardiac surgery, the plasma circulating miRNA for GFAP was a predictor of postoperative delirium [33]. In another study on cardiac surgery patients, on the discharge of PND patients the GFAP and tau levels were significantly elevated, although further statistical analysis revealed only modest predictive abilities for PND at discharge [34]. It is important to remember that there are substantial differences in the nature and intensity of pathologies developing during cardiac surgery in patients under extracorporeal circulation, which make comparisons difficult to interpret. An interesting question arises regarding the possible molecular explanation of the sevoflurane activity on GFAP release, which was not statistically significant after exposure to PBA.
The lack of a significant postoperative increase in tau after the procedure was rather unexpected. If axonal injury is taken into account as a possible pathology occurring after anesthesia, the tau level should consequently increase postoperatively, as an abundantly expressed protein in axons. It may result from the inadequate timing of blood sampling. We sampled blood only 24 hours after the operation. Results obtained from later sampling could strengthen the analysis. However, patients had been released from the hospital after 24 hours, and we were not able to collect additional samples. The lack of its significant increase seems to be a positive outcome for the patients, especially due to the fact that in animal studies, propofol increased the hyperphosphorylation of the hippocampus neurons and led to cell injury [35]. In studies conducted on humans, the preoperative increase in the plasma tau level was a predictor of postoperative delirium after knee and hip replacement or laminectomy [36], whereas the postoperative increase was a predictor of delirium in patients after major cardiac operations [37]. Still, delirium is an extremely pronounced pathology. Our study focused on the subtle changes in less invasive procedures, which may be the reason for the low plasma tau levels observed in our patients.
The changes in neuromarkers did not translate to the clinical outcome in MoCA results. None of the selected neuromarkers correlated with the MoCA results. We may consider that the subtle neuroinjury detected in selected neuromarkers was not able to trigger the clinical deterioration. The utility of applying neuromarkers into diagnostics of patients with high sensitivity (100%) and low specificity (38.5%) was established for GFAP, heart fatty-acid binding protein (H-FABP), and interleukin 10 for acute trauma brain injury (TBI) when these neuromarkers were compared with computed tomography results [38]. Koivikko et al. [39] measured S100B, H-FABP, NFL and IL-10 levels in patients with TBI to evaluate their diagnostic usefulness in acute moderate brain trauma. The results for the neuromarkers were significantly lower than in patients with moderate and severe TBI, but alone or in combination were unable to distinguish patients with TBI from orthopedic controls. Only high postoperative levels of S100β, neuron-specific enolase, and Aβ may predict PND in patients after CABG according to Wang et al. [40]. The authors concluded in the end that the relationship between these biomarkers and PND may be affected by sampling time. Unfortunately, the available data on the possible correlations of neuromarkers and the results of the MoCA are very scarce in the literature. Nurcahyo et al. [41] analyzed the correlation between MoCA INO results (Indonesian version of MoCA) and GFAP in 28 PND patients after CABG operations and found higher GFAP levels in this group 73 hours after the operation. Unfortunately, the authors did not provide the units in which the GFAP was described (neither in the text nor in the tables), which makes it difficult to make comparisons. To our knowledge, our study seems to be one of very few analyses of the mutual relationships between the selected neuromarkers and MoCA results. Further research in this field is necessary. Future research could place special emphasis on the set of neuromarkers, sampling time, and predictive cut-off values.
The age of the patients in our group predicted neither the MoCA nor the neuromarker results. The physiological ageing process triggers important changes in the brain morphology (e.g. cerebral atrophy with decreased complexity of dendritic arborization, reduced synaptic density, loss of myelin, axons, cells, astrocytic gliosis, arterial inflammation and stiffening), neuronal and glial biochemistry (dysfunction of the cholinergic, dopaminergic, serotoninergic systems, disturbed blood-brain barrier), and the molecular structure (e.g. alterations in gene expression, stress response, telomere shortening, mitochondrial dysfunction, accumulation of molecules damaged by oxidative stress, electrophysiological changes, dys-regulation in neuronal calcium homeostasis), but they are commonly considered to be mild [42, 43]. Age is a well-known risk factor of cognitive alterations [13, 44, 45]. Our patients were mostly middle-aged and well-educated, and these factors may have contributed to the cognitive sparing effect.
LIMITATIONS OF THE STUDY
Limited number of study participants, lack of long-term follow-up, reliance on a single version of the MoCA and its test-retest effect.
CONCLUSIONS
In the context of earlier studies, which proved the efficacy of neuroinjury prediction, it can be tentatively concluded that both types of anesthesia used in our protocols resulted in a favorable postoperative cognitive status regardless of the significant changes in the plasma levels of GFAP, NFL, and UCH-L1. Our study showed that stable anesthesia for laparoscopic gynecological operations resulted in a safe cognitive outcome for the patients in the most vulnerable period of hospitalization, regardless of the type of anesthetic used. Further research could focus on the possible causes of the postoperative MoCA increase in the context of preoperative distress, which still seems to be a greatly underestimated issue.