
Peripheral venous catheter (PVC) insertion is one of the most common interventions in medicine. It is also an essential part of the patient’s prepara- tion for elective surgery unless the insertion of a central venous catheter is required. Conventio- nally, the visualization and palpation technique of insertion is used. However, it has been reported that the success rate of the first puncture using this method can be as low as 51% in various settings and that 3 or more punctures may be required in up to 7% of patients [1]. Unsuccessful attempts to insert a PVC in patients undergoing surgery pro- long patient preparation and increase patient stress and discomfort before surgery. A way to increase the success rate of the first cannulation attempt is ultrasound (US) guidance or assistance in patients with or without predicted difficult PVC insertion [2]. A recent significant improvement in ultrasound technology made it possible to use this method nearly everywhere. It has been shown that, in the setting of the emergency department, the ward, and pre-hospital emergency medicine, ultrasound guidance or assistance improves the overall success rate and success rate of the first attempt, and may reduce the total number of necessary attempts in different patient populations [1–5].
However, the method of ultrasound-assisted PVC insertion has not been evaluated in the environment of an operating theatre yet in a non-selected pa- tient population. Therefore, we decided to perform a prospective randomized clinical trial to compare the conventional method and ultrasound-assisted method for peripheral venous cannulation in pa- tients undergoing surgery in general anaesthesia. The aim of the trial was to assess the superiority of US assisted PVC insertion over conventional tech- nique. We hypothesized that there is a statistically significantly higher success rate on the first attempt when the ultrasound assistance method is used in comparison with the conventional method.
METHODS
We conducted a prospective randomized con- trolled unblinded clinical trial on adult patients scheduled for elective surgery in general anaes- thesia indicated for PVC placement in the opera- tional theatre. The trial was approved by the local ethical committee (Ethics Committee, Masaryk Hospital Usti and Labem, Czech Republic, reference code 290/13). The study was conducted following the Declaration of Helsinki and good clinical prac- tice. All patients or their legal surrogates agreed to be included in the clinical trial and signed a written informed consent form. The trial has been registered with the number NCT05119985 at https://clinical-trials.gov/study/NCT05119985.
Trial design
After obtaining informed consent, patients were randomized to one of the two predefined groups in a 1 : 1 ratio. The randomization was done as part of the pre-anaesthetic examination. This examina- tion was minimally three weeks before the surgery. In Group A, the further intervention was the inser- tion of a PVC using ultrasonographic assistance, whereas, in Group B, cannulation was performed using the conventional visualization and palpation technique. The procedure of cannulation was car- ried out in the operating theatre, immediately before the surgery. The indication, the procedure of cannu- lation and the maintenance of PVC were conducted according to the international ERPIUP consensus [6].
Standard PVCs, with a gauge size from 16 G up to 22 G and a length of 32 mm, were used in both groups. The Sonosite SII-VA (Bothell, Washington, USA) probe was used with a Fujifilm Sonosite PX ultrasound machine (Bothell, Washington, USA) for ultrasound-assisted cannulation in Group A.
The target vein was selected according to the protocol: the upper arm basilic vein, upper arm cephalic vein, or median cubital vein as the first choice; the lower arm basilic vein or the lower arm cephalic vein as the second choice; the rete veno- sum dorsale manus was selected as the third choice.
However, the final decision was made by the inves- tigator based on individual assessment of the pos- sibility of cannulation in a given cannulation site, in- cluding the selection of the right or left upper limb. After selecting the target vein, the cannulation was performed as described below. If the first cannula- tion attempt was unsuccessful, at least two more attempts were performed in both groups. If even those were unsuccessful, further attempts were allowed according to the investigator’s decision, or an alternative procedure (including ultrasound guidance in Group B) could be used. If all cannula- tion attempts failed, alternative approaches were used for securing vascular access.
The duration of the trial intervention was mea- sured using a Decathlon Kalenji ONstart 110 stop- watch (Villeneuve d’Ascq, France). The measurement began with the start of the cannulation attempt and stopped when the sterile covering of the inserted cannula was finished, or when cannulation attempts were terminated due to failure. In all enrolled pa- tients, the modified A-DIVA score was used for eval- uating the difficulty of peripheral venous access [7].
Patients’ enrolment
All patients included in the trial were admitted to the Masaryk Hospital in Usti nad Labem, Czech Republic for elective surgery. This is a tertiary hos- pital in the North Bohemian region. Eligible partici- pants were enrolled from the 1st of December 2021 to the 15th of December 2022. The inclusion criteria were an adult patient scheduled for elective sur- gery under general anaesthesia, an indication for PVC insertion, and a signed informed consent form. The exclusion criteria were as follows: unconscious- ness, age < 18 years, primary indication for central venous catheter placement, contraindication of an ultrasound examination, contraindication of peri- pheral venous cannulation on both upper arms (acute skin lesion, phlebitis, phlegmon, burns, frost- bite, eczema, trauma, arteriovenous malformations, arteriovenous fistulas) and the patient’s refusal.
Study interventions
In Group B, conventional PVC insertion was performed in accordance with the recent common practice without ultrasound or other guidance or assistance guidance except for visual and tactile identification of the target vein after proximal limb compression [8].
In Group A, the basic technique was the same as in Group B with added ultrasound assistance. After tourniquet placement in the middle of the upper arm, a display depth of 3.0 cm was set on an ultrasound device. Ultrasound scanning with the linear probe in the transverse orientation was used for target vein identification. To differentiate the target vein from an artery, a compression test was used for each patient and assessed the pulsatility of an artery. The target vein was chosen taking into account the diameter and depth of the vein. Preference was given to the vein with the largest diameter of all those found and located preferably no deeper than 1 cm below the skin surface [9]. The optimal puncture site was chosen. Then, the cannulation was performed con- ventionally, without further help of ultrasound.
Competence of investigators
Twenty anaesthetist nurses participated in the trial as investigators and measured the data. All investigators met the local competence for ob- taining peripheral venous access with or without ultrasound guidance.
Anaesthetist nurses were naive to ultrasound guidance methods prior to the trial but were highly experienced in the conventional method. Each had performed more than 2000 peripheral venous can- nulations in the setting of an operating theatre – an assumption based on the years of experience. One month before patient recruitment started, all inves- tigators took part in a course that aimed to provide the necessary theoretical and practical background for ultrasound-assisted peripheral venous cannu- lation. All investigators attended 2 hours of theo- retical and 2 hours of practical hands-on courses, 2 hours of a course about anatomical areas on upper limb, a 4-hour long theoretical session with a discussion regarding the use of ultrasound for venous identification (Doppler imaging, pulsatility, compression test, most common mistakes in vein identification), and a 4-hour long practical course on ultrasound guidance for peripheral venous can- nulation. The hands-on course focused on ultra- sound-assisted peripheral venous access cannula- tion using the CAE Blue Phantom Branched 4 Vessel Ultrasound Training Block Model (CAE, Sarasota, Florida, USA). The four-hour practical session pro- vided participants with the opportunity to perform ultrasound-assisted peripheral venous cannulation on patients undergoing general anaesthesia, all under the direct supervision of a course instructor. The course had an instructor–attendant ratio of 1 : 5.
The primary objective of the trial was to com- pare the success rate of the first attempt of PVC in- sertion into the superficial venous system of the up- per extremities in an operating theatre in patients undergoing surgery in general anaesthesia between the groups.
The secondary objective was to compare the overall peripheral venous cannulation success rate, the number of attempts required for securing peri- pheral vein access, the time needed for PVC place- ment, and the functionality of the catheter the day after insertion.
Statistical analysis
A sample size of 498 subjects was calculated to identify a 20% difference in the primary out- come between the two groups with 90% power with a cut-off for statistical significance of P = 0.05. The mean values ± standard deviation (SD) or per- centages were calculated as necessary. Patients were randomized by Study Randomizer Software Application 2017, Available at: https://www.study-randomizer.com. Differences between groups were compared using the c2 test, and statistical significance was calculated by the Fisher exact test for alternative variables. For ordinary variables, the Mann-Whitney U test was used to calculate statistical significance. Statistical significance for continuous variables was determined by the paired Student t-test. The data were analysed using Micro- soft Excel 2010 (Microsoft, Redmond, WA, USA) and JMP 3.2 statistical software (SAS Institute, Cary, NC, USA). A P-value less than 0.05 was considered sta- tistically significant. Subgroups, predicted difficult PVC insertion, non-predicted difficult PVC insertion, one attempt for successful PVC insertion and mul- tiple attempts for successful PVC insertion, were identified and statistically compared during post hoc analysis.
RESULTS
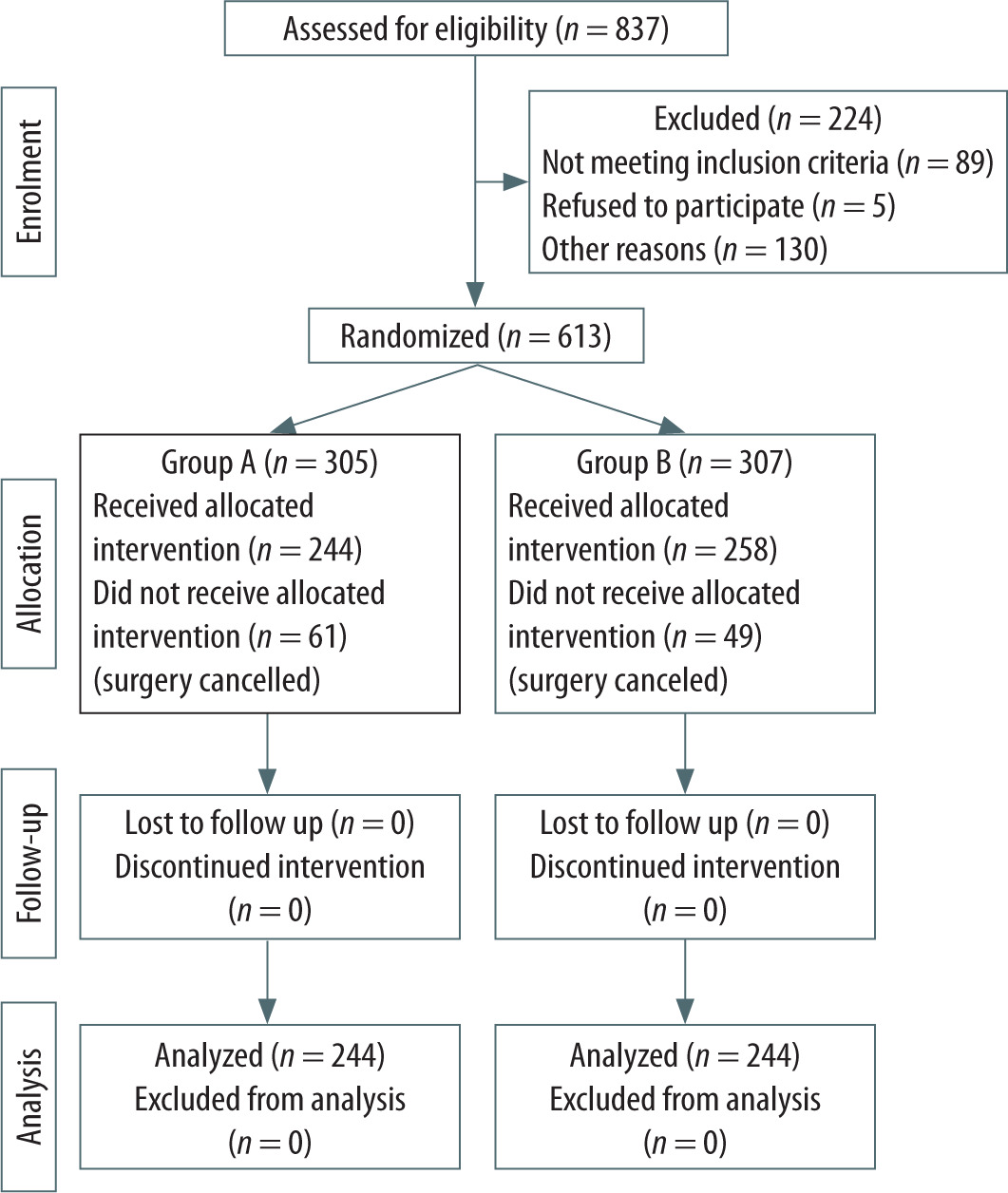
A total of 837 patients were assessed for eligibil- ity. A total of 613 subjects were randomized to two groups equally. There were 61 patients in Group A and 49 patients in Group B who did not receive the allocated intervention because of surgery cance- lation due to the COVID-19 pandemic outbreak. See Figure 1 for a diagram of the enrolment process.
The baseline demographic data and clinical characteristics of the patients in the groups are pre- sented in detail in Table 1. There were no statistically significant differences in demographic and clinical characteristics between the patients in the groups and patients excluded due to the COVID-19 pan- demic outbreak.
TABLE 1
Demographic data and clinical characteristics of patients in the groups
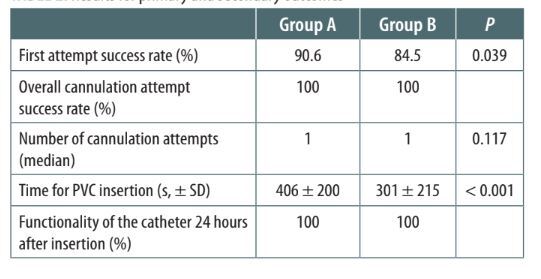
The success rate of the first cannulation attempt was significantly higher in Group A compared to Group B (Group A: 90.6%, Group B: 84.5%, P = 0.039). Both groups achieved a 100% overall success rate, with no cases requiring a change of the cannulation method beyond the randomized intervention. We did not observe a statistically significant difference in the total number of cannulation attempts per- formed per patient in Group A compared to Group B (Group A: median 1, Q1 = 1, Q3 = 1, Group B: median 1, Q1 = 1, Q3 = 1, interquartile range in both groups 0, P = 0.117). The time required for the procedure re- gardless of the number of attempts was significantly longer in Group A than in Group B (Group A: 406 ± 200 s, Group B: 301 ± 215 s, P < 0.001). We did not observe a statistically significant difference in func- tionality of the catheter on the day after insertion, as the functionality was in both groups 100% at that time. For details see Table 2.
TABLE 2
Results for primary and secondary outcomes
The mean score of predicted cannulation diffi- culty was comparable in both groups (Group A: 0.6, Group B: 0.7, P = 0.267).
There were no statistically significant differences between the groups in the selection of the cubital and distal part of the forearm as the target cannula- tion site. In Group A, the median cubital vein was cannulated in 32.8% of cases, compared to 31.4% in Group B (P = 0.737). The basilic vein was cannulated in 52.5% of cases in Group A and 46.1% in Group B (P = 0.152). The cephalic vein was cannulated in 14.7% of cases in Group A and 22.5% in Group B, with a statistically significant difference (P = 0.025).
There were no cannulation attempts on the rete venosum dorsale manus in either group.
In post hoc analysis of the subgroup of patients in whom only one attempt was sufficient for PVC insertion, we found that the time required for the procedure was longer in Group A (n = 221) than in Group B (n = 217) (Group A: 377 ± 152 s, Group B: 246 ± 138 s, P <0.001).
In the post hoc analysis of the subgroup of pa- tients who required more than one attempt to suc- cessfully insert the PVC, we identified a comparable number of attempts in both groups (Group A: me- dian 2, Group B: median 2, interquartile range 0, P = 0.409), as well as the time required to success- fully insert the PVC (Group A: 691 ± 342 s, Group B: 601 ± 301 s, P = 0.283). We found no significant dif- ference in the proportion of different cannula sizes used between the groups.
Upon analysing the subgroup of patients pre- dicted to have difficult cannulation and those pre- dicted to have non-difficult cannulation, we found that the difference in the success rate of the first cannulation attempt was in favour of Group A in both subgroups, but it did not reach statistical sig- nificance. The findings are presented in detail in Table 3.
TABLE 3
Comparison of outcomes between groups in patients with predicted difficult cannulation and non-difficult cannulation
The estimated effect sizes for the trial outcomes were small, as indicated by Cohen’s d values below 0.2.
DISCUSSION
Peripheral vein cannulation is an intervention that is performed in the case of nearly every patient undergoing any type of anaesthesia. The reported first-attempt success rate in different in-hospital clinical settings may be as low as 51%, and in up to 7% of cases, three or more attempts are needed to successfully perform peripheral vein cannulation [1, 4, 5]. Paradoxically, to our best knowledge, there are insufficient data for cannulation in the operating theatre setting.
However, great emphasis should be placed on the success of first-attempt cannulation in this set- ting to optimize workflow, reduce patient discom- fort, and limit the number of punctures as potential sources of bleeding. There are several methods to increase the first attempt success rate of the proce- dure [10, 11]. The generally accepted one is ultra- sound navigation [12]. Published clinical trials in an adult and paediatric population are characte- rized by a similar design and definition of the spe- cific clinical setting in which the studies were conducted (emergency department, pre-hospital setting, in-hospital ward) [2, 4, 5, 8, 13, 14].
Most of the trials were conducted on patient populations with anticipated difficult or moder- ate peripheral venous access. Van Loon et al. [3] published a meta-analysis of eight clinical rando- mized trials, with a total of 1660 patients, showing the overall success rate in the ultrasound group to be 81% and 70% in the control group, with an odds ratio for success associated with ultrasound guidance of 2.49 (95% confidence interval [CI]: 1.37–4.52, P = 0.003). Moreover, reduction of the number of puncture attempts and the time needed to achieve overall success and a trend of increas- ing success rates with the first puncture attempt were documented [2, 3]. The largest randomized clinical trial was completed by McCarthy et al. [11] on 1189 emergency department patients. In the pa- tients with anticipated difficult or moderately dif- ficult access, ultrasound guidance was associated with an increased success rate, while in the easy access group, it was not. In a recent randomized clinical trial completed by Skulec et al. [2] in 2020, ultrasound guidance in the non-selected patient population was associated with an increased suc- cess rate. This clinical trial is the only one previously conducted on a non-selected patient population, like ours. In our study, we used the A-DIVA score to predict difficult peripheral vein cannulation; however, patients were not selected based on this evaluation [7]. Other studies provide only limited information, indivi dually, for small numbers of par- ticipants.
In the clinical setting of the operating theatre, as in our trial, two studies have been published: one by Aponte [15] and the second by Pappas [16], both on a patient population with predicted different PVC insertion, which is a different population compared to that in our trial. An important aspect of our trial is that participants were not classified according to the anticipated difficulty of cannulation, and there- fore data could be extrapolated to the general pa- tient population. Both studies mentioned differ in the number of participants compared to our trial; thus, although their findings align with ours, they cannot be generalized.
Moreover, in the clinical trials conducted on pa- tients with anticipated difficult or moderate venous access, different methods of anticipation were used.
In conclusion, published data have shown that ultrasound guidance or assistance may increase the success rate of PVC placement in the hospital ward, emergency department and operating theatres.
These findings are in concordance with our find- ings. The main finding of our trial was that the ultra- sound-assisted insertion of a PVC in the general patient population scheduled for elective surgery in general anaesthesia was associated with a higher first-attempt success rate than the conventional method. This may be attributed to the enhanced visualization of vessel position and trajectory pro- vided by ultrasound assistance. Moreover, with this information, the operator can select a more suitable vessel for cannulation. Benkhadra et al. [17] also re- ported a higher success rate at first puncture attempt (85% vs. 35%, P = 0.001) and a shorter procedure time (63.5 vs. 420.5 s, P < 0.001) when using ultrasound guidance in a general paediatric population.
The most common method of ultrasound guid- ance is based on vein visualization on its short axis and needle tip control until it reaches the centre of the vein [18]. Skulec et al.[2] compared two dif- ferent ultrasound guidance methods – full ultra- sound guidance and ultrasound alone – for find- ing the target vein with subsequent conventional PVC placement, and they found that the latter was non-inferior to the former. Based on this finding, we chose visualization of the vein on its short axis.
In the control group, the overall success rate did not differ from the interventional group and was consistent with predictions based on several clinical studies [1, 3–5]. The overall success rate was 100%. We attribute this high rate to two factors. First, all the patients enrolled in this clinical trial were elec- tive patients, and second, all the operators partici- pating in this clinical trial were skilful and routinely performed PVC insertions on a daily basis. Therefore, we cannot extrapolate our findings to professionals who are not trained in PVC insertion.
We found that the time needed to insert the PVC was statistically significantly longer when ultra- sound assistance was used in the cohort in which only one attempt was needed. In the cohort where more than one attempt was needed to successfully insert the PVC, the time did not differ. We attribute this prolongation to the extra time needed to turn on the ultrasound machine. However, the prolonga- tion seems not to be clinically important.
All procedures in our trial were performed in a single-operator manner. Therefore, the results support the option to delegate ultrasound-guided cannulation of a peripheral vein to nurses. This is particularly relevant to the European medical set- ting, in which ultrasound usage falls mainly within the physician’s scope of practice. However, a suf- ficient level of training must be provided before the widespread implementation of this technique among nurses, who are typically inexperienced in ultrasound application.
We recognize several limitations of the trial. First, it is a single-centre trial, and therefore its generaliz- ability is limited. Another limitation is the number of ultrasound machines available. During the trial there were seven ultrasound machines in the com- plex of nine operating theatres. Therefore, there was no issue in accessing the ultrasound equipment when needed. The results for centres with limited access to ultrasound may differ regarding the time needed for cannulation. Also, the trial did not in- clude acute surgical patients. We did not include this group of patients for safety reasons to avoid any potential delay due to trial intervention. The trial did not include the paediatric patient population. The findings of our trial could therefore be extrap- olated only to the adult population. We observed a significantly higher first attempt success rate than was anticipated. The higher first pass success rate in our trial compared to other trials was likely due to different settings. To our best knowledge, there have been no reported data of first pass attempt success rates in operating theatres in the general patient population. The final limitation we should note is the number of patients who were lost after randomization that was done three weeks prior to surgery. These patients were lost due to cancelation of their surgery because of the COVID-19 pandemic outbreak. During this outbreak, according to Czech law, all scheduled elective surgical procedures had to be cancelled to preserve the hospital capacity for emergency cases and to enhance the hospital’s abil- ity to care for patients with respiratory failure.
CONCLUSIONS
The results of our trial show that ultrasound guidance of peripheral vein cannulation in elective surgical patients in general anaesthesia increases the first attempt success rate in comparison with the conventional landmark method. Moreover, our trial shows that ultrasound guidance and select- ing the left upper limb for peripheral cannulation improve the chance of successful peripheral vein cannulation on the first attempt. We consider the ul- trasound guidance method for introducing PVC to be an effective and clinically relevant method for implementation in an operating theatre setting. We recommend structured training on this method be- fore implementation in daily practice.