
Neuropathic pain (NP) is pain arising as a direct consequence of a lesion or disease affecting the somatosensory nervous system [1, 2].
It impairs the patient’s quality of life in social, economic, and psychological aspects [3].
The diagnosis of NP relates to a detailed neurological examination. It is recommended for every day use by clinicians, as well as for research purposes [2–4].
Detailed neurological examination and the diagnosis of NP can be established by means of the DN4 questionnaire (Douleur Neuropathique en 4 questions) [5]. It consists of seven items concerning the presence of pain symptoms (burning, painful cold, electric shocks, tingling, pins and needles, numbness, itching) and three related to physical examination (hypoesthesia to touch, hypoesthesia to pinprick, pain caused or increasing by brushing) [6]. The presence of four or more of the above symptoms qualifies the pain as neuropathic.
The basic tool for assessing any pain intensity is the Numerical Rating Scale (NRS) [7]. This is a unidimensional measurement of pain intensity in which a respondent selects a whole number (0 to 10 integers) that best reflects the intensity of his or her pain. While zero means no pain, 10 corresponds to the worst pain intensity imaginable. Higher scores on the NRS mean greater pain intensity. The NRS is characterized by good reproducibility and suitability for scientific applications [7, 8]. Neuropathic pain therapy should be multidisciplinary. The first and second choice in pharmacotherapy of NP are gabapentinoids and antidepressants (ADs): tricyclic ADs (TCAs), serotonin-norepinephrine reuptake inhibitors (SNRIs), as well as lidocaine and capsaicin, used topically for localized or peripheral neuropathic pain [9]. The third line of pharmacotherapy includes selective serotonin reuptake inhibitors (SSRIs) or certain other anticonvulsants (lamotrigine, carbamazepine, topiramate, and sodium valproate), as well as N-methyl-D-aspartate receptor (NMDA) antagonists. Opioids are proposed for use in severe pain (especially in the case of NP accompanying cancer) or in cases of temporary exacerbation [9]. The strategy of the first and second line of systemic pharmacotherapy in NP according to the latest guidelines and recommendations is shown in Table 1.
TABLE 1
The strategy of neuropathic pain pharmacotherapy according to selected guidelines and recommendations
| Guidelines/Recommendations (year) | First-line pharmacotherapy | Second-line pharmacotherapy |
|---|---|---|
| 2010 [10] | TCAs, SNRIs, gabapentin, pregabalin | Tramadol, other opioid analgesics |
| 2014 [11] | Monotherapy: TCAs, SNRIs, gabapentin, pregabalin. Tramadol, other opioid analgesics | Combination therapy: (TCAs or SNRIs) and (gabapentin or pregabalin) and tramadol, other opioid analgesics |
| 2015 [4] | Monotherapy: SNRIs, TCAs, pregabalin, gabapentin (combination therapy may be considered as an alternative to increasing dosages in monotherapy). | Tramadol |
| 2019 [9] | Monotherapy: TCAs, SNRIs, gabapentin, pregabalin | Combination of first-line therapies Tramadol |
| 2022 [12] | Monotherapy: SNRIs, gabapentin, TCAs. | Pregabalin Combination of ADs and gabapentin/pregabalin Tramadol |
It is hypothesized that ADs increase both the recruitment of noradrenergic descending pathways and peripheral release of noradrenaline from sympathetic fibers into dorsal root ganglia. Additionally, their effect might be mediated by their anti-proinflammatory cytokine effects and their influence on the opioid system [13].
ADs are recommended to be used as the first, second, or third choice in the treatment of NP, and their effectiveness is indisputable at the current level of knowledge.
Amitriptyline has a number needed to treat (NNT) of 2 (95% CI: 1.7–2.5), and a relative risk (RR) of 4.1 (95% CI: 2.9–5.9), for the achievement of at least moderate pain relief. Venlafaxine (three studies) has an NNT of 3.1 (95% CI: 2.2–5.1) RR 2.2 (95% CI: 1.5–3.1) [14]. Duloxetine (standard dose of 60 mg) showed a small to moderate effect for substantial pain relief (OR = 1.91, 95% CI: 1.69–2.17) in a meta-analysis [15]. It is also effective in painful diabetic neuropathy, with an NNT of 5.8 (95% CI: 4.5–8.4) [16]. This is reflected in the inclusion of ADs in the treatment of NPs in many guidelines and recommendations [4, 9, 11, 12, 17]. The effectiveness of such a therapy can be assessed only after a trial period of treatment with doses previously titrated to the therapeutic range [9, 10].
However, guidelines do not suggest how long should ADs be used in NP treatment if the patient is benefiting from the therapy. In depression treatment WHO strongly recommends the length of AD usage as not shorter than 9–12 months after recovery from a depressive episode or disorder in adults who have benefited from AD therapy [18]. A more recent study recommends maintaining AD therapy for at least 6 months after remission of acute major depressive disorder [19].
In the clinical reality, AD prescriptions in psychiatric settings differed from the clinical guidelines and evidence-based recommendation [20].
In the Australian population, the average duration of therapy in depression is now approximately four years, and half of users are long-term users [21, 22].
Studies assessing the effectiveness of AD treatment for neuropathic pain analyze, on average, periods no longer than 10–13 weeks [15].
There is currently no reliable evidence for the longterm efficacy of any ADs. There in also no evidence for the safety of ADs for chronic pain treatment [15]. Simultaneously, despite a 66% increase in published trials, only a limited improvement of NP treatment has been obtained, and a large proportion of neuropathic pain patients are left with insufficient pain relief [23].
The current study was designed as a retrospective cross-sectional study to analyze the real effectiveness of ADs in the treatment of NP in pain clinics in Warsaw. We focused on the relation between AD intake and the intensity of NP and on their impact on the intensity of pain in long-term use.
We aimed to: 1) assess the relationship between AD usage in NP treatment and the intensity of pain measured on the NRS; 2) determine the relationship between NP intensity (on the NRS) and the length of treatment with ADs at the pain clinic.
METHODS
Ethical approval for this study was provided by the Bioethical Committee at the Medical University of Warsaw, Poland, with the reference number AKBE/25/15. Informed consent was obtained from all the participants. Our cross-sectional study was conducted among patients 18 years old and older who were diagnosed with NP according to the guidelines of the Polish Society for the Study of Pain, had NP questionnaire (DN4) scores equal to or greater than four, had no earlier use of interventional therapy methods of treating NP, and who did not require simultaneous treatment of a different kind of chronic pain [24]. The tests were conducted between January 2014 and April 2018 at two pain clinics: the Department of Anaesthesiology and Intensive Care, Medical University of Warsaw, Poland, and the Medical Center of Postgraduate Education in Warsaw.
The exclusion criterion was a lack of informed consent on the part of the patient. Simultaneous use of other forms of NP pharmacotherapy did not exclude patients from the study.
Our research intervention consisted of collecting the data on the ADs taken, patients’ pain intensity in terms of NRS results, and the duration of treatment in a pain clinic.
Based on their pain intensity NRS results, the patients were divided into three groups corresponding to different levels of pain intensity: no or mild pain (NRS 0–3), moderate pain (NRS 4–6), and severe pain (NRS ≥ 7) [25].
The patients included in the study were divided into seven groups depending on the duration of treatment at the pain clinic (< 1 month, 1–3 months, 3–6 months, 6–12 months, 1–2 years, 2–5 years, and > 5 years).
These time intervals were defined based on treatment time guidelines for recurrent depression episodes proposed by other authors [21, 26, 27].
Statistical analysis
All the data collected during the study were gathered into the Microsoft Excel program of MS Office 2010 for Windows 10. Statistical analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, North Carolina, USA). Qualitative data were described by means of quantity and percentage. Qualitative outcomes were presented as percentages and compared using the χ2 test. Quantitative data were presented as mean with standard deviation (SD). Multinomial logistic regression was used to examine the quantitative relationship between the use of ADs and pain intensity. The sensitivity analysis test was used to assess the relationship between pain intensity and the use of ADs (between groups).
RESULTS
The study was conducted on a database from 421 patients. Out of the group of 421 patients under analysis, 231 (54.86%) took antidepressants.
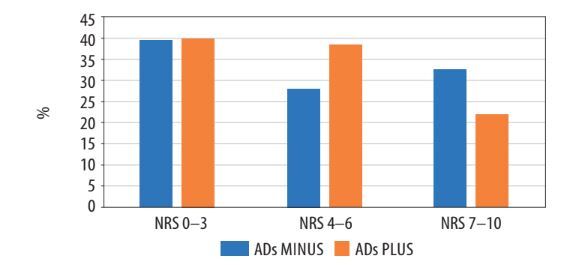
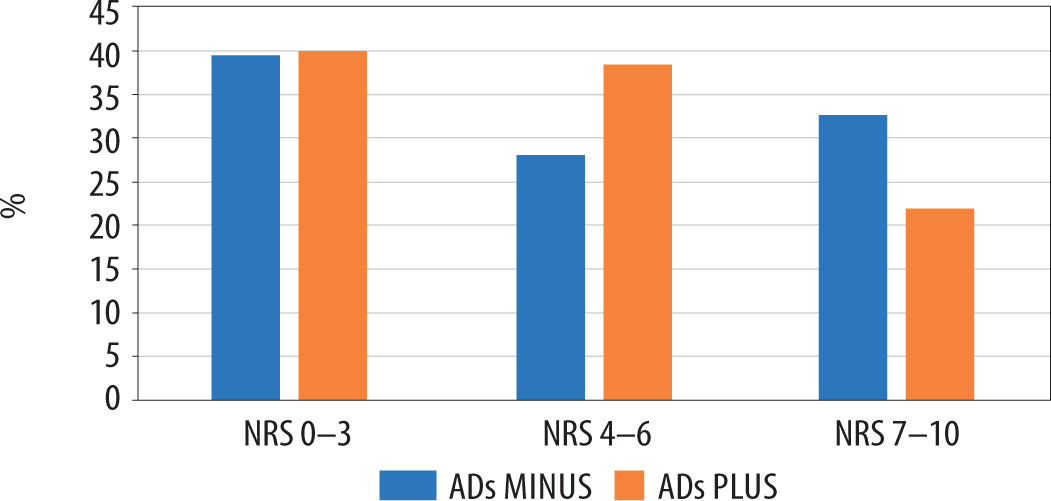
Table 2 summarizes the frequency of AD therapy used depending on the intensity of pain (divided into 3 groups according to the intensity of pain on the NRS). Based on the distribution, it appears that there is a smaller percentage of patients in the severe pain group (NRS 7–10) and a larger percentage in the moderate pain group (NRS 4–6) in the ADs PLUS patients (Figure 1). This relationship indicates that AD treatment significantly reduces the likelihood of being in the NRS 7–10 group compared to the NRS 0–3 group (OR = 0.611, 95% CI: 0.37–1.0, P = 0.05).
Table 3 shows the frequency of AD use depending on the length of treatment in the pain clinic (divided into predefined time intervals). The groups of patients taking ADs (ADs PLUS) and those not taking ADs (ADs MINUS) differ significantly (P < 0.016, χ2 test) in this respect.
When assessing the relationship between pain intensity (on the NRS) and the length of treatment with ADs at the pain clinics, a significant reduction in the likelihood of being in the NRS 7–10 group of patients was found compared to the NRS 0–3 group in ADs PLUS patients compared to ADs MINUS treated up to 24 months (OR 0.41, 95% CI: 0.22–0.75, P < 0.004). Among people treated for longer than 24 months, no relationship was observed between AD treatment and pain intensity on the NRS.
DISCUSSION
Our cross-sectional study aimed to assess the effectiveness of ADs in NP treatment by evaluating the relationship between AD usage, the intensity of pain, and the length of treatment at the pain clinic.
The results of our study confirmed the effectiveness of ADs in the treatment of NP. They showed that the use of ADs in the treatment of NP is associated with significantly lower likelihood of being in the group of patients suffering from severe pain (NRS 7–10) compared to the group of patients whose pain is well controlled (NRS 0–3) (OR = 0.611, 95% CI: 0.37–1.0, P = 0.05). In the group of patients suffering from moderate pain (NRS 4–6), a similar relationship was observed, but without statistical significance. The groups of patients with minor pain treated and untreated with ADs were comparable.
Current guidelines for NP pharmacotherapy do not directly indicate the selection of specific drugs depending on the intensity of pain (except for short- term treatment with strong opioids or their inclusion in the treatment of severe neuropathic pain secondary to cancer) [11].
The above results indicate the particular validity of including ADs in multimodal therapy for severe NP (7–10 in NRS).
Analyzing the results of our observations as well as the delay in the effects of ADs in relation to the time of their initiation described in the literature, the use of these drugs for the treatment of strong NP should be suggested as the first choice, regardless of the indications for treatment with other drugs (including strong opioids) [28].
The results of this study also indicate that the relationship between taking ADs and lower pain intensity is significant only for patients treated with them for up to 24 months.
In 2023, Birkinshaw et al. [15] noted that the assessments of effectiveness of ADs in NP were conducted for an average period no longer than 10–13 weeks. The authors suggest that there is currently no reliable evidence for the long-term efficacy of any ADs.
The authors of the discussed study found one report in the literature assessing the effectiveness of ADs in the treatment of NP over a longer period of observation. In their study, Wernicke et al. [26] evaluated the addition of duloxetine to the routine treatment of NP in the course of peripheral diabetic polyneuropathy. Under these conditions, duloxetine correlated with a statistically significant reduction in pain perception over a 52-week follow-up period (approximately 12 months).
The results of our study indicate longer (up to 24 months) effectiveness of ADs in the treatment of NP. We also did not observe the effect of ADs on the severity of NP in the group of patients treated for 2–5 years. However, it should be noted that we did not distinguish smaller subgroups from this group due to its small number.
Separate analysis of groups of patients treated for three, four, and five years could have had an impact on the extension of the two-year relationship observed in the study dependency.
The potential possibility of a longer-term impact of AD therapy on the severity of NP may be suggested by the guidelines for their use for recurrent depression episodes. Norman et al. [27] recommended use of ADs for a period of 3–5 years for these indications.
LIMITATIONS
This study has a cross-sectional nature, which potentially limits the strengths of the conclusions [29]. Regardless of the limitations resulting from the use of the research method itself, our study did not consider other elements of multimodal pharmaco-therapy in the treatment of NP.
CONCLUSIONS
Considering the limitations of the study, we conclude that the use of ADs in NP therapy may have a significant impact on reducing the frequency of severe pain intensification over a period of up to 24 months of therapy and should be included as an element of pharmacotherapy in this group of patients.