
Due to a growing demand for new treatment options for type 2 diabetes (T2DM), several classes of novel antidiabetic medications have been developed. These include glucagon-like peptide-1 receptor agonists (GLP-1RAs), dual glucose-dependent insulinotropic polypeptide receptor agonist (GIP/GLP-1RA) as well as sodium-glucose cotransporter-2 (SGLT2) inhibitors. In addition to their effects on glycaemic control, some of these medications are indicated for weight management and are therefore gaining popularity. GLP-1RAs have now become a part of an emerging treatment approach for obesity, with liraglutide being the first GLP-1RA approved by the US Food and Drug Administration (FDA) in December 2014. SGLT2 inhibitors are now authorised for the treatment of chronic kidney disease and heart failure in individuals with or without T2DM [1, 2].
Patients with T2DM are more likely to undergo some surgical procedures than those without the condition [3], partly due to vascular complications that increase their need for surgery. As the number of patients treated with novel antidiabetic drugs continues to rise, the likelihood of encountering individuals in the perioperative setting is also surging. This trend is of particular relevance to anaesthesiologists, given the emerging evidence of potential adverse effects associated with these medications.
GLP-1RAs are known to delay gastric emptying – a condition in which the stomach empties slower than normal – potentially leading to the presence of residual gastric content (RGC) in appropriately fasted patients. Clinically significant RGC, assessed by gastric ultrasound, is defined as a volume greater than 1.5 mL kg–2 [4, 5]. Evidence of increased RGC in patients receiving GLP-1RAs has been demonstrated both by endoscopy [6–8] and gastric ultrasound [9–11]. Several case reports describing episodes of pulmonary aspiration in an appropriately fasted patient on GLP-1RAs therapy have been published [12–15]. Among the side effects of SGLT2 inhibitors, euglycemic diabetic ketoacidosis (EDKA) is one of the most concerning and potentially life-threatening complications. A systematic review of 194 publications identified 42 cases of EDKA associated with perioperative use of SGLT2 inhibitors [16].
Various recommendations are available for the perioperative management of patients on GLP-1Ras or SGLT2 inhibitors [17–21]. These are based largely on expert opinion and multi-society consensus, which may lead to variations in clinical practice both regionally and globally. This review aims to familiarize anaesthetists with these novel drug classes and to present current recommendations from professional organisations. In the absence of robust evidence, uncertainty persists regarding appropriate peri-operative management.
INDICATIONS FOR NOVEL ANTIDIABETIC MEDICATIONS
GLP-1RAs and dual GIP/GLP-1 receptor agonists are approved for two main indications: T2DM and obesity. Many patients meet criteria for both conditions. In individuals with T2DM, these agents can be used throughout the course of the disease. However, in patients with established atherosclerotic cardiovascular disease, high cardiovascular risk, or chronic kidney disease, they are now recommended as first-line therapy [22].
For the treatment of obesity, GLP-1RAs and GIP/ GLP-1RAs are indicated in patients with a body mass index (BMI) ≥ 30 kg m–2, or ≥ 27 kg m–2 in the presence of at least one weight-related comorbidity, to support weight reduction [23].
SGLT2 inhibitors are indicated for three conditions: T2DM, chronic kidney disease, and chronic heart failure.
GLUCAGON-LIKE PEPTIDE RECEPTOR AND GLUCOSE-DEPENDENT INSULINOTROPIC POLYPEPTIDE RECEPTOR AGONISTS
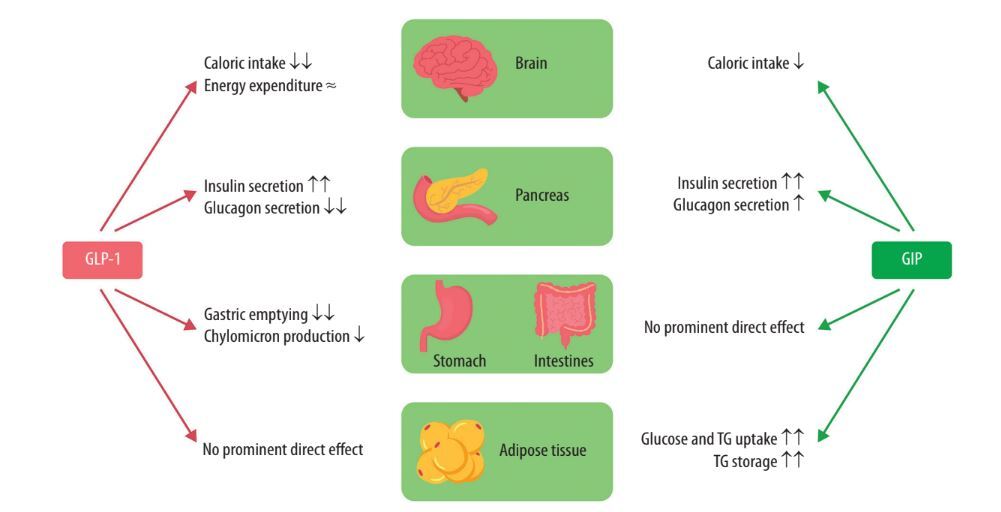
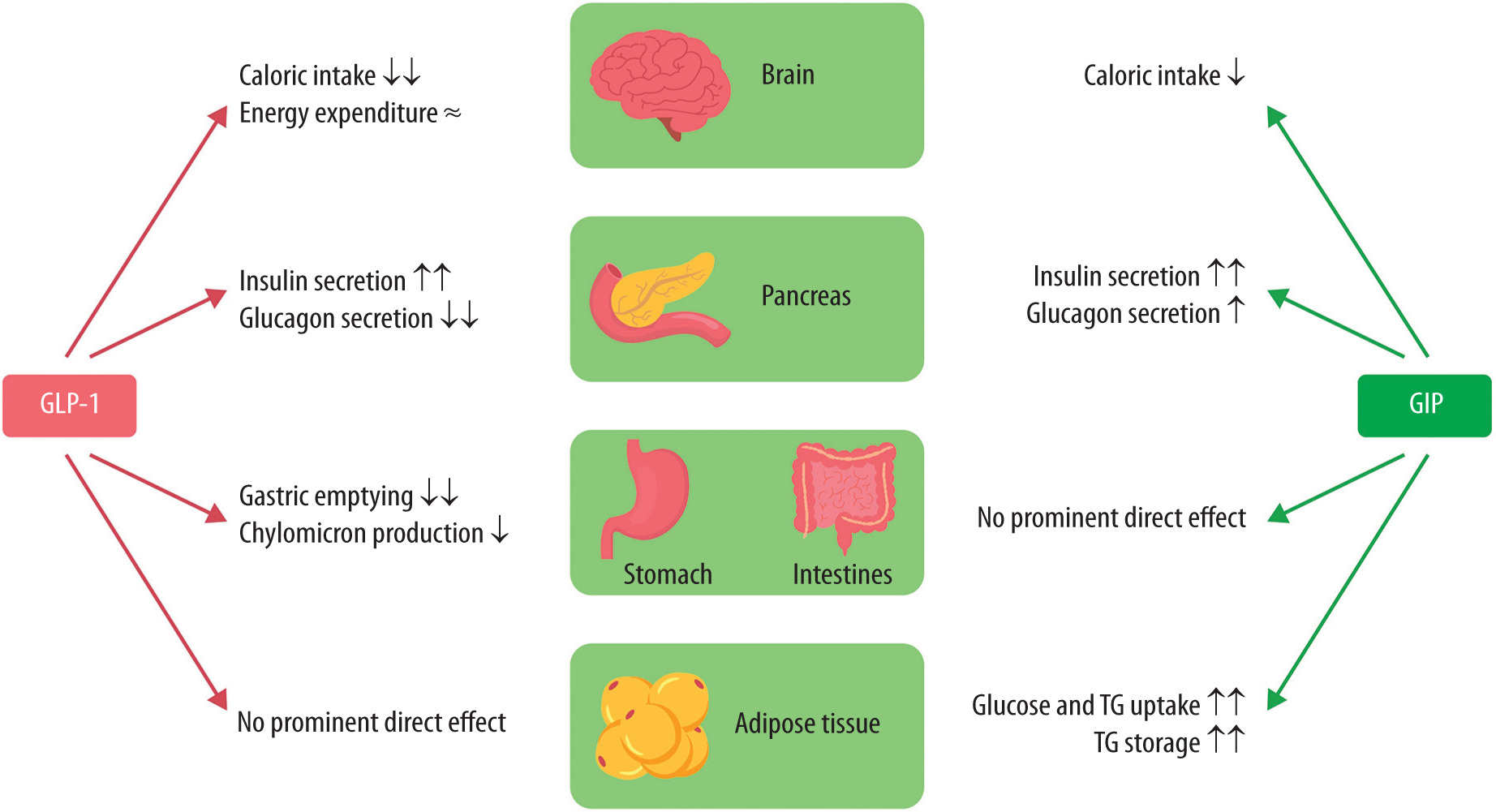
These medications act by mimicking endogenous incretins – peptide hormones secreted by the gastrointestinal system, controlled by neural mechanisms. GLP-1 is secreted physiologically by enteroendocrine L-cells of the small and large intestine, and GIP is secreted by duodenojejunal K-cells in response to food intake [23]. Activation of the GLP-1 receptor peripherally results in increased insulin secretion, reduction of glucagon secretion and slowing of gastric motility [24].
GLP-1 receptors are also widely distributed in the hypothalamus, and their activation enhances satiety, which leads to a decrease in calorie intake and consequently weight reduction [25]. Both GIP and GLP-1 are rapidly metabolised after their secretion via the enzyme dipeptidyl peptidase (DPP-4).
GLP-1RA and GIP/GLP-1RA, although structurally similar to endogenous incretins, are resistant to inactivation by DPP-4, which prolongs their effects (Figure 1).
FIGURE 1
Physiological effect of glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP)
TG – triglycerides, GLP-1 – glucagon-like peptide-1, GIP – glucose-dependent insulinotropic polypeptide
There are several GLP-1RAs and one GIP/GLP-1RA available for the management of T2DM and/or obesity. Semaglutide, liraglutide and dulaglutide are GLP-1RAs, whereas tirzepatide is a dual GIP/GLP-1RA. Tirzepatide leads to greater weight loss and is often better tolerated as compared to semaglutide, and for this reason, it is becoming more popular [25]. The high efficacy in weight loss – which is comparable to the effects of bariatric surgery – is the main driver of their rapidly increasing use. These agents have different dosages and half-life, which are summarised in Table 1.
TABLE 1
Glucagon-like peptide-1 receptor agonists (GLP-1RAs), dual glucose-dependent insulinotropic polypeptide receptor agonists (GIP/GLP-1RAs) and sodium-glucose cotransporter-2 (SGLT2) inhibitors, their dosage and half-lives
The most common side effects of this class of drugs are related to the gastrointestinal system: nausea, heartburn, vomiting, dyspepsia, diarrhoea, obstruction, and abdominal pain [26]. These adverse events typically occur at the time of treatment initiation or during dose escalation. In the SUSTAIN trial, 52% of patients receiving semaglutide experienc ed gastrointestinal side effects, compared with 35% in the placebo group. Consequently, treatment discontinuation due to adverse events occurred in 14% of patients in the semaglutide group and 8% in the placebo group [27].
PERIOPERATIVE CONSIDERATIONS FOR GLP-1RAS AND GIP/GLP-1RA THERAPY
Increased residual gastric content
There is emerging evidence that the use of GLP-1 receptor agonists is associated with increased RGC, based on studies in patients undergoing endoscopy, despite fasting for at least 8 hours [6–8]. Data from one meta-analysis indicated that there was significant reduction of RGC in patients who underwent both endoscopy and colonoscopy on the same day (OR = 0.28, 95% CI: 0.22–0.36, P < 0.00001) [6]. These findings support the conclusion that bowel preparation with osmotic laxatives, combined with the prolonged fasting required for colonoscopy, facilitates gastric content clearance. Several prospective studies have applied gastric ultrasonography to evaluate RGC observed in patients taking GLP-1RAs [5, 9–11]. This method has also demonstrated increased RGC in patients on GLP-1RAs.
Pulmonary aspiration
The risk of pulmonary aspiration in patients treated with GLP-1RAs remains uncertain. One metaanalysis from 2025 indicates that GLP-1RAs exposure is not associated with increased risk of pulmonary aspiration, but with low certainty of evidence [28]. Notably, in this meta-analysis the authors pooled evidence from 9 observational studies in which the overall incidence of pulmonary aspiration was 0.16%. As a trial sequential analysis was not performed, with such a low event rate, it is difficult to rule out the risk of statistical error type II [29]. Moreover, several reports have described episodes of pulmonary aspiration in appropriately fasted patients treated with GLP-1RAs [12–15].
Given the variability in the half-life of these drugs (Table 1), the pharmacokinetic and the pharmacodynamic profile of GLP-1RAs must also be taken into consideration. Semaglutide administered once weekly has the longest half-life of 7 days; however, one study reported that even a 10-day cessation of semaglutide was insufficient and some patients still manifested RGC on preoperative gastric ultrasound [9].
SOCIETY’S RECOMMENDATIONS FOR GLP-1RAS
The perioperative management of GLP-1RAs has been addressed by several societies, highlighting the potential risk of RGC and pulmonary aspiration. In 2024 a consensus-based guidance was formed by representatives from the American Society of Anesthesiologists (ASA), the American Gastrointestinal Association (AGA), the American Society of Metabolic and Bariatric Surgery (ASMBS), the International Society of Perioperative Care of Patients with Obesity (ISPCOP) and the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) [17]. The guidance emphasises that decisions regarding the continuation or withholding of GLP-1RAs in the perioperative period should be based on shared decision-making involving the patient, anaesthesiologist, prescribing clinician, and surgical team. Therefore, the individual patient profile and the assessment of other possible risk factors for delayed gastric emptying are particularly important. The initial step is preoperative evaluation of aspiration risk, considering factors that may predispose to delayed gastric emptying. These include the escalation phase of dosing, long-acting GLP-1RAs, higher doses, and the presence of gastrointestinal symptoms of delayed gastric emptying (e.g., nausea, vomiting and abdominal discomfort). It is crucial to recognise that both diabetes and obesity can independently affect gastric motility. Moreover, concomitantly prescribed opioids, anticholinergics and tricyclic antidepressants can delay gastric emptying. According to the consensus, patients without identifiable risk factors may continue GLP-1RA therapy during the perioperative period. However, for individuals considered at higher risk of aspiration, a liquid diet is recommended for at least 24 hours before surgery. If a decision is made to temporarily discontinue GLP-1RA therapy, the duration of cessation should follow the guidance of the ASA: on the day of the procedure for daily formulations, and one week prior to surgery for weekly formulations [17]. It is important to note that discontinuing GLP-1RAs in patients with T2DM may increase the risk of perioperative hyperglycaemia, which has been associated with higher incidence of postoperative complications such as wound infection, delayed wound healing and prolonged hospital stay [30].
In accordance with ASA recommendations, the European Society of Anaesthesiology and Intensive Care (ESAIC) advises withholding weekly formulations of GLP-1RA at least one week before surgery and daily formulations on the day of surgery. Moreover, the ESAIC points out that all patients treated with GLP-1RAs could possibly have gastric content despite the absence of gastrointestinal symptoms and recommends a clear liquid diet the day before the procedure. For patients receiving GLP-1RA for weight management the ESAIC provides more restrictive recommendations and advises considering withholding the drug at least three half-lives [21].
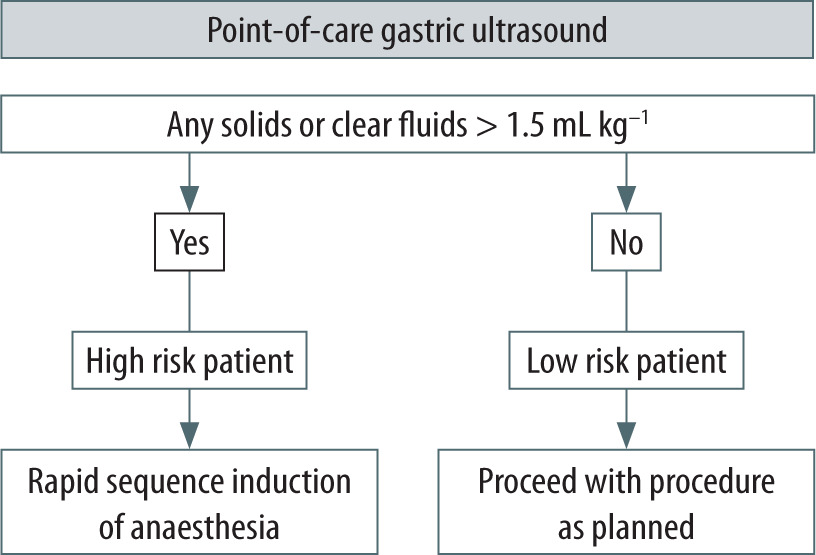
Conversely, the UK multidisciplinary consensus statement recommends continuing GLP-1RA therapy in the perioperative period, but states that it should be supported through risk assessment and stratification, shared decision-making and the use of peri-operative techniques to mitigate risk of pulmonary aspiration [18]. Performing preoperative point-of-care gastric ultrasound in patients who continue GLP-1RA therapy appears to be an appropriate strategy (Figure 2). This approach may help identify patients at increased risk of aspiration, preventing unnecessary surgical delays or cancellations, and enhance patient safety. Although not yet widely adopted, point-of-care gastric ultrasound is likely to become more integral to perioperative management. Some authors suggest that it might have limited application due to its variability [31]. Studies have shown that performing 33 supervised gastric ultrasound examinations is required to achieve a 95% accuracy rate in qualitative assessment of gastric content [32]. Furthermore, this method might be technically challenging in patients with obesity. For patients identified as high risk on the day of the procedure, rapid sequence induction (RSI) of general anaesthesia may be considered, or regional anaesthesia may be used if feasible [17].
FIGURE 2
Assessment of residual gastric content using point-of-care gastric ultrasound on the day of the procedure
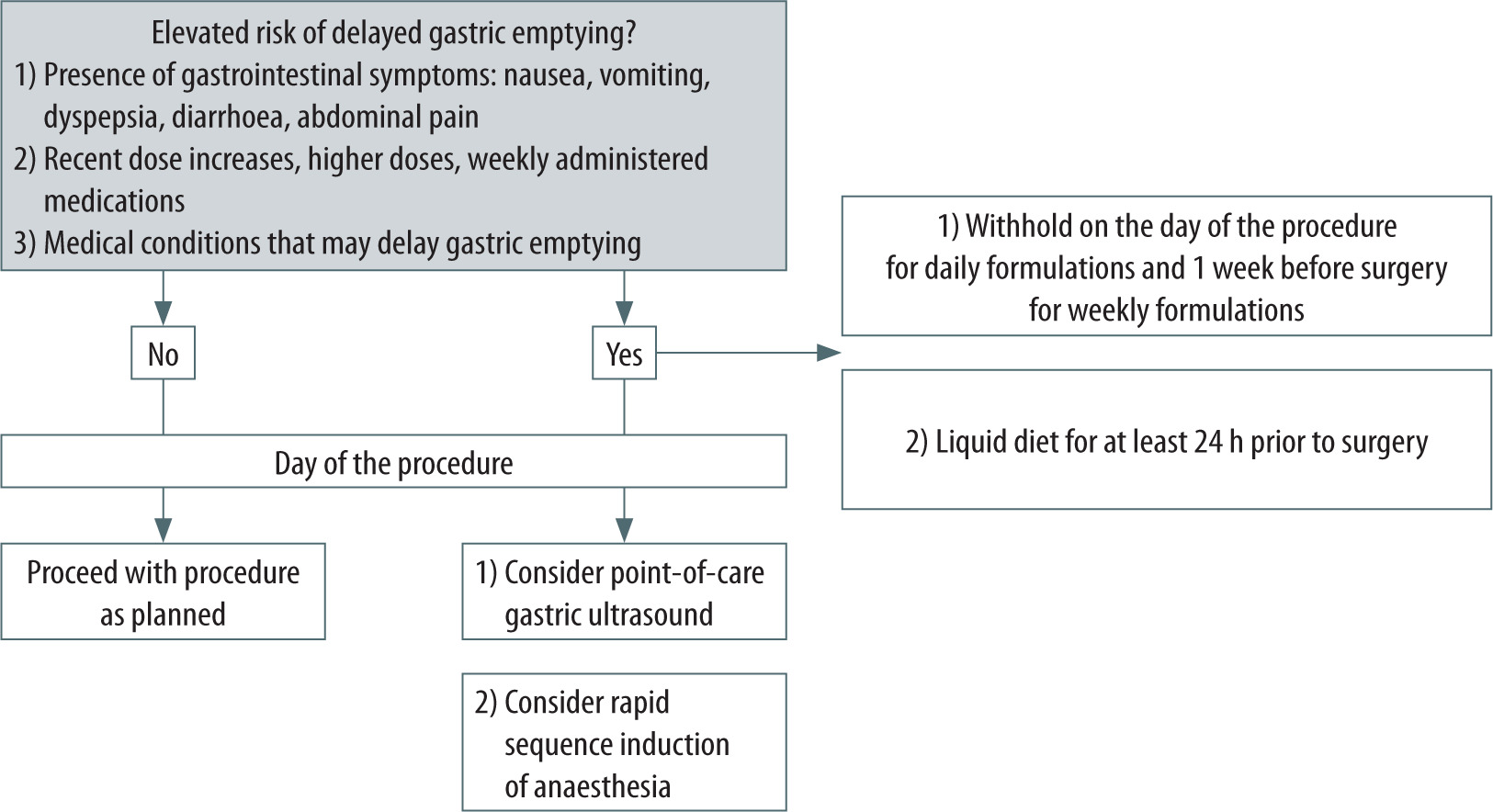
In conclusion, the ASA multi-society consensus provides practical recommendations for the perioperative management of patients receiving GLP-1RAs (Figure 3). However, it is important to note that these recommendations are based on expert opinion rather than high-level evidence.
SODIUM-GLUCOSE COTRANSPORTER-2 INHIBITORS
SGLT2 inhibitors are a class of agents that facilitate glycaemic control by inhibiting renal glucose reabsorption, thus stimulating glycosuria. There are three commonly used agents: canagliflozin, dapagliflozin and empagliflozin. In addition to their glycosuric effect, SGLT2 inhibitors confer multiple cardiovascular and renal benefits, particularly in patients with chronic heart failure – both with reduced and preserved ejection fraction – as well as those with chronic kidney disease.
Importantly, these cardiovascular and renal benefits are seen in both patients with and those without T2DM [33, 34]. Nowadays, SGLT2 inhibitors are approved for the treatment of chronic heart failure and chronic kidney disease. In T2DM they have become the foundation of pharmacotherapy, just as in chronic heart failure.
The excretion of glucose in the urine lowers the patient’s insulin levels and increases glucagon concentrations [35]. Such a modulatory effect induces compensatory lipolysis, hepatic gluconeogenesis and ketogenesis, and it may lead to development of diabetic ketoacidosis (DKA), particularly EDKA, in patients with insufficient endogenous insulin secretion. EDKA may occur when the blood glucose level is within or near the normal range. The ability of glucose to enter cells is reduced; thus, cells utilize triglycerides and fatty acids as an alternative energy source. The increased lipolysis may lead to ketonemia, ketonuria, and in rare cases to metabolic acidosis. Importantly, an asymptomatic mild increase in plasma ketone concentrations with no signs of ketoacidosis is often noted in SGLT2 inhibitor users and should not be a cause for concern as it clearly results from the mechanism of action of this class of drugs. Additionally, this mild hyperketonaemia is believed to contribute to cardioprotective and renoprotective effects of SGLT2 inhibitors [35]. However, as SGLT2 inhibitors enhance renal reabsorption of ketone bodies by reducing sodium reabsorption in the kidneys, some patients – particularly those with low insulin production (e.g. lean individuals with T2DM) – may develop ketoacidosis without the presence of ketonuria. Therefore, the presence of urinary ketones is not a reliable marker for detecting SGLT2 inhibitor-associated euglycaemic ketoacidosis). Biochemical criteria for diagnosis include serum ketones > 3 mmol L–1, pH < 7.3, serum bicarbonate concentration < 15 mmol L–1 and anion gap > 12 mmol L–1 [36].
FIGURE 3
Summary of recommendations from the multisociety clinical practice guidance on the perioperative use of GLP-1 receptor agonists, developed by representatives of the American Society of Anaesthesiologists
Although the occurrence of EDKA associated with SGLT2 inhibitors is rather rare, several predisposing factors have been recognised. These include surgery, infection, dehydration, fasting and reduced carbohydrates intake, and – in patients with type 1 diabetes – too drastic reduction of insulin dose. It is worth noting that the use of SGLT2 inhibitors in type 1 diabetes is off label but occurs in patients with erratic glucose fluctuations or advanced chronic heart failure or chronic kidney disease. In cohort studies SGLT2 inhibitors were associated with a two-fold increased risk of EDKA as compared with GLP-1RAs; therefore, they have become a potential management issue perioperatively [37]. SGLT2 inhibitors might not cause EDKA by themselves but instead create a predisposition that can lead to the condition when certain triggering factors are present. Apart from the surgical procedure itself, most of these triggers commonly occur in the perioperative period. A retrospective review of 1307 patients receiving SGLT2 inhibitors who underwent surgical procedures demonstrated an incidence of EDKA of 0.2% in elective surgery, compared to 1.1% in emergency procedures, given the inability to withhold SGLT2 inhibitors in the latter group [38]. These emerging data have raised concerns among anaesthesiologists and brought into question the optimal time to withhold this class of medications. In the perioperative management of patients taking SGLT2 inhibitors, the optimal approach for preventing EDKA is to withhold the medication in any setting where predisposing factors for ketoacidosis are present (e.g. surgery, infection, dehydration). There are various recommendations on when these drugs should be stopped in the perioperative period. The ESAIC recommends withholding this class of drugs for three to four days before elective surgery. Consistent with this recommendation, the FDA also advises withholding SGLT2 inhibitors for three days [20, 21]. In turn, the UK Medicines and Healthcare product Regulatory Agency (MHRA) and the UK multidisciplinary consensus statement guidance suggests that these drugs should be withheld the day before planned surgery [18, 39]. However, a review of nearly 100 case reports on perioperative DKA suggested that preoperative cessation of the drug for more than two days did not result in DKA occurrence [40]. Given that the half-life of SGLT2 inhibitors varies from 11 to 13 hours, it seems reasonable to withhold these medications for three days (or five half-lives) before elective surgery. These medications should be recommenced once the patient is clinically well, euvolemic and tolerating an oral diet. However, practitioners must stay alert to the potential development of EDKA and monitor patients for any symptoms of ketoacidosis (nausea, vomiting, abdominal pain).
TABLE 2
Recommendations for the perioperative management of patients taking glucagon-like peptide-1 receptor agonists (GLP-1RAs), dual glucose-dependent insulinotropic polypeptide receptor agonists (GIP)/GLP-1RAs and sodium-glucose cotransporter-2 (SGLT2) inhibitors
[i] GLP-1RAs – glucagon-like peptide-1 receptor agonists, GIP/GLP-1RAs – dual glucose-dependent insulinotropic polypeptide receptor agonists, SGLT2 inhibitors – sodium-glucose cotransporter-2 inhibitors, ASA – American Society of Anesthesiologists, ESAIC – European Society of Anaesthesiology and Intensive Care; RSI: rapid sequence induction
PRACTICAL RECOMMENDATIONS
Clinicians should be aware of the potential perioperative risk in patients receiving GLP-1RAs, GIP/ GLP-1RA and SGLT2 inhibitors. Current evidence is insufficient to provide clear recommendations on the optimal drug cessation before elective surgery. Regarding GLP-1RAs, the ASA recommends continuation of therapy in the preoperative period if there is no evidence of delayed gastric emptying. However, it is important to note that both indications for these agents – T2DM and obesity – are themselves associated with impaired gastric motility. An individualised, shared decision-making approach is re commended. In patients continuing GLP-1RA therapy, the use of point-of-care gastric ultra sound may be a reasonable strategy to enhance patient safety and prevent unnecessary surgical cancellations. The ASA does not specifically address the management of patients taking GIP/GLP-1RAs; however, given the similarity in their mechanism of action, applying the same recommendations appears appropriate. According to the ESAIC and the FDA, patients taking SGLT2 inhibitors should withhold these medications three days before surgery. Furthermore, the Polish Diabetes Association has addressed the issue of the optimal timing for the cessation of SGLT2 inhibitors and GLP-1RAs, recommending withholding SGLT2 inhibitors for three days prior to surgery and omitting one dose of weekly administered GLP-1RA [41]. We summarised the current evidence and available recommendations from the ASA and ESAIC to support clinicians in the perioperative management of patients receiving SGLT2 inhibitors, GLP-1RAs and related therapies (Table 2).
DIRECTIONS FOR FUTURE RESEARCH
The clinical use of GLP-1RAs and dual GIP/GLP-1RAs has risen sharply in recent years, driven by their proven efficacy in managing T2DM and obesity. Despite their growing use, the optimal perioperative management of patients receiving these agents remains uncertain. Current guidelines recommend continuing GLP-1RA therapy during the perioperative period; however, emerging evidence suggests a potential association with increased RGC, even in adequately fasted patients. Ongoing studies aim to further elucidate the perioperative safety profile of these therapies.
Importantly, two randomised controlled trials (NCT06839248, NCT06654219) investigated the effect of 24-hour clear liquid diet compared to standard fasting guidelines on gastric contents assessed by gastric ultrasound. In the absence of robust, high-quality evidence, clinical decisions should be guided by individual risk assessment and shared decision-making. Data from the meta-analysis by Elkin et al. [28] suggest that patients who omitted at least one dose of their GLP-1RA prior to surgery had a lower risk of RGC compared to those maintained on a regular dosing regimen. However, this evidence is derived from small observational studies and should be interpreted with caution. While current data do not show a clear association between GLP-1RA use and pulmonary aspiration, further research is needed to evaluate the risk of this potentially life-threatening complications. At the same time, withholding GLP-1RAs in the perioperative period is not without risk, as it may lead to suboptimal glycaemic control and loss of the cardiometabolic benefits associated with continued therapy [28, 42].
Performing a preoperative assessment of RGC using point-of-care gastric ultrasound in patients continuing GLP-1RA or GIP/GLP-1RA therapy has been suggested by experts and professional societies as a risk mitigation strategy to reduce the potential for aspiration and enhance perioperative safety [17, 28, 43].
In summary, there is a pressing need for large-scale, prospective studies to determine the optimal timing for perioperative cessation of GLP-1RAs, GIP/ GLP-1RAs, and – looking ahead – emerging triplehormone receptor agonists [44]. These studies should evaluate the impact of varying cessation intervals on gastric emptying and aspiration risk across different patient populations, including those with obesity, diabetes, delayed gastric emptying, or undergoing high-risk procedures. Such data are essential to guide evidence-based, multidisciplinary perioperative management strategies.