
Aspiration of gastric contents may complicate an otherwise uneventful anaesthetic [1]. Preoperative fasting for surgical patients is necessary to prevent this complication [2]. While preoperative fasting is a traditional strategy to mitigate the risk of perioperative regurgitation and aspiration, it does not offer complete protection [3, 4]. Rapid sequence induction and intubation (RSI) is popular to further optimise perioperative airway management and minimise regurgitation and aspiration.
Key strategies to reduce the risk of aspiration include the application of cricoid pressure (CP), avoidance of positive-pressure ventilation prior to securing the airway with tracheal intubation, and performing laryngoscopy only after full neuromuscular blockade has been achieved [5, 6].
During RSI, the CP manoeuvre applies manual force over the cricoid cartilage to compress the underlying oesophagus against the cervical vertebrae, potentially obstructing the passage of gastric contents [7]. Several factors may compromise the effectiveness of CP in preventing aspiration during RSI. These include operator technique (hand placement and applied force), patient characteristics (neck circumference), and anatomical variations (oesophageal position) [8].
Anatomical considerations further limit the effectiveness of CP. Up to 50% of patients exhibit a left-sided oesophageal position. This difference in anatomy might make it harder for the cricoid manoeuvre to completely block the oesophagus, which could make it less effective at stopping passive regurgitation of stomach contents [9]. Moreover, oesophageal mobility can further compromise the effectiveness of CP. Research has shown that in some patients, the oesophagus already resides on the left side, and the application of cricoid force may even accentuate this displacement. The potential for further leftward movement of the oesophagus during the manoeuvre raises concerns about its ability to consistently achieve complete oesophageal occlusion [10–12].
Despite achieving anatomical alignment, the potential impact of CP on the lower oesophageal sphincter (LES) may limit its efficacy. Studies suggest that CP itself may decrease LES tone [13, 14]. Even with the oesophagus compressed, this relaxation could weaken the barrier against regurgitation. These observations highlight the potential shortcomings of CP as a standalone strategy for preventing aspiration.
Recent guidelines and reviews highlight the controversies surrounding the use of CP including use of supraglottic devices for aiding intubation [15, 16]. CP could potentially hinder the effectiveness of bagmask ventilation, which is a crucial step in securing the airway [17]. The role of CP in RSI remains a topic of discussion. A large randomised controlled trial suggested that the use of this technique may prolong intubation time and worsen the laryngoscopic view [18]. This raises concerns about potential hindrances to successful tracheal intubation. While some studies have indicated that CP effectively prevents gastric insufflation, others have reported air bypassing the compressed area at high airway pressures [19]. Additionally, documented cases of regurgitation despite CP application highlight its limitations [20, 21]. These findings suggest CP may not be a foolproof measure and indicate the need for a multifaceted approach to minimizing aspiration risk during RSI.
Two terms have been proposed as an alternative to CP. The term “paralaryngeal pressure” was described as the pressure applied paralaryngeally at the level of cricoid, with the pressure vector directed medially at an angle of 45° towards the vertebral column [22]. “Paratracheal pressure” (PP) is the pressure applied at the left side of the patient’s trachea, immediately above the left clavicle and medial to the sternocleidomastoid muscle [23].
The study by Andruszkiewicz et al. [22] employed ultrasound technology to investigate the effectiveness of CP. Their findings suggested that applying CP may compress the oesophagus, not at the cricoid cartilage level itself but rather on the left paratracheal side at that level. Researchers have found that paratracheal pressure (PP) may be a better way to block the oesophagus and keep air from going into the stomach during mask ventilation than CP [24, 25]. Emerging evidence suggests PP as a potential alternative to CP during RSI.
However, before implementing paratracheal compression in our practice, it is important to research any negative effects, such as how it may affect the glottic vision during direct laryngoscopy. This study aimed to perform a comparative analysis of PP and CP regarding their impact on the laryngeal view during direct laryngoscopy. We tested the hypothesis that PP would not deteriorate the glottic view during direct laryngoscopy, compared to CP. In addition to the primary outcome, the investigation encompassed the evaluation of the secondary outcomes, ease of mask ventilation, change in peak inspiratory pressure (PIP) during mechanical mask ventilation, ease of tracheal intubation, and resistance encountered while advancing the tube into the glottis.
METHODS
This study was conducted between December 2022 and January 2024, following approval from the Institutional Ethics Committee, Indira Gandhi Institute of Medical Sciences, Patna, India (707/ IEC/IGIMS/2022 dated 06/10/2022). The study was prospectively registered with clinical trial registry, India (www.ctri.nic.in) vide registration no. CTRI/2022/11/047679, dated 25/11/2022. All participants provided written informed consent before enrolment in the study. This study complied with the 2013 revisions to the Helsinki Declaration. It was a parallel group, randomized, double-blind, noninferiority trial conducted at a university hospital.
The inclusion criteria were patients of American Society of Anesthesiologists (ASA) 1 and 2, patients between 18 and 75 years of age with no sex restrictions, patients able to comprehend and willing to participate, and patients scheduled for general elective surgery.
Exclusion criteria included patient’s refusal to participate, patients who were at risk for gastric regurgitation, patients with a history of surgery of the neck or oesophagus, patients with stenosis or bruit of the left carotid artery, and patients with a history of stroke or acute coronary syndrome in the preceding 3 months.
The application of PP and CP before the study period was practised. We used a 50 mL syringe model to train for applying the correct force. Force compressing the volume of a syringe filled with air from 50 to 33 mL was measured as 30 N using a scale. In the cricoid group, CP was applied with a single-handed 3-finger manoeuvre [26]. Standard fasting guidelines with no sedative premedication were ensured in all patients. Before anaesthetic induction, standard monitoring was initiated, including lead II electrocardiogram, non-invasive arterial blood pressure, and pulse oximetry. Additionally, an intravenous access was secured on the dorsum of the left hand. Baseline vital signs, encompassing heart rate (HR), mean arterial pressure (MAP) and oxygen saturation (SpO2), were documented. The patients were allocated randomly according to computer-generated random numbers to one of two groups using sealed envelopes. Group P: patients in whom PP was applied. This manoeuvre targeted a force of 30 N directed against the vertebral body at a specific location: the left side of the patient’s trachea, immediately superior to the left clavicle and medial to the sternocleidomastoid muscle. Group C: patients in whom CP was applied using a standardised single-handed, three-finger manoeuvre.
Anaesthetic induction was achieved using a standardised regimen of intravenous medications: fentanyl (2 μg kg–1), propofol (2 mg kg–1), and rocuronium bromide (0.6 mg kg–1). To maintain airway patency during both manual and mechanical ventilation phases, an oropharyngeal airway was inserted in all participants.
A 5 to 12 MHz linear ultrasound transducer was employed to assess the transverse spatial relationship between the oesophagus, trachea, and cricoid cartilage in each patient. The examination specifically targeted the lower-left paratracheal region and the area encompassing the cricoid cartilage. Based on the ultrasound findings, the oesophageal position relative to the trachea and cricoid cartilage was categorized into five distinct groups: left – the oesophageal lumen deviated entirely to the patient’s left side, with no overlap on the trachea or cricoid cartilage; partial left – the oesophageal lumen partially overlapped the left side of the trachea or cricoid cartilage; middle – the oesophageal lumen completely overlapped the trachea or cricoid cartilage poste riorly; partial right – the oesophageal lumen partially overlapped the right side of the trachea or cricoid cartilage; right – the oesophageal lumen deviated entirely to the patient’s right side, with no overlap on the trachea or cricoid cartilage.
The ease of manual bag-mask ventilation during intervention application was assessed using a standardised 4-point scale: easy – ventilation was achieved effortlessly while the assigned manoeuvre was maintained; moderate – adequate ventilation was established by increasing fresh gas flow or adjusting the pressure limiting valve; difficult – insufficient ventilation volume despite increased airway pressure; impossible – ventilation was undetectable with the allocated manoeuvre in place, accompanied by the absence of exhaled carbon dioxide. Following the release of the assigned manoeuvre, mechanical ventilation was established via a facemask to evaluate potential airway obstruction.
Changes in expired tidal volume and PIP were documented. A volume-controlled ventilation mode was employed with the following parameters: tidal volume 8 mL kg–1; respiratory rate 12 breaths min–1; positive end-expiratory pressure (PEEP) 5 cmH2O; inspiratory-to-expiratory ratio (I : E) 1 : 2. Sevoflurane in oxygen (6%) was used for anaesthesia maintenance. A two-handed technique ensured a proper facemask seal. Baseline PIP was recorded before repeating the measurements while reapplying the allocated intervention. Data collection for all ventilation parameters occurred only after reaching a steady state.
The impact of each manoeuvre on achieving a favourable laryngoscopic view was evaluated. This assessment compared the incidence of a compromised glottic view during direct laryngoscopy with the allocated manoeuvre in place versus the view obtained without the manoeuvre. Sequential glottic visualizations, both with and without the assigned manoeuvre, were graded using the modified Cormack-Lehane scale as the primary endpoint of the study [27, 28]. “Deterioration” in modified Cormack-Lehane grade was defined as a decrease of glottis exposure (e.g., ≥ 1 grade change). If the allocated manoeuvre was released as a rescue step to complete tracheal intubation, it was recorded along with the reason for release of the manoeuvre. After evaluating the laryngoscopic view, tracheal intubation was conducted during the application of each intervention. All intubations were performed using a Macintosh laryngoscope of appropriate size without use of any intubation adjuncts (e.g., stylets or bougies).
Tube resistance while advancing the tracheal tube through the glottis was evaluated on a 4-point scale: slight, moderate, severe, and obstructed. The ease of tracheal intubation was assessed using a standardised 4-point scale: easy – the trachea was successfully intubated on the first attempt; moderate – the trachea was intubated after multiple attempts or with the need for increased laryngoscopic force; difficult – the trachea was intubated only with the aid of tracheal tube modification (e.g., stylet insertion); impossible – the trachea could not be intubated. The duration of intubation was documented. This measurement encompassed the time between the initial insertion of the tracheal tube into the oral cavity and the confirmation of capnography, signifying successful carbon dioxide detection. If the allocated manoeuvre (either PP or CP) needed to be released to facilitate successful tracheal intubation, these cases were documented. Additionally, the specific rationale for manoeuvre release was recorded.
Blinding
Group allocation was concealed from the clinician performing mask ventilation and tracheal intubation by an opaque drape strategically positioned to cover the patient’s neck and the hand of the manoeuvre provider. This drape remained in place until successful tracheal intubation was achieved. An independent anaesthesiologist performed group allocation, further ensuring that the clinician performing the procedures remained unaware of the assigned intervention (either PP or CP). Both patients and those directly assessing airway patency and intubation ease were blinded to the group allocation.
Primary outcome
Incidence of deteriorated laryngoscopic view evaluated by the modified Cormack-Lehane grade.
Secondary outcome
Ease of mask ventilation, change in PIP during mechanical mask ventilation, ease of tracheal intubation, and resistance encountered while advancing the tube into the glottis.
Sample size and statistical analysis
Based on the study by Won et al. [29], the incidence of the modified Cormack-Lehane grade was observed as the primary outcome, occurring in 3% of the subjects in the active control group (CP) and 0% in the test group (PP). To achieve a power of 80% and a level of significance of 2.5% for stating that the PP is not inferior to the active CP at a –10% margin of non-inferiority (assuming that a larger proportion is desirable) and after applying continuity correction, the study required a sample size of 100 for each group, i.e., a total sample size of 200, assuming equal group sizes [30].
All data were entered into an MS Excel file with coded variables. Stata Version 10 (Stata Corp, Houston, Texas, USA) was used for data analysis. Continuous variables were assessed for normality using the Shapiro-Wilk test. Normally distributed continuous variables were summarised using mean and standard deviation, with 95% confidence intervals (CI). Non-normally distributed variables were summarised using median and inter-quartile range (IQR). Categorical variables were presented as proportions, and the independence of attributes was assessed using the χ2 test to evaluate associations. Patient demographics and baseline characteristics were assessed for balance between the two groups using absolute standardised differences. Any characteristic exceeding a 0.2 threshold in the absolute standardised difference was evaluated in the clinical context to determine potential imbalances. Logistic regression was applied to adjust for the confounding effect due to potential imbalances of some independent variables.
The primary outcome measure, deterioration of the laryngoscopic view, was evaluated using the modified Cormack-Lehane grade. A non-inferiority analysis was conducted to compare PP with CP, employing a two-sided 95% CI. Non-inferiority was concluded if the upper bound of the 95% CI for the difference in deterioration of laryngoscopic view was less than –10%. This 10% non-inferiority margin was predetermined, reflecting a clinically acceptable level of difference given the known incidence of view deterioration with CP. Secondary outcomes, including intubation duration and changes in various variables before and after the manoeuvre, were analysed using appropriate statistical tests depending on data normality. Normally distributed data underwent analysis via independent t-tests, while non-normally distributed data were subjected to Mann-Whitney U tests. Ordinal data, including scores related to ease of ventilation or intubation, were analysed using ordinal logistic regression. This method facilitated the calculation of odds ratios (OR) to quantify the likelihood of experiencing a worse outcome (e.g., greater difficulty) in the PP group compared to the CP group.
RESULTS
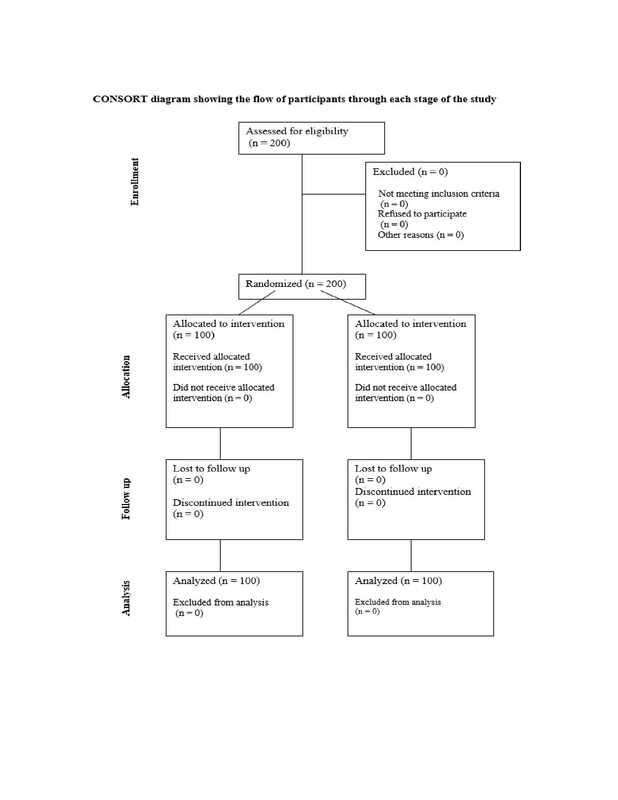
Two hundred patients were screened for eligibility, and no dropouts occurred at any stage of the study. Data from all 200 patients were included in the analysis (Figure 1).
Table 1 outlines a comparative analysis of demographic and clinical characteristics between the groups. The ultrasonographic findings showed that 86 participants (86%) in the paratracheal group had oesophagus on the left and 14 (14%) on the partial left. In the cricoid group, 67 participants (67%) had it on the left and 33 (33%) on the partial left. Bag mask ventilation was easy in 92% patients of the paratracheal group and 95% in the cricoid group. Fisher’s exact test indicated no significant difference (P = 0.558).
Table 2 outlines the baseline comparison of continuous variables between the paratracheal group and the cricoid group. All these variables were comparable.
Table 3 outlines the comparison of incidence of deteriorated laryngoscopic view after application of paratracheal and CP. At the baseline i.e., before the intervention, there was no significant difference in the proportion of various laryngoscopic views between the two groups (χ2 with 2 d.f. = 4.975, P = 0.083). However, after the intervention, there was a significant difference in the proportion of various laryngoscopic views between two groups (χ2 with 2 d.f. = 12.996, P = 0.002). Logistic regression analysis was performed to evaluate the difference of views between two groups after controlling for the sex and ultrasonographic variables. For that, three dummy variables were created: full view vs. others, partial view vs. others, and only arytenoids vs. others, for comparing laryngoscopic views in the two groups. We did not observe any significant difference between the two groups when comparing the proportion of full view vs. other, as the adjusted OR, after adjusting for sex and ultrasonography, with 95% CI, was 0.84 (0.44–1.59), P = 0.595, whereas the adjusted OR with 95% CI for partial view vs. others was 1.68 (0.87–3.29), P = 0.119. However, for only arytenoids vs. other, the OR with 95% CI was 0.19 (0.05–0.723), P = 0.015, indicating deterioration of laryngoscopic view in the cricoid group as compared to the paratracheal group.
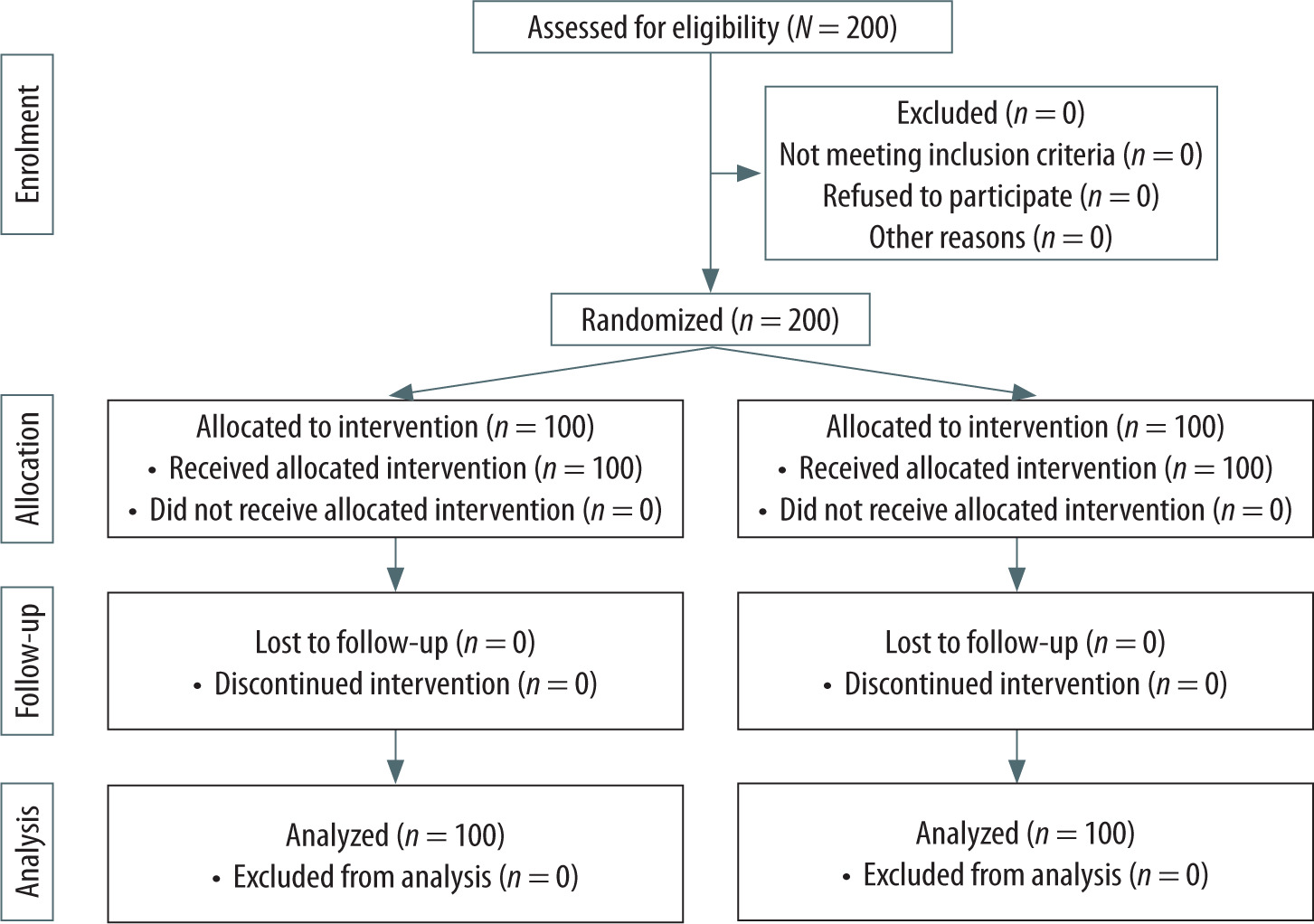
TABLE 1
Baseline comparison of categorical variables between the paratracheal group and the cricoid group
TABLE 2
Baseline comparison of continuous variables between the paratracheal group and cricoid group
TABLE 3
Comparison of modified Cormack and Lehane grade (MCLG) in two groups during intubation
TABLE 4
Number of worsened laryngoscopic views
| MCLG | Paratracheal group (n = 100) | Cricoid group (n = 100) | Risk difference | 95% CI |
|---|---|---|---|---|
| 2B | 0 (0%) | 20 (20%) | –20% | –26.68 to –13.32 |
| 2A | 0 (0%) | 23 (23%) | –19% | –27.83 to –8.16 |
Table 4 outlines PP’s demonstrated non-inferiority to CP in its effect on the laryngoscopic view. Specifically, none of the patients in the paratracheal group experienced deterioration in the laryngoscopic view as evaluated by the modified CormackLehane grade, whereas partial view of the glottis decreased from 42% at baseline to 23% after intubation in the cricoid group as compared to 0% in the paratracheal group (0% to 19%; absolute risk difference, –19%; 2-sided 95% CI: –27.83 to –8.16%; P < 0.001). Furthermore, in 20 patients arytenoids were visible after intubation, indicating deterioration of laryngoscopic view in the cricoid group (0% vs. 20%; absolute risk difference, –20%; 2-sided 95% CI: –26.68 to –13.32; P < 0.001).
Table 5 outlines a summary of the effects of paratracheal and cricoid manoeuvres on mask ventilation and intubation. The ease of manual bag-mask ventilation, assessed on a 4-point scale, was found to be greater in the paratracheal group compared to the cricoid group. However, this difference did not reach statistical significance (OR = 0.60, 95% CI = 0.15–2.17, P = 0.2840).
Intubation ease and resistance during tracheal tube passage showed significant differences between the two groups. Ease of intubation was significantly higher in the paratracheal group, with an OR of 3.57, a 95% CI of 1.92–6.67, and a P-value of 0.0001. Additionally, the odds of observing slight resistance was significantly better in the PP group when passing the tracheal tube into the glottis, with an OR of 16.67, a 95% CI of 7.14–40, and a P-value < 0.001.
The duration of intubation, measured in seconds, did not show a statistically significant difference between the two groups. This was determined using the Mann-Whitney U test, with a z-value of –1.197 and a P-value of 0.235.
Table 6 shows that there was no significant difference in PIP at baseline between paratracheal and cricoid groups (P = 0.412). The increase in PIP was significantly smaller in the paratracheal group (0.47 (0.31–0.63) vs. 1.46 (1.22–1.69), P = 0.002). The difference in the paired comparison between the two groups showed more significant changes in the cricoid group as compared to the paratracheal group (P < 0.001).
TABLE 5
Effects of mask ventilation and intubation
TABLE 6
Comparison of peak inspiratory pressure (PIP) in two groups before and after
There was no significant difference in HR or MAP between the groups and no incidence of desaturation was reported. Sequential assessments (with/ without manoeuvre) were performed as per standard sequence of care and keeping in view patient safety, e.g. minimizing apnoea time, without any influence on the results.
DISCUSSION
The primary aim of this study was to compare the effects of paratracheal and CP on the laryngoscopic view during intubation, as well as other secondary outcomes.
In our study, we found that PP was non-inferior to CP in terms of its effect on the laryngoscopic view. None of the patients in the paratracheal group experienced a deteriorated laryngoscopic view, whereas 20% of patients in the cricoid group did. This indicates that PP may be a viable alternative to CP in preventing a worsened laryngoscopic view during intubation, being more effective in achieving oesophageal compression in our patient population.
The demographic characteristics, including sex distribution, ASA classification, and body mass index (BMI), showed some differences between the groups. Specifically, there was a significant sex imbalance, with a higher proportion of males in the paratracheal group (65%) compared to the cricoid group (41%). While this could introduce bias, the randomization process helps mitigate potential impacts on the study outcomes.
Mask ventilation, measured on an ordinal scale, was found to be easier with a paratracheal group than with cricoid group. Ease of intubation was significantly better in the paratracheal group compared to the cricoid group.
Another important finding of our study was that the difference in PIP was significantly lower in the paratracheal group compared to the cricoid group after the intervention (P = 0.0001). This suggests that PP may result in better ventilation dynamics compared to CP.
The resistance encountered during intubation was also significantly different between the two groups. This suggests that PP may reduce the difficulty of advancing the tube into the glottis compared to CP.
A significant difference was observed in the ease of intubation between the two groups. The paratracheal group had a higher proportion of easy intubations (73%) compared to the cricoid group (43%). This finding suggests that PP may facilitate a smoother and less complicated intubation process than CP.
The difference in intubation duration was not statistically significant, suggesting that the time required for intubation was equivalent for both techniques.
Our findings are similar to those of Won et al. [29], who concluded that PP was non-inferior to CP regarding the incidence of deterioration of modified Cormack and Lehane grade (P < 0.001). Mask ventilation was easier with PP than with CP (OR, 0.41; 95% CI, 0.21–0.79; P = 0.008). The increase in PIP was significantly smaller in the PP group (P = 0.001). The differences in other secondary outcomes were comparable.
Another non-inferiority trial comparing left PP to CP for successful laryngeal mask airway (LMA) insertion in adult patients found that left PP was effective for LMA insertion and did not demonstrate greater adverse effects compared to CP [31].
A non-inferiority trial compared left PP to CP regarding tracheal intubation conditions using the Pentax Airway Scope [32]. The study concluded that left PP is not inferior to CP, offering comparable conditions for tracheal intubation without increased adverse effects.
It was found that i-gel insertion was easier and faster while applying PP than CP along with lesser numbers of reinsertions [33]. Another study found that paralaryngeal pressure was non-inferior to CP in occluding the oesophagus without any deterioration in the intubation parameters in parturients undergoing caesarean delivery [34].
Gautier et al. [23] studied the impact of applying force to the left paratracheal area on air into the gastric antrum during positive-pressure ventilation using a facemask. Their findings revealed that left PP effectively reduced air entry into the stomach, thereby mitigating the risk of gastric insufflation during positive-pressure ventilation.
Our observations hold significant implications for clinical practice and necessitate further exploration through larger, multi-centre trials. In the PP group, typically the pressure is applied above the clavicle with a potential to alter the carotid blood flow in patients with carotid pathology [35]. This fact should always be kept in mind in susceptible patients.
Our study had a few limitations. Although the study was adequately powered based on preliminary data, the sample size may still be insufficient to detect rare adverse effects or subtle differences between the interventions.
The use of a syringe-based method to apply 30 N of pressure lacks real-time objective force measurement. Hence, despite training, there may have been inter-operator variability. Javillier et al. [36] used a dynamometer to measure force precisely and found considerable inter-individual variation in the force required to achieve oesophageal occlusion. This finding suggests that a fixed force of 30 N may not be optimal or sufficient for all patients.
Only ASA I–II patients undergoing elective surgery at a single centre were included in our study, and patients with high risk of aspiration such as the obese, patients with difficult airway and patients scheduled for emergency surgery were not included. Modified Cormack-Lehane assessments were not confirmed by a second observer. This may be seen as potential observer bias. Also, there was a notable sex imbalance between groups (65% male in PP vs. 41% in CP), which may have influenced our results.
Other limitations of this study include potential operator unblinding and use of a single laryngoscope type.
CONCLUSIONS
This randomized, double-blind study provided evidence that PP may be a viable alternative to CP during RSI. The findings suggest that PP offers comparable, if not superior, effectiveness in preventing high PIP without significantly compromising the laryngoscopic view or ease of ventilation. However, further research is needed to confirm these results in larger, more diverse populations and to assess the long-term safety and efficacy of PP. Implementing standardised training and protocols will be crucial in optimizing the application of this technique in clinical practice.