
Assessing pain is central to safe anaesthesia and intensive care, yet it is often most difficult when patients are sedated, intubated, or nonverbal [1, 2]. In the absence of self-report, clinicians rely on observable behaviour and physiological signals, both of which can miss pain or prompt overtreatment [3]. To address this, newer approaches estimate nociception rather than pain per se – ranging from structured behavioural scales to autonomic and brain-signal measures, with emerging options such as computer-vision facial analysis, contact-free sensors, and wearables. These tools can inform decisions, but none is definitive, and all remain vulnerable to confounders (e.g., haemodynamic instability, β-blockade, vasopressors, deep sedation, neuromuscular blockade); interpretation belongs in clinical context and should feed a predefined action-reassessment plan. A pragmatic multimodal strategy includes anchoring assessment in validated behavioural scales when feasible, adding an objective index when not, and reassessing against agreed thresholds, in line with PADIS principles: Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU [4].
This is especially important in paediatric patients. In infants and young children, pain assessment is even more challenging. Their behavioural responses are often non-specific, and their physiological regulation is still developing. Some objective monitors have been adapted for use in children – but the data are more limited, and normal ranges vary by age. In neonates, pain responses may be blunted or unclear, and no single tool has been shown to work well in all situations. This makes a combined approach essential when caring for this group.
The purpose of this review is to summarize the current methods available for objective assessment of acute pain in anaesthesia and intensive care, with a focus on both adult and paediatric populations. We review recent literature, including clinical studies, reviews, and professional guidelines. The article covers four main categories of tools: behavioural scales, vital signs and autonomic system measure, neurophysiology and multimodal indices, and AI-based tools. For each group, we describe how the method works, its clinical uses, limitations, and the quality of supporting evidence.
In this review, pain refers to the conscious and subjective experience that requires awareness and can be communicated by the patient. By contrast, nociception describes the neural activity responsible for detecting and transmitting potentially harmful stimuli. Objective monitoring techniques, whether based on autonomic responses or (neuro) physiological signals, indicate nociceptive or stress-related activity rather than pain itself. Consequently, unless studies involve awake subjects who can report their sensations, the parameters are discussed here should be formally considered as measures of nociception.
To provide an overview of the available research, we summarised the current evidence in a narrative level-of-evidence (LoE) table (Table 1). The grading reflects the amount, design, and consistency of published studies and indicates the relative robustness of data supporting each monitoring modality. This approach follows the general logic of evidence hierarchies but does not rely on a formal system such as OCEBM (Oxford Centre for Evidence-Based Medicine) or GRADE (Grading of Recommendations Assessment, Development and Evaluation).
TABLE 1
Level of evidence (LoE). Narrative appraisal of current evidence
| Method | LoE (OR) | LoE (ICU) | Evidence highlights | Key caveats |
|---|---|---|---|---|
| Behavioural scales (BPS, CPOT) | – | Moderate | Validated against procedures; good inter-rater reliability [1, 2, 6–9] | Mostly single-centre cohorts; limited outcome data despite guideline endorsement [4, 21] |
| Vital signs (HR, BP, RR) | Low | Low | Universally available markers of general stress response [3] | Non-specific for pain; heterogeneous observational evidence [3, 22] |
| Pupillometry/PPI | Moderate | Low | OR/ICU cohorts and RCTs show sensitivity to nociception; useful with deep sedation or NMB [12, 18, 23–27, 29] | Small samples; lighting/eye-access and drug confounding; ICU evidence limited [12, 28, 29] |
| Skin conductance (EDA) | Low | Low | Continuous signal; responsive to noxious stimulation in OR/ICU cohorts [13, 14] | Poor specificity; artefacts from anxiety/fever/sweating; sparse ICU validation [13, 14, 29] |
| HRV/ANI | Moderate | Low | Multiple trials/reviews support intra-op titration value [11, 16, 31–34] | Requires sinus rhythm; sepsis/ventilation/vasoactives confound ICU baselines [11, 35] |
| Surgical Pleth Index (SPI) | Moderate | Low | Predicts early postop pain; meta-analyses and RCTs show intra-op signal [20, 30, 36, 40–45] | No consistent opioid reduction across meta-analyses; PPG quality/positioning effects [15, 17, 36] |
| Nociception Level Index (NOL) | Moderate | Investigational | Intra-op validation and RCTs; meta-analysis shows statistical improvements [46–55] | Clinical benefit uncertain; specialised probe; limited ICU data and early pilots/protocols [35, 52–54] |
| EEG/fNIRS (neurophysiology) | Low | Low | Mechanistic links between cortical signals and pain/nociception [58–61, 76–79] | Small/experimental studies; no standard cut-offs; susceptibility to EMG/artefacts and clinical confounders [60, 62, 67] |
| AI-based behavioural tool | Low | Investigational | Emerging multimodal systems; early feasibility in clinical settings [81–86] | Bias and generalisation risks; privacy/ethics considerations; limited external validation [81, 87–89] |
[i] LoE used in this review (narrative appraisal): high – consistent multicentre RCTs with patient-centred outcomes, moderate – multiple trials/meta-analyses show reliable discrimination, outcome benefits unclear/inconsistent, low – small/heterogeneous studies with inconsistent effects, investigational – early feasibility or very limited data (no established clinical role).
BEHAVIOURAL METHODS OF PAIN ASSESSMENT
Accurate pain assessment in anaesthetised and critically ill patients unable to self-report remains a major challenge. Traditional self-report tools are not very feasible, and physiological indicators may reflect symptoms of sympathetic reaction or critical illness rather than pain [2]. Due to this, behavioural tools based on observable responses (e.g., facial expression, body movements, muscle tension, ventilator compliance) have become essential components of pain management protocols in intensive care units (ICUs) and can also provide useful information about an anaesthetised patient [2].
Among the most extensively validated in adult population tools are the Behavioral Pain Scale (BPS) and the Critical-Care Pain Observation Tool (CPOT). Using these tools helps standardize pain monitoring and has been linked to improved clinical outcomes, including reduced duration of mechanical ventilation and ICU stay [5].
Behavioral Pain Scale
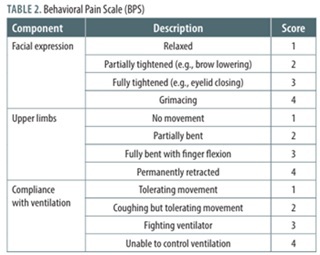
The BPS (Table 2) was first introduced in 2001 by Payen et al. [6] as an instrument for assessing pain in mechanically ventilated patients receiving analgesia and sedation. Since then, the BPS has been validated across multiple ICU settings and studies, and it is now recognized as one of the most widely used tools for pain assessment in critically ill patients [7, 8]. The BPS comprises three key components: facial expression, movement of the upper limbs, and either compliance with mechanical ventilation or vocalization in non-intubated patients. The scale ranges from 3 (no pain) to 12 points (maximum pain), with scores corresponding to pain intensity. A score of ≥ 6 is generally considered indicative of moderate to severe pain, warranting therapeutic intervention. Research demonstrates that the BPS is psychometrically sound and achieves moderate to high agreement between independent observers [2].
TABLE 2
Behavioral Pain Scale (BPS)
[i] Total score range: 3–12. Interpretation: 3 points – no pain, 4–6 points – mild pain, 7–9 points – moderate pain, 10–12 points – severe pain.
Clinical takeaway: Standard for mechanically ventilated ICU patients – threshold ≥ 6 indicates significant pain.
Payen JF, Bru O, Bosson JL, Lagrasta A, Novel E, Deschaux I, et al. Assessing pain in critically ill sedated patients by using a behavioral pain scale. Crit Care Med 2001; 29: 2258-2263 [6].
TABLE 3
The Critical-Care Pain Observation Tool (CPOT)
[i] Total score range: 0–8. Interpretation: 0–2 points – no pain or minimal discomfort, ≥ 3 points – indicates the presence of pain, 6–8 points – suggests severe pain or distress and requires prompt analgesic intervention and reassessment after treatment.
Clinical takeaway: preferred when distinguishing pain from non-pain-related agitation; threshold ≥ 3 indicates pain.
Gélinas C, Fillion L, Puntillo KA, Viens C, Fortier M. Validation of the critical-care pain observation tool in adult patients. Am J Crit Care 2006; 15: 420-427 [1].
Critical-Care Pain Observation Tool
The CPOT (Table 3) was first developed and validated in 2006 by Gélinas et al. [1] as an instrument for assessing pain in critically ill adults. The tool evaluates four behavioural domains: facial expression, body movements, muscle tension, and either compliance with the ventilator or vocalization in non-intubated patients. It has demonstrated strong reliability and validity in differentiating painful from non-painful procedures. Each feature is scored between 0 and 2 points, and the total score ranges from 0 (no pain) to 8 (maximum pain).
Since its introduction, the CPOT has been extensively validated across diverse intensive care settings worldwide, and it is currently recommended as one of the standard behavioural scales for noncommunicative ICU patients [9].
Behavioural pain assessment tools are often compared in clinical settings to evaluate their reliability and diagnostic accuracy in non-communicative ICU patients. Rijkenberg et al. [9] and Thomas et al. [10] compared the BPS and CPOT. Both scales demonstrated good inter-rater reliability and increased scores during a painful procedure (turning), confirming their sensitivity to nociceptive stimuli. These findings suggest that both scales can be applied with confidence in daily ICU practice.
Quality of evidence and limitations
The main limitations of these measures include observer subjectivity, reduced reliability in cases of deep sedation, neuromuscular blockade, or neurological injury, as well as their inability to capture the multidimensional nature of pain. They may also confuse pain with agitation or non-nociceptive responses. For this reason, behavioural scales should be complemented by clinical judgment and physiological indicators.
Although BPS and CPOT are the most validated behavioural tools in those settings, most supporting studies are small, single-centre observational cohorts with moderate risk of bias. Multicentre randomized trials demonstrating improvements in hard outcomes such as mortality or long-term morbidity are lacking. Reliability decreases in deeply sedated, paralyzed, or neurologically impaired patients. Overall, the level of evidence is moderate, and these tools should be interpreted in the context of broader clinical judgment [9, 10].
AUTONOMIC AND PHYSIOLOGICAL METHODS OF ACUTE PAIN ASSESSMENT
Painful stimulation shifts autonomic tone toward sympathetic activation with vagal withdrawal, creating a characteristic pattern in which heart rate (HR) rises and high-frequency heart rate variability (HRV) falls [11, 12]. Peripheral vasoconstriction lowers pulse-oximetry waveform amplitude, pupils dilate, and palmar sweating increases [13–16]. Because these changes are measurable at the bedside, nociceptive stress can be tracked through several autonomic approaches: electrocardiography (ECG)-derived HRV/ANI [12, 17], pulse-oximetry – based SPI [18], electrodermal activity [16], reflex pupil-lometry [13, 19], and multiparametric indices such as NOL [20, 21]. Most tools here read autonomic activity rather than pain, so their drawbacks repeat across methods. Signals are nonspecific and rise with anxiety, fever or general stress, and they shift with drugs that change autonomic tone, including beta blockers, anticholinergics, opioids and vasoactive medication [12, 22]. In the ICU, sepsis and ventilation can depress HRV, deep sedation or neuromuscular block alters reactivity, and practical constraints add noise: light and eye access limit pupillometry, skin moisture and anticholinergics alter electrodermal activity, PPG quality and positioning affect SPI, and NOL needs a dedicated probe and remains investigational [12–15, 18–20].
Physiological parameters – heart rate, blood pressure, respiratory rate
Acute nociception triggers a stereotyped stress response via sympathetic–adrenomedullary and hypothalamic–pituitary–adrenal activation, typically manifesting as tachycardia, hypertension, tachypnoea, pupillary dilatation, sweat gland activity (diaphoresis), and a rise in circulating cortisol. Because HR, blood pressure (BP), and respiratory rate (RR) are continuously monitored in the operating room (OR), ICU, and post-anaesthesia care unit (PACU), clinicians have long used changes in these variables as readily available, though non-specific, signals of pain or distress [3, 23].
HR and BP can be influenced by numerous factors other than pain, such as fever, hypovolaemia, hypoxia, anxiety, medications or emotional/psychological stimuli. Studies in emergency department patients have shown no clear linear correlation between self-reported pain scores and HR [13], and BP fluctuations can similarly occur for reasons unrelated to nociception. Respiratory rate may increase with pain but is also affected by sedation, ventilator settings, or metabolic factors. Consequently, relying on a single vital sign to assess pain often leads to false positives or negatives.
In ICU patients, interventions such as beta-blockers, neuromuscular blocking agents, or deep sedation can blunt or mask typical physiological responses to pain. As a result, normal vital signs do not rule out pain, and abnormal signs do not always indicate it. Clinical guidelines stress that vital signs alone are insufficient for pain assessment but can serve as cues for further evaluation [14]. While universally available, vital signs lack specificity for pain monitoring and are now considered adjunctive indicators – helpful for identifying general stress responses but too confounded by other factors to guide analgesia reliably on their own.
Quality of evidence and limitations
The evidence supporting vital signs as pain indicators is weak. Most studies are observational with heterogeneous methods, and common confounders (fever, anxiety, hypovolaemia, hypoxia and vaso-active agents) undermine reliability. Consequently, the overall certainty of evidence is low; used in isolation, vital signs show poor discriminant validity for pain and should serve only as cues to trigger assessment with validated instruments [3, 24].
Pupillometry (pupillary dilation reflex)
The pupillary dilation reflex is an autonomic response directly linked to nociceptive stimulation, where noxious stimuli increase sympathetic activity and inhibit parasympathetic tone, causing pupil dilation – even in unconscious patients. Infrared pupillometry quantifies this reflex by measuring pupil size and its response to a controlled stimulus. Unlike behavioural pain scores, this reflex remains intact under neuromuscular blockade, making it particularly valuable for deeply sedated or paralyzed patients. Pupillometry allows for monitoring of an autonomic reflex closely coupled to nociception, offering greater specificity than global vital signs [25].
Modern portable pupillometers deliver precise, objective measurements and, when paired with a controlled noxious stimulus (e.g., tetanic electrical stimulation), allow clinicians to estimate analgesia levels using the Pupillary Pain Index (PPI). The PPI, scored from 1 to 9 (or 0 to 10), reflects the pupil-lary dilation response: low scores indicate adequate analgesia, while high scores suggest insufficient analgesia [26] and have been shown to correlate with nociception and predict reactivity in children [27]. In the OR, pupillometry helps anaesthesiologists titrate opioids by detecting inadequate analgesic depth during surgical stimuli, reducing opioid consumption and preventing unwanted pain responses [28]. In ICU settings, pupillometry is useful for assessing pain in sedated or unconscious patients, with studies showing correlations between pupil-lary dilation and behavioural pain scores during routine procedures [19]. It can also predict inadequate analgesia during interventions such as endotracheal suctioning, allowing proactive adjustments to analgesic infusions [29].
Despite its advantages, pupillometry has limitations. It is episodic rather than continuous, and requires shielding from ambient light as well as unobstructed eye access, which may be impractical with ocular or cranio-facial pathology (e.g., injury, oedema, cataract). Pupillometry is highly sensitive to nociception but drug effects can confound it and performance varies between patients and procedures, so findings should be interpreted in the clinical context. It is most effective in intraoperative settings and for ICU patients under deep sedation or neuromuscular blockade, where conventional pain scales are not applicable.
Quality of evidence and limitations
Pupillometry has been evaluated in several small randomized trials and observational studies, mostly in OR or ICU settings. While results are promising, evidence remains limited to single-centre cohorts, often with < 100 participants, and susceptible to drug and lighting confounders. No large multicentre randomized controlled trials (RCTs) have confirmed its routine clinical value. The current evidence level is low-to-moderate [13].
Skin conductance (electrodermal activity responses)
As noted above, sympathetic activation increases sweat eccrine gland activity; skin-conductance monitors leverage this by measuring cutaneous electrical conductance, which rises with sweat secretion. Often termed galvanic skin response or electrodermal activity (EDA) monitoring, this technique involves placing electrodes on the palmar surfaces of the hand or sole of the foot to detect minute fluctuations in skin conductance and thus perspiration. Skin conductance rises within seconds of a noxious stimulus and is most reliable for tracking changes within the same patient; baseline values vary widely, so between-patient comparisons are less meaningful [14]. Skin conductance reflects eccrine activation via sympathetic cholinergic fibres – as opposed to adrenergic fibres, which regulate, inter alia, HR and contractility, vascular tone, and pupillary dilatation. This response occurs rapidly and is independent of haemodynamic changes. Research by Storm et al. [14] indicated that the skin conductance algesimeter responds to noxious stimuli with a high sensitivity (around 90%) and can detect nociception-related autonomic reactions better than HR or blood pressure. During general anaesthesia, increases in skin conductance correlate with surgical stress and are attenuated by analgesics. Because sweat gland activity is not affected by neuro-muscular blockade or most anaesthetic agents, this technique can work even in fully paralyzed patients [30]. It also provides continuous, real-time output – potentially allowing clinicians to see a ‘spike’ on a monitor shortly after a patient experiences a nociceptive event.
Skin conductance monitoring has been explored in various clinical contexts. For example, Günther et al. [15] monitored ICU patients with the Med-Storm device and observed that skin conductance fluctuations increased during routine nursing procedures and apparent discomfort. However, they also found significant limitations in specificity: patients who were agitated or anxious (even if not in pain) also showed elevated conductance activity, and deeply sedated patients had generally low conductance regardless of moderate pain. The overlap between pain-induced and agitation-induced signals was considerable. This study concluded that while skin conductance might reflect a general ‘stress’ level, it was unsuitable for detecting pain alone in the ICU context because of confounding factors [22].
Electrodermal activity reflects sympathetic arousal rather than pain. Additionally, agitation and fever can produce false positives. Analogically, changes in sedation levels or emergence from anaesthesia can also trigger responses unrelated to pain. States that impair eccrine function (such as skin dryness, peripheral neuropathy, influence of anticholinergic drugs) may yield spuriously low readings [15, 22]. While the monitor provides continuous data, it can be difficult to interpret, as clinicians must separate meaningful increases from random fluctuations or background noise. There is no clear standard for how many fluctuations indicate pain, so the results must always be considered in context. These challenges have limited the use of skin conductance monitoring for pain assessment in adult critical care.
Quality of evidence and limitations
Most studies on electrodermal activity are pilot or feasibility projects with small sample sizes. Although sensitivity to nociceptive stimuli is high, specificity is poor, with frequent false positives related to agitation, stress, or fever. No randomized trials or large multicentre validations are available. The overall quality of evidence is low, and clinical applicability in adult ICU remains very limited.
Heart rate variability and Analgesia Nociception Index
HRV refers to the natural beat-to-beat fluctuations in HR caused by dynamic autonomic nervous system balance. In a healthy resting state, the vagus nerve influences variability of the HR, particularly linked to the respiratory cycle. Acute pain or nociceptive stress tends to decrease parasympathetic (vagal) activity and increase sympathetic activity, which leads to a reduction in high-frequency HRV and a relative increase in low-frequency components. Based on this physiology, monitoring HRV can provide insight into the patient’s nociception level-diminished HRV (specifically, reduced high-frequency variability) is associated with pain and stress, whereas higher HRV indicates a more relaxed, comfortable state [12, 31].
The Analgesia Nociception Index (ANI) is a metric derived from HRV analysis. ANI monitors use the ECG signal to calculate the proportion of high-frequency variability in the last 56–176-second window (depending on used index and version of the device), internally normalized within the analysis window, and scale it into an index from 0 to 100 that is continuously updated. An ANI of 100 would correspond to maximal parasympathetic tone (suggesting no nociceptive stress), whereas an ANI of 0 would mean no high-frequency variability (indicating extreme nociception or pain stress). In practice, during balanced general anaesthesia, ANI values typically range between ~50 and 70; drops below a certain threshold (e.g. ANI < 50) might signal inadequate analgesia, prompting intervention. It is important to remember that the reliability of HRV-based monitors depends on a normal sinus heart rhythm and relatively stable physiology. Cardiac arrhythmias such as atrial fibrillation, frequent ectopic beats, or paced rhythms invalidate the ANI calculation, because the algorithm assumes variability is due to autonomic modulation, not random rhythm disturbance.
ANI has been extensively studied in the OR setting. Data show that a declining ANI often precedes or accompanies signs of autonomic response to a surgical stimulus and can lead to lower opioid consumption [32]. Additionally, a recent trial of auto mated (closed-loop, ANI-guided) remifentanil delivery during burn surgery showed promising results (lower intraoperative remifentanil use and improved haemodynamic stability) without sacrificing post operative analgesia [33]. Systematic reviews and meta-analyses indicate that ANI is moderately effective in reflecting intraoperative nociception, although results have been mixed [34]. A meta-analysis assessing periprocedural applicability of the ANI analogue for neonates (NIPE, Newborn Infant Para-sympathetic Evaluation) revealed heterogeneous outcomes and study designs, indicating that further studies are required to confirm its efficacy [35].
HRV-based nociception monitoring in awake or lightly sedated ICU patients is less validated. Critical illness or inflammation can by itself reduce HRV (often seen in sepsis or MODS), so critically ill patients might have low ANI values at baseline not strictly related to pain [36].
Currently, evidence suggests that while ANI and similar indices can improve the titration of opioids in the OR, it should be treated as a tool to refine clinical judgment. In the ICU, HRV-based monitoring remains mostly investigational, except perhaps in specific scenarios such as during procedural sedation.
Quality of evidence and limitations
Several RCTs and meta-analyses have assessed ANI in perioperative settings, but the results are inconsistent – some show reduced intraoperative opioid use, while others fail to demonstrate differences in postoperative pain outcomes. ICU studies are mostly pilot cohorts with major confounding from sepsis, arrhythmias, and vasoactive drugs. Overall, the evidence behind ANI remains moderate in anaesthesia and low in intensive care [34].
Surgical Pleth Index
The Surgical Pleth Index (SPI) is an objective index derived from the pulse oximetry curve – photoplethysmogram – that quantifies the balance between nociception and analgesia during general anaesthesia. The SPI is calculated from two key components of the pulse wave: the heartbeat interval (HBI, reflecting the interpulse interval) and the pulse photoplethysmography amplitude (PPGA). SPI is computed as 100 minus a weighted combination of HBI and PPGA, with greater weight given to changes in PPGA. Nociceptive stimulation triggers sympathetic nervous system responses – namely, tachycardia (shortened HBI) and peripheral vasoconstriction (reduced PPGA) – which cause the SPI value to rise. Thus, higher SPI values correspond to an increased sympathetic response to pain, whereas lower values reflect adequate analgesia or deep anaesthesia. Monitoring SPI requires only a standard pulse oximeter sensor, making it non-invasive and easily integrated into routine intraoperative monitoring. The numeric SPI (0–100) allows intuitive interpretation: in adults under general anaesthesia, 20–50 is typically optimal; persistent values above this range may signal an inadequate opioid effect, and values below it may indicate excessive autonomic suppression.
Pooled RCTs/meta-analyses show no overall reduction in intraoperative opioid use with SPI guidance. They do show modest benefits (fewer tachycardia events, lower propofol use, faster eye opening), but effects on extubation time, postoperative pain scores, postoperative nausea and vomiting, and postoperative opioid use remain mixed [16, 18]. Additionally, SPI values measured before emergence have been linked with early postoperative pain levels and analgesic needs, suggesting a predictive role [31].
SPI reads sympathetic activation and is not pain specific. Interpretation should account for photoplethysmography signal quality and patient positioning [37].
Apart from SPI, the plethysmographic perfusion index (PI) (also known as the peripheral perfusion index – PPI) has been examined as a marker of nociceptive response. Recent work illustrates ongoing but uneven interest in this approach, e.g. a recent intraoperative study showed PI to fall with surgical stimulation and rise after opioid administration [38]. Smaller postoperative cohorts, including an earlier study by Chu et al. [39], reported PI increases after pain relief and modest correlations with anal-gesic requirement [40]. These examples reflect continued interest in PI as a nociception marker, but current evidence is inconsistent and lacks formal validation.
Quality of evidence and limitations
Evidence for SPI-guided analgesia comes primarily from small randomized trials; findings on opioid use are mixed [41–45], and pooled analyses show no overall reduction [16]. Effects on haemodynamic/sympathetic stability are modest [16] and inconsistent across studies [42, 43, 46]. Outcomes are largely surrogate, with clinically relevant endpoints such as delirium, length of stay, or mortality being rarely addressed. Heterogeneity in anaesthetic techniques, comparators, and SPI targets further limits synthesis [16, 18]. Almost no data exist for ICU populations. The current evidence is moderate in surgical settings and low in critical care.
Nociception Level Index
The Nociception Level (NOL) Index is a technology that supports personalized analgesic management using a numeric, non-linear scale from 0 (no nociception) to 100 (extreme nociception), with values above 25 indicating insufficient analgesia [47, 48]. It employs a special finger-probe sensor platform to continuously collect and analyse physiological signals through advanced algorithms. The system integrates data from four sensors – photoplethysmography, galvanic skin response, peripheral temperature, and accelerometry – to capture the sympathetic response to noxious stimuli [20]. From these inputs, the NOL algorithm extracts and evaluates parameters such as pulse rate, pulse-rate variability, pulse-wave amplitude, skin conductance level, peripheral temperature, and movement. This multiparametric approach improves the detection and quantification of nociceptive responses [21, 49].
Clinical evidence highlights the benefits of using the NOL Index to guide analgesic management during surgery. In a prospective RCT, NOL-guided opioid titration during major abdominal surgery under sevoflurane/fentanyl anaesthesia led to significantly improved postoperative pain scores compared to standard care [49]. Similarly, a double-centre RCT found that patients undergoing elective abdominal surgery reported less postoperative pain when opioid dosing was adjusted based on the NOL Index [50]. Beyond pain control, studies have linked NOL monitoring to enhanced haemodynamic stability during major abdominal and gynaecological laparoscopic procedures, further demonstrating its clinical utility [51, 52]. Notably, a trial regarding abdominal procedures revealed that NOL-guided analgesia reduced remifentanil consumption by approximately 30%, underscoring its potential to optimize opioid use while maintaining effective pain management [52].
While NOL monitoring shows promise in critically ill patients, its application in the ICU remains under investigation. Studies suggest that NOL can differentiate between nociceptive and non-nociceptive stimuli [53], making it a potentially valuable tool for pain assessment in ICU patients. This includes those receiving continuous neuromuscular blockade with deep sedation as well as patients managed with light-to-moderate sedation without neuromuscular blocking agents [36].
The NOL Index has been compared to commonly used pain-assessment tools, including HR, systolic blood pressure (SBP), ANI, and the Bispectral Index (BIS) [48]. Studies consistently show that all these indicators deviate significantly from baseline during nociceptive stimulation. The NOL Index outperforms the other parameters, underscoring its superior sensitivity and potential clinical utility [36, 47, 48].
In summary, the NOL Index represents a significant advancement in nociception monitoring, providing a multiparametric and objective method to guide analgesic management. Its potential to improve intraoperative and critical care pain assessment, reduce opioid consumption, and enhance patient outcomes makes it a valuable tool for modern anaesthetic practice. The main limitation of this method is that can be influenced by similar factors as other autonomic-based indices.
Quality of evidence and limitations
Clinical studies of the NOL Index include several randomized trials [e.g., 36, 39, 40, 42, 54], but most are single-centre, and some are industry-sponsored, introducing potential bias. Sample sizes are modest, and ICU applications remain investigational, with a major trial underway (NCT05339737) [55]. Although the 2023 meta-analysis by Bornemann-Cimenti et al. [56] found statistically significant reductions in postoperative opioid use and pain intensity with NOL-guided anaesthesia, it showed no clinically meaningful benefits; therefore, current evidence does not support routine NOL use. More independent multicentre studies are needed before the tool can be considered for routine practice. Current evidence is preliminary and low-to-moderate in quality.
NEUROPHYSIOLOGICAL AND AI-BASED TECHNIQUES
Electroencephalography
A few years after discovering the human electroencephalogram in 1929 and describing sensory ‘alpha blocking’ (i.e., the suppression of resting occipital rhythms by sensory input or attention), Hans Berger demonstrated (in 1935) that a brief painful stimulus (a needle prick) could disturb ongoing rhythmic activity. This early observation hinted that brain signals might provide objective readouts of pain [57, 58]. Systematic electroencephalography (EEG) research focused on pain and nociception accelerated much later, from the 1980s on, eventually linking quantitative oscillations to perceived intensity in paradigms of sustained (e.g., tonic heat, alpha-pain relations), as well as phasic stimulation [59]. Broadly, reductions in sensorimotor alpha (8–12 Hz) and beta (12–30 Hz) frequencies correlate with noxious stimuli, whereas increases in prefrontal/ salience-network gamma (> 30 Hz) correlate with reported pain intensity during tonic stimulation [60–62]. For brief, phasic noxious stimuli, transient increases in low-frequency power (delta 1–4 Hz, theta 4–8 Hz), together with gamma event-related synchronization, superimposed on sensorimotor alpha desynchronization, are characteristic [59]. Early machine-learning approaches can detect such signatures in real time, but performance is not consistent across patients, states, and drugs [63, 64].
In EEG, two recording approaches matter clinically. Scalp EEG is non-invasive and easy to deploy but blends sources and offers limited anatomical specificity. Intracranial EEG has shown nociception-related activity in operculo-insular and cingulate regions, but these findings come from epilepsy-mapping and experimental settings and are not currently applied to pain monitoring [65].
EEG patterns are heavily influenced by drugs, sedation depth, movement, and noise; current metrics still lack evidence for routine clinical use. Still, the experimental patterns above offer anchors: alpha/beta reductions index nociceptive drive, while frontal gamma relates more to perceived intensity. Under general anaesthesia, cortical responses to noxious stimuli are state- and drug-dependent, which precludes their universal use as markers in this context [61, 63].
At the same time, EEG-derived or EEG–electro-myography (EMG) monitors have been tested in clinical practice: qCON/qNOX (CONOX) provides hypnosis and a probabilistic response-to-noxious-stimulus index [66]; the GE Entropy module’s RE-SE gap reflects facial EMG reactivity and can widen with nociception [67]; BIS is a primarily hypnosis index, but EMG-related BIS surges during noxious stimulation (or neuromuscular-block reversal) are well described [68]; and the fully EEG-based Pain Threshold Index (PTI) has shown early promise, including a randomized trial of PTI-guided analgesia [69]. These tools are available and potentially useful/helpful, but the body of evidence is still too small for recommendation of their routine use.
Complementing the oscillation-based EEG markers outlined above, nociceptive evoked potentials (EPs) are time-locked cortical responses to noxious stimuli that provide an objective probe of small-fibre/spinothalamic function, complementing examination, sensory testing and imaging. In practice, several modalities are available [62], among which laser-evoked potentials (LEPs) are the best established for clinical neurophysiology, with the broadest evidence base and sensitivity to spinothalamic lesions. Crucially, because EPs need timed stimuli and averaging, they cannot track ongoing nociception at the bedside; they are mainly used in controlled pain/analgesia studies, not real-time analgesia titration. As of now, EEG metrics lack evidence to inform routine analgesia titration in practice, but recent trials are addressing exactly this: for example, validation of EEG-guided analgesia in older adults undergoing CABG surgery (recently completed, NCT05279898), a PICU validation of processed EEG (SedLine PSI) for analgosedation in mechanically ventilated children (NCT05969483). Collectively, the next steps are standardized pipelines, robust normative data, and multicentre outcome trials linking EEG-guided decisions to pain, opioid use, and recovery.
Functional near-infrared spectroscopy
Functional near-infrared spectroscopy (fNIRS) is a non-invasive optical method that measures cortical activity through changes in oxy- and deoxyhaemoglobin. Its portability makes it especially useful in settings where conventional neuroimaging is impractical, such as neonatology and anaesthesia.
fNIRS was central to proving that infants both feel and process pain – Slater et al. [70] showed that heel lance evokes oxygenated haemoglobin increases in the contralateral somatosensory cortex of newborns. These findings, later corroborated with EEG [71] and functional magnetic resonance imaging (fMRI) [72] studies, contributed to overturning the outdated belief that neonatal brains were too immature for nociception. A 2011 review emphasized that cortical responses can be measured even when behavioural cues are absent, making fNIRS particularly valuable in fragile infants [73]. More recent work has used fNIRS to test interventions such as sucrose or skin-to-skin care, with mixed effects on cortical activity [74] and to assess pain associated with circumcision [75].
In adults, fNIRS detects reproducible cortical changes during experimental thermal and mechanical pain [76]. Clinically, nociceptive activity has been observed during colonoscopy [77] and during surgical incision under general anaesthesia [78]. Importantly, cortical responses persist under anaesthesia (although typically attenuated), raising the prospect of fNIRS as a monitor of intraoperative nociception [79].
Catheter ablation under anaesthesia was shown to evoke cortical deactivations measurable with fNIRS. A randomized trial further demonstrated that remifentanil attenuated these responses compared with placebo [79, 80], highlighting its potential for guiding intraoperative analgesia.
Although not yet standard practice, several promising uses are emerging. In neonatology, fNIRS may complement behavioural scores to provide objective pain assessment and evaluate analgesic strategies. In perioperative care, forehead probes could be incorporated into multimodal anaesthesia monitoring to detect inadequate analgesia before motor or autonomic changes occur. Beyond the OR, fNIRS may also support assessment in non-communicative adults, such as patients with cognitive impairment or disorders of consciousness.
Recent advances in signal processing and artefact correction are improving the reliability of fNIRS and moving it toward clinical application. Functional- connectivity studies indicate utility for monitoring responses to non-pharmacological analgesia, including virtual-reality interventions for cancer pain [81]. In parallel, clinical evaluation is progressing with several trials underway; the role of fNIRS in analgesic targeting and routine bedside monitoring remains to be defined.
Quality of evidence and limitations
EEG and fNIRS provide valuable mechanistic insights, but clinical validation is scarce. Most studies are experimental, involve small samples, and lack standardized protocols or reproducible cut-offs. Signals are highly susceptible to confounders (sedatives, muscle activity, artefacts), limiting generalizability. At present, evidence quality is low, and these techniques remain research tools rather than established clinical monitors.
AI-based tools
From dementia wards to PACUs and ICUs, AI algorithms that read behaviour (through analysis of faces, voice, and/or motion) are emerging as potentially reliable tools for pain detection. Broadly, approaches fall into three groups: facial-video systems, audio-based classifiers using vocalizations/prosody, and multimodal pipelines that fuse face/audio with simple physiology [82]. Facial-analysis apps such as PainChek show good reliability in hospital patients with dementia but are aids, not replacements, for clinical judgment [83]. Beyond dementia care, peri-operative facial-video models can triage clinically significant pain with high accuracy [84]. ICU-focused systems are also emerging: a prospective adult-ICU study demonstrated feasible automated facial- video classification of pain, and a pilot calibration trial (NEVVA) during sedation weaning reported AUC ≈ 0.79 with reasonable sensitivity/specificity [85]. Multimodal pipelines that fuse facial video with simple physiology (e.g., heart-rate time series) improve binary detection efficiency, and continuous- monitoring approaches combining face/audio with ECG/EMG/EDA further strengthen performance [86]. In practice, performance is limited by occlusion (tubes, masks), variable lighting, oedema, and sedation. Within this field, a wide range of tools employing distinct methodological approaches has been proposed, a comprehensive synthesis of which was provided by Werner et al. [82]. Ethical (and practical) issues include known demographic biases in common monitors, e.g., pulse oximetry [87], and more broadly, dataset bias [88], the need for explicit consent and strong privacy safeguards for continuous audio/video capture [89], and avoiding over-reliance on surrogate indicators when patient self-report – the clinical reference standard – is available [90].
TABLE 4
The Face, Legs, Activity, Cry and Consolability (FLACC) Scale
[i] Total score range: 0–10. Interpretation: 0 point – relaxed and comfortable, 1–3 points – mild discomfort, 4–6 points – moderate pain, 7–10 points – severe discomfort or pain.
Clinical takeaway: First-line for young children as non-communicative patients.
Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr Nurs 1997; 23: 293-297 [96].
Quality of evidence and limitations
Overall evidence quality is low to moderate, driven by single-centre studies, small datasets, surrogate labels, retrospective analyses, and limited external validation. Generalisability remains uncertain due to demographic imbalance, occlusion/ lighting artefacts, device variability, sedation effects, and a paucity of prospective trials linking outputs to anal gesic decisions or patient outcomes.
ACUTE PAIN ASSESSMENT IN THE PAEDIATRIC POPULATION
Pain in hospitalized children is often underrecognized despite its common occurrence, particularly during diagnostic and therapeutic procedures. Accurate pain intensity assessment is crucial for effective treatment and outcomes, as it allows for personalized interventions that improve quality of life [91]. While over 40 validated scales exist for assessing acute pain in young children, alongside multidimensional tools for older children, their clinical use remains inconsistent, undermining their potential to enhance patient care.
Premature infants and newborns pose unique challenges, as their inability to communicate verbally necessitates careful observation of behavioural cues such as muscle tension, grimacing, and positional changes. Nociceptive pathways are active from birth [70–72], but descending inhibitory mechanisms remain immature, which may enhance responsiveness to noxious stimuli [92, 93]. Repeated painful exposures, even from routine care, can lead to lasting stress, impacting development and potentially causing emotional, behavioural, and cognitive impairments [93]. The therapeutic team must therefore prioritize minimizing pain and stress during medical care to mitigate these risks.
Additionally, patients with intellectual disabilities present further complexities, as their behavioural changes can obscure typical pain indicators, complicated by conditions such as seizures or neurological disorders [94, 95]. These challenges highlight the need for specialized training and tailored approaches to ensure effective pain management in vulnerable populations.
Behavioural scales
The Face, Legs, Activity, Cry, and Consolability (FLACC) Scale (Table 4) and the COMFORT-Behavioral Scale (Table 5) are two widely used behavioural tools for assessing pain, distress, and sedation in paediatric patients. The FLACC scale, introduced in 1997, is designed to evaluate postoperative, procedural, and acute pain in children, particularly young children and those with intellectual disabilities [96]. It assesses five parameters – facial expression, leg position, activity, crying, and consolability – each scored on a 0–2 scale, resulting in a total score of 0–10, where 0 indicates no pain and 10 requires immediate intervention [96].
TABLE 5
COMFORT-Behavioral (COMFORT-B) Scale
[i] Total score range: 6–30. Interpretation: 6–10 – over-sedation, 11–23 – moderately sedated patient, 24–30 – pain or distress (requires intervention).
Clinical takeaway: standard in PICU for ventilated and sedated children.
Ista E, van Dijk M, Tibboel D, de Hoog M. Assessment of sedation levels in pediatric intensive care patients can be improved by using the COMFORT ‘behavior’ scale. Pediatr Crit Care Med 2005; 6: 58-63.
The COMFORT-Behavioral Scale, originally developed for mechanically ventilated children, has been validated for use in both ventilated and non-ventilated paediatric intensive care unit (PICU) patients [97]. It evaluates six factors: alertness, calmness/agitation, respiratory response (or crying), physical movement, muscle tone, and facial tension; each is scored from 1 to 5, yielding a total score of 6–30. Scores indicate oversedation (6–10), moderate sedation (11–23), or minimal/no sedation (24–30) [97]. While both scales are observational tools for paediatric care, the FLACC scale is specific to pain assessment, whereas the COMFORT-B scale focuses on sedation and distress. Both share the goal of providing standardized methods for monitoring and improving patient comfort.
TABLE 6
Comparison of the tools
Physiological and neuromonitoring techniques in paediatric pain assessment
In recent years, physiological and autonomic methods such as the HRV-derived NIPE index [35], pupillometry[27], and skin conductance measurement [98], have been increasingly used to assess pain in paediatric populations, especially when verbal communication is limited. These techniques, as mentioned earlier, focus on physiological responses to pain, with the NIPE index being validated for use in neonates, particularly in the NICU, to detect insufficient pain relief in anaesthetized infants and critically ill children [99, 100].
However, pain assessment in neonates remains challenging due to the immaturity of the central nervous system and nonspecific behavioural responses. While behavioural and physiological scales are helpful, they do not directly measure neocortical nociception, which is critical for pain encoding and central pain pathway development. Brain-oriented techniques such as fNIRS [73, 75], EEG [71], and fMRI [72] have been employed to assess neonatal pain at the cortical level, with evidence suggesting that both sensory and emotional pain components are active in neonates.
Despite advancements, no single gold standard exists for pain assessment in infants and young children. Each method has limitations: behavioural scales may be influenced by non-pain factors, physiological measures such as HRV or skin conductance lack specificity, and brain-oriented techniques are resource-intensive and impractical for routine use. Additionally, pain assessment differs from adults due to developmental variations in pain perception and expression. For instance, neonates’ underdeveloped pain inhibitory systems heighten sensitivity to noxious stimuli, necessitating tailored approaches.
Given these challenges, a multimodal strategy combining behavioural, physiological, and brain-oriented techniques is essential to capture pain’s multidimensional nature in paediatric populations. While no single tool encompasses the full extent of the phenomenon of pain and nociception, integrating multiple methods provides a more comprehensive understanding, enhancing management strategies and improving care for even the youngest patients.
Quality of evidence and limitations
Pain assessment in children employs diverse methods tailored to their needs, each offering distinct advantages and challenges. Behavioural scales, while practical, can be influenced by non-pain factors. Physiological measures provide objective data but may lack specificity. Brain-oriented techniques offer direct cortical insights but are impractical for routine use. A multimodal approach enhances understanding, and developmental considerations are crucial for accurate assessment.
CONCLUSIONS
Assessing pain in patients who cannot self-report, across adult and paediatric intensive care, remains difficult. Behavioural scales (BPS, CPOT, FLACC, COMFORT-B) are the most recommended and validated options; they are simple and reproducible but observer-dependent, less reliable with deep sedation or neurological impairment, and do not capture pain’s multidimensionality. The main characteristics of each method are listed in Table 6, with children-specific caveats in Table 7.
Autonomic and physiological indices (pupillometry, HRV-derived ANI/NIPE, SPI, skin conductance) provide supplementary information when behavioural cues are sparse, including under deep sedation or neuromuscular blockade. Evidence for these tools is stronger in peri-operative settings than in the ICU, where validation is limited and findings are mixed; specificity is further constrained by drug effects, haemodynamic instability, and non-pain stressors.
TABLE 7
Objective pain monitoring methods in paediatrics – main applications and limitations
Neurophysiological approaches (EEG, nociceptive evoked potentials, fNIRS) provide insight into central processing but largely remain in the research domain and require further clinical validation. AI-enabled behavioural monitoring is emerging, although performance is affected by occlusion, lighting, sedation, device variability, and scarce external validation.
No single tool replaces clinical judgement. A multimodal strategy – integrating behavioural assessment, physiological indicators, neurophysiology where available, and selected AI-based adjuncts – offers the best prospect for individualised analgesia while minimising under- and overtreatment.
FUTURE DIRECTIONS
The evidence base remains dominated by small, single-centre studies with heterogeneous methods; adequately powered multicentre trials should evaluate effects on patient-centred outcomes (e.g., opioid exposure, delirium, ICU length of stay). Standardised protocols and thresholds would improve reproducibility, and clinically embedded multimodal pipelines merit testing. Paediatric and neonatal populations are under-studied and require rigorous validation and cost-effectiveness analyses for wider implementation.