

Second-generation supraglottic airway devices (SGAs) have revolutionized pediatric anesthesia by providing significant advancements in airway management, particularly during short-duration procedures [1]. Unlike their first-generation counterparts, these devices offer enhanced sealing capabilities and integrated gastric drainage channels, which substantially reduce the risks of aspiration, inadequate ventilation, and other complications that can arise during general anesthesia [2, 3]. Their efficiency, ease of use, and safety profile make them indispensable tools in modern pediatric practice.
Among the second-generation SGAs, the laryngeal tube suction disposable (LTS-D, VBM Medizintechnik, Sulz, Germany) and i-gel (Intersurgical Ltd, Wokingham, Berkshire, UK) have been widely adopted due to their innovative designs and specific advantages. The LTS-D is equipped with inflatable cuffs, which provide enhanced adaptability to the pharynx [4], ensuring better sealing and stability in various clinical scenarios. In contrast, the i-gel, composed of a thermoplastic elastomer, offers a naturally conforming seal without the need for cuff inflation, simplifying insertion and potentially reducing complications related to intracuff pressure [5]. Both devices have been lauded for their effectiveness and practicality, particularly in the context of pediatric airway management [1], where anatomical and physiological challenges demand high-performance solutions [6].
Despite the growing popularity of these devices [7], limited comparative evidence exists regarding their performance in pediatric patients, particularly in non-paralyzed pediatric patients during general anesthesia [8]. The unique anatomical and physiological considerations in children, such as smaller airways and higher metabolic demands, further emphasize the need for a rigorous evaluation of these devices. Moreover, while the i-gel has been extensively studied for its rapid insertion and superior anatomical positioning, the recently updated version of the LTS-D, which features enhanced curvature and increased adaptability, has not been adequately assessed in clinical practice. This lack of evidence represents a critical gap, as the choice of airway device directly influences not only oxygenation and ventilation but also procedural efficiency, patient safety, and postoperative recovery.
This study addresses this gap by systematically comparing the clinical performance of the LTS-D and i-gel in anesthetized non-paralyzed pediatric patients undergoing elective surgical procedures. We hypothesize that, although both devices are effective in maintaining adequate oxygenation and ventilation during spontaneous breathing under general anesthesia, their design differences will result in clinically meaningful variations. The primary aim of this study was to compare the efficacy of the LTS-D and i-gel in maintaining optimal oxygenation and ventilation in non-paralyzed pediatric patients under general anesthesia. Secondary aims included evaluating differences in device insertion time, rate of gastric tube insertion, oropharyngeal leak pressure, fiberoptic visualization of the vocal cords, tidal volumes (Vt), anesthesiologist satisfaction, and adverse events.
FIGURE 1
Structural comparison of the laryngeal tube suction disposable (LTS-D) (A) and the i-gel (B). The illustration highlights key differences in design, material composition, and functional features, including the integrated sealing mechanisms and access to the gastrointestinal tract, which are crucial for their respective performance in airway management

METHODS
Study design
This study was designed as a prospective, randomized controlled trial to compare the clinical performance of the LTS-D and i-gel in pediatric patients undergoing elective surgery under general anesthesia without neuromuscular paralysis. The trial adhered strictly to the Consolidated Standards of Reporting Trials (CONSORT) guidelines. Ethical approval was obtained from the Ethics Committee of Bnai Zion Medical Center (Approval No. 0117-22-BNZ), and the trial was registered at ClinicalTrials (NCT05503277). Written informed consent was secured from the legal guardians of all participants prior to enrollment.
Participants
Eligible participants included pediatric patients aged 2 to 8 years, weighing 12–25 kg, classified as ASA physical status I, and scheduled for elective short-duration surgery under general anesthesia with spontaneous ventilation. Surgical procedures included inguinal hernia repair, circumcision, and umbilical hernia correction. Exclusion criteria included ASA physical status II or higher, upper respiratory tract symptoms within 10 days of surgery, congenital airway abnormalities, and any history suggesting a difficult airway or contraindications to general anesthesia, or supraglottic airway device use.
All participants underwent a detailed preoperative assessment, including a review of medical history and physical examination, to confirm eligibility.
Device characteristics
This study examined two second-generation SGAs for pediatric patients: LTS-D and the i-gel, both in size #2, selected based on manufacturers’ weight recommendations. These SGAs aim to enhance airway management by providing superior sealing capabilities and integrated gastrointestinal access. Despite similar purposes, the devices differ substantially in design, material, and operational features. Figure 1 highlights these structural and functional differences.
Laryngeal tube suction disposable
The LTS-D is a cuffed SGA constructed from medical-grade polyvinyl chloride (PVC) [4]. Its key features include two inflatable cuffs – a proximal oropharyngeal cuff and a distal esophageal cuff – with a ventilation channel positioned between them to ensure optimal airway patency and minimize leakage. Key design updates include (manufacturer communication): (1) curvature redesign: modified from 45° to 60°, improving anatomical adaptability; (2) enhanced material: softer PVC increases pharyngeal compliance; (3) hypopharyngeal space: redesigned ventilation section expands the hypopharyngeal space by 25%, reducing insertion resistance and pressure. The device integrates a gastric drain tube to aspirate stomach contents, lowering regurgitation risk, and supports tracheal intubation through its ventilation channel. Inflation of the cuffs requires a color-coded syringe (35 mL for size #2), with intracuff pressures monitored to remain at or below 60 cmH2O to maintain effective sealing while minimizing tissue compression.
i-gel
The i-gel is a cuffless intubating supraglottic airway device made from medical-grade thermoplastic elastomer, designed to naturally conform to the patient’s anatomy, eliminating the need for inflatable cuffs [5]. This simplifies use, reduces insertion time, and minimizes insertion-related complications. Its anatomically shaped airway seal aligns with the laryngeal inlet and hypopharyngeal tissues, ensuring a reliable seal. An integrated gastric channel facilitates gastric tube placement for evacuating stomach contents. The i-gel is lightweight, disposable, cost-effective, and suitable for diverse clinical settings.
Randomization and blinding
Patients were randomized to two groups (LTS-D or i-gel) using a computer-generated randomization sequence produced with the blockrand package in R (version 4.0.3). Allocation concealment was ensured through the use of sealed, opaque envelopes, which were opened immediately before device insertion. Due to the distinct characteristics of the devices, the anesthesiologists performing the insertions were not blinded. However, outcome assessors and data analysts were blinded to the group assignments.
Anesthetic protocol
Standard fasting guidelines (6 hours for solids, 2 hours for clear fluids) were followed. No premedication was given to standardize the protocol. Routine monitoring included electrocardiography, non-invasive blood pressure, pulse oximetry, capnography, and temperature monitoring. Anesthesia was induced in a dedicated pediatric induction room with parental presence to reduce anxiety [9]. Induction was achieved using a face mask with sevoflurane in a 50 : 50 mixture of nitrous oxide and oxygen. After peripheral intravenous cannulation, fentanyl (2–3 μg kg–1) and propofol (3 mg kg–1) were administered. Anesthesia was maintained with sevoflurane (2–3%) in a 33% oxygen and 66% nitrous oxide mixture.
Device insertion
Two experienced pediatric anesthesiologists (M.S. and L.G.), each with over 100 prior insertions of both devices, performed all insertions to ensure proficiency.
Insertion procedure: (1) Devices were lubricated with sterile, water-based gel (K-Y Jelly, Johnson & Johnson, USA). (2) Patients were positioned in the “sniffing” position to optimize airway alignment. (3) Devices were inserted using the manufacturer-recommended blind insertion technique. (4) LTS-D: Cuff inflation was performed with 35 mL of air using a color-coded syringe, maintaining intracuff pressure at ≤ 60 cmH2O via a pressure gauge. (5) The i-gel was inserted without cuff inflation, simplifying the process. (6) Adjustments such as head repositioning, jaw thrust, or device repositioning were allowed if ventilation was inadequate. Major interventions, including reinsertion or switching device size, were permitted for persistent ventilation failure. A second insertion attempt was allowed before proceeding to tracheal intubation. (7) A lubricated 10 Fr gastric tube (Haiyan Kangyuan Medical, Zhejiang, China) was inserted through the gastric channel of each device to assess insertion success and evacuate stomach contents.
Outcome measures
Primary outcomes included oxygen saturation (SpO2) continuously monitored and recorded throughout the procedure, and end-tidal carbon dioxide (EtCO2) measured via capnography.
Secondary outcomes were: (1) device insertion time: defined as the time from facemask removal to achieving a stable square-wave capnograph tracing, measured with a stopwatch by an independent observer; (2) adjustment maneuvers: adjusting head position, jaw lift, pushing or pulling the device, changing the device size, or performing a second attempt; (3) gastric tube insertion: success rate and ease of insertion; (4) oropharyngeal leak pressure: measured by closing the expiratory valve at a fresh gas flow of 3 L min–1 and noting the airway pressure at which an audible leak occurred; (5) fiberoptic visualization: assessed using a 2.8-mm fiberoptic bronchoscope (Storz GmbH, Tuttlingen, Germany) and laryngeal view graded with the Brimacombe Score [10] (1: vocal cords not visible, 2: vocal cords and anterior epiglottis visible, 3: vocal cords and posterior epiglottis visible, 4: only vocal cords visible); (6) Vt: inspiratory and expiratory Vt; (7) anesthesiologist satisfaction and ease of insertion: rated on a 5-point Likert scale [11], where higher scores indicated greater satisfaction; (8) ease of insertion: graded as, 1: very difficult, 2: difficult, 3: easy, or 4: very easy; (9) perioperative adverse events: classified as mild (blood-stained device, gagging), moderate (sore throat, hoarseness), or severe (hypoxia, regurgitation, or gross blood staining).
Data collection
Intraoperative data (SpO2, EtCO2, and Vt) were recorded at 5-minute intervals for 30 minutes after device insertion by a blinded observer. Postoperative complications were assessed in the post-anesthesia care unit (PACU) and during follow-up calls conducted 24 hours after surgery.
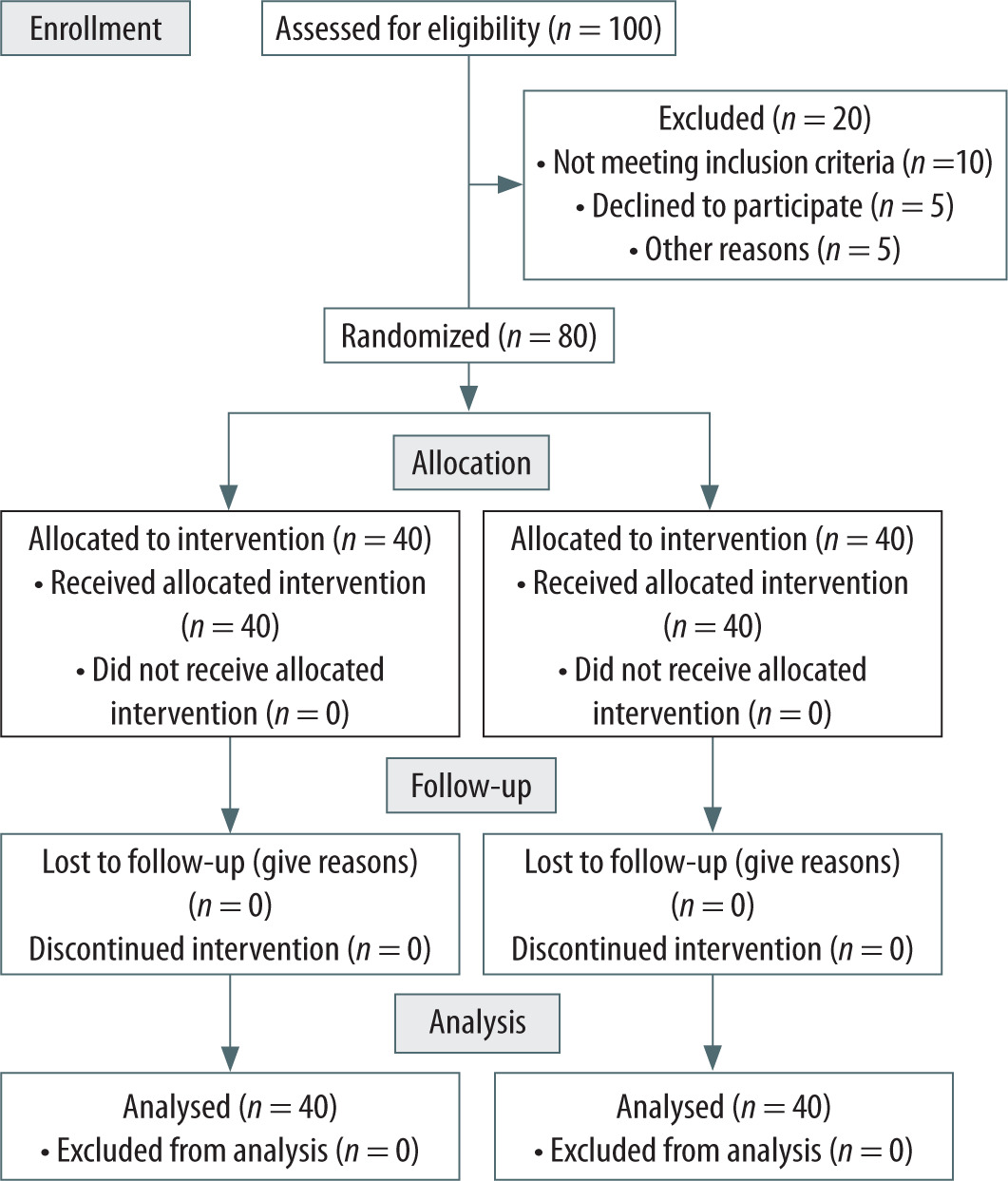
FIGURE 2
CONSORT-style flow diagram of patient enrollment, randomization, allocation, follow-up, and analysis
Statistical analysis
The sample size was calculated to detect a 3% SpO2 and 5 mmHg EtCO2 difference with 95% power and a = 0.05, requiring at least 39 patients per group, plus allowance for dropouts. These thresholds were chosen for their physiological relevance and alignment with pediatric anesthesia studies and guidelines on hypoxia (SpO2 < 95%) and hypercapnia (EtCO2 > 50 mmHg).
Data analysis was performed using SPSS (v27, IBM Corp.). Repeated measures ANOVA was used to compare continuous variables, while Fisher’s exact test was used to analyze categorical data. Equivalence was assessed with the two one-sided tests (TOST) procedure, and Bonferroni corrections were applied for multiple comparisons. A P-value < 0.05 was considered statistically significant.
RESULTS
A total of 100 patients were assessed for eligibility, of whom 80 met the inclusion criteria and were enrolled after obtaining parental consent. All enrolled patients completed the study and were randomized to the two groups (LTS-D and i-gel). Twenty patients were excluded for not meeting the inclusion criteria, as illustrated in the CONSORT flow diagram (Figure 2). Patient demographics and peri-operative characteristics were comparable between groups, ensuring baseline homogeneity (Table 1).
Oxygen saturation (SpO2), end-tidal carbon dioxide (EtCO2), inspiratory and expiratory Vt, and the clinical characteristics related to device performance are shown in Table 2 and Figures 3 and 4.
Primary outcomes
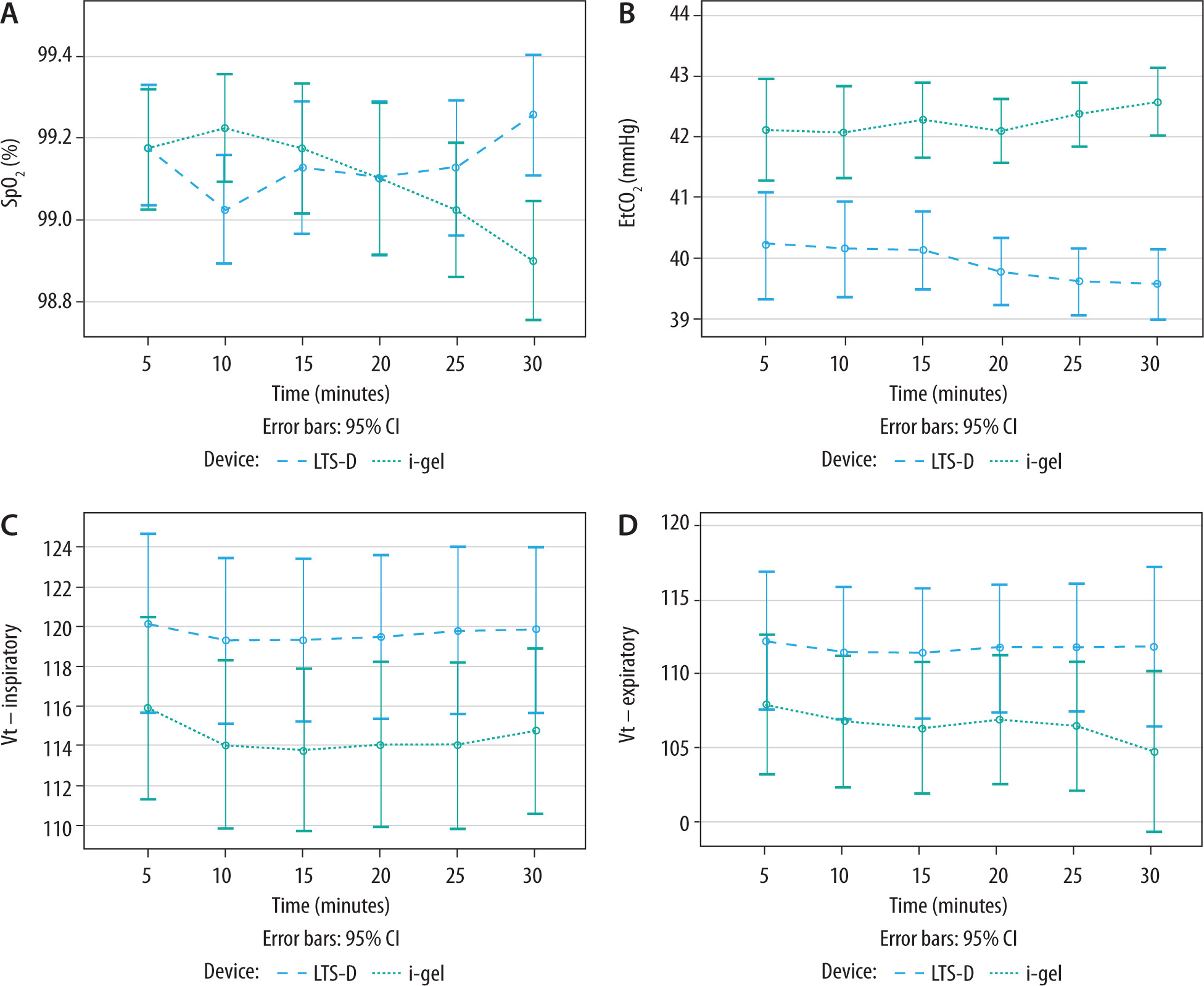
SpO2 remained consistently above 98% in all patients, with no desaturation below 95% or significant intergroup differences (P = 0.96; Table 2, Figure 3A). EtCO2 was within normal limits, though slightly higher with the i-gel (42.13 ± 0.58 mmHg vs. 39.57 ± 0.45 mmHg, P < 0.001; Table 2, Figure 3B), but not clinically significant.
Secondary outcomes
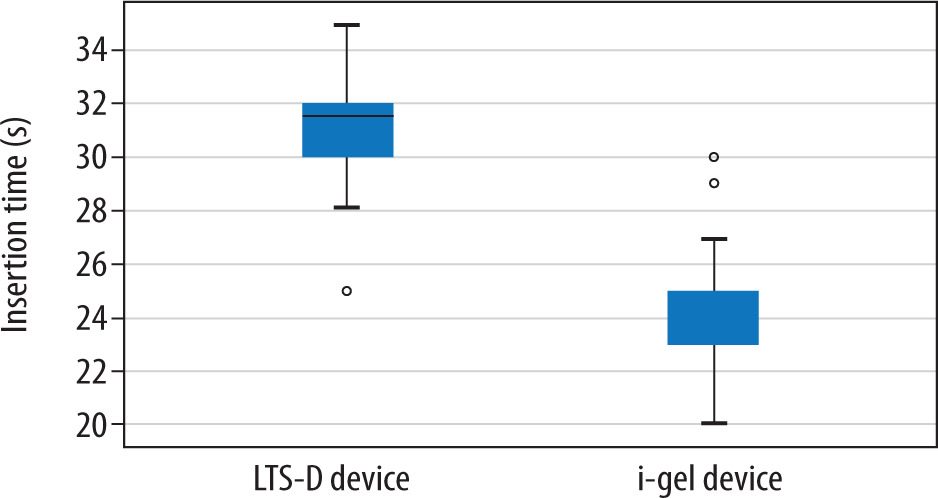
The i-gel allowed significantly faster insertion (24.53 ± 2.00 s vs. 31.20 ± 1.95 s, P < 0.001, Figure 4), while the LTS-D achieved higher oropharyngeal leak pressures (37.63 ± 3.71 cmH2O vs. 24.43 ± 1.72 cmH2O, P < 0.001). Head/neck adjustments were more frequent with the LTS-D, but gastric tube insertion was 100% successful in both groups.
TABLE 2
Comparison of primary and secondary outcomes between the laryngeal tube suction disposable (LTS-D) and i-gel in pediatric patients undergoing elective surgery under general anesthesia with spontaneous ventilation
Fiberoptic evaluation favored the i-gel, with 99% achieving optimal visualization (grades 3–4) vs. 70% for LTS-D (P < 0.001). Vt were comparable (P = 0.25), with no significant differences in inspiratory or expiratory volumes (Figures 3C–D).
Anesthesiologist satisfaction was high for both devices, with no differences in ease of insertion (P = 0.16). Adverse events were minimal, with mild complications (blood-stained devices, sore throat) occurring in 17.5% (LTS-D) vs. 12.5% (i-gel) (P = 0.65). No severe complications (hypoxia, regurgitation) were observed.
DISCUSSION
The findings of this study demonstrate that both the LTS-D and i-gel are effective and safe devices for airway management in non-paralyzed pediatric patients undergoing short-duration elective procedures under general anesthesia with spontaneous ventilation. Both devices maintained comparable SpO2 levels, with no episodes of desaturation, underscoring their efficacy in ensuring adequate oxygenation. While the i-gel group exhibited slightly higher EtCO2 levels than the LTS-D group, these differences were not clinically significant, as all values remained within normal physiological ranges.
A growing body of evidence supports the increasing use of second-generation SGAs as an alternative to endotracheal intubation in pediatric airway management [12–14]. These devices are associated with reduced recovery times, lower rates of airway trauma, and greater ease of use [15, 16]. Recent meta-analyses highlight the importance of tailoring SGA choice to the specific needs of the procedure and patient, based on factors such as sealing pressures, insertion speed, and safety [15, 17]. To the best of our knowledge, this is the first study to directly compare the clinical performance of the updated LTS-D and i-gel in pediatric patients. The findings provide valuable insights into the unique strengths of each device, aiding clinicians in tailoring airway management strategies.
FIGURE 3
Comparison of oxygen saturation (SpO2), end-tidal carbon dioxide (EtCO2), and inspiratory and expiratory tidal volumes (Vt) between the laryngeal tube suction disposable (LTS-D) and i-gel devices
One of the most striking differences observed was the significantly faster insertion time of the i-gel compared to the LTS-D. This aligns with previous studies [17–19] highlighting the simplicity of the i-gel’s design, which eliminates the need for cuff inflation and reduces procedural complexity [20]. Faster insertion times may be particularly advantageous in emergency scenarios or when rapid airway establishment is critical [21]. Conversely, the prolonged insertion time associated with the LTS-D is likely due to the additional steps required for cuff inflation and subsequent adjustments. Furthermore, the LTS-D required more frequent head or jaw adjustments to achieve effective placement, suggesting slightly greater complexity in its use [22].
The LTS-D performance in achieving higher oropharyngeal leak pressures compared to the i-gel reflects its superior sealing capacity. These findings are consistent with previous studies [23, 24]. This feature is particularly valuable in scenarios requiring high airway pressures, such as mechanical ventilation, poor lung compliance, or the need to limit ventilatory pressures to prevent gastric insufflation. While such high sealing pressures are not typically necessary during non-paralyzed mechanical ventilation, the enhanced sealing provided by the LTS-D may prove advantageous in specific clinical contexts [25, 26]. These differences underline the importance of tailoring device selection to specific surgical or patient requirements [27].
Fiberoptic evaluation revealed a significant advantage for the i-gel, with superior anatomical positioning and optimal visualization of the vocal cords in nearly all cases. This finding is clinically relevant, as precise positioning reduces ventilation-related complications and facilitates tracheal intubation. Conversely, the LTS-D, consistent with previous studies [27], exhibited suboptimal fiberoptic views in some cases, although adequate ventilation was always achieved. The thermoplastic elastomer construction of the i-gel likely enhances its natural airway conformity, minimizing the need for adjustments [5, 19].
Vt, both inspiratory and expiratory, were comparable between the LTS-D and i-gel, demonstrating their effectiveness in supporting spontaneous ventilation during short procedures. The i-gel’s anatomically shaped airway seal ensures reliable performance without epiglottic fins, which may obstruct the airway due to epiglottic folding in other devices. Similarly, the LTS-D’s multiple ventilation apertures likely prevent soft tissue obstruction, further ensuring effective ventilation.
High satisfaction ratings from anesthesiologists for both devices further support their usability and reliability in pediatric airway management. However, the need for more frequent adjustments with the LTS-D may indicate a minor disadvantage in ease of use compared to the i-gel.
The safety profiles of both devices were excellent, with no severe complications such as hypoxia or regurgitation observed [20]. Mild adverse events, such as sore throat or minor blood staining, occurred at similar rates in both groups and were consistent with previous studies [28, 29].
Although this trial focused exclusively on elective pediatric cases under spontaneous ventilation, it is important to contextualize our findings within the broader scope of SGA performance. Several studies have evaluated the efficacy of LTS-D and i-gel devices in controlled ventilation settings or emergency scenarios, primarily in adult populations [30–33]. For instance, their use has been explored in out-of-hospital cardiac arrest [32, 34] and military environments [33], demonstrating variable first-pass success rates and ventilation efficacy. One pediatric study, conducted in a prehospital setting, assessed ventilation performance using manual resuscitators in moving ambulances [35]. While these contexts differ significantly from our study population, they underscore the adaptability of these devices across clinical conditions and warrant further pediatric-specific investigation.
This study provides valuable insights into the comparative performance of the LTS-D and i-gel in pediatric airway management, but several limitations must be noted. First, generalizability is limited, as the study included only ASA I children aged 2–8 years undergoing short elective surgery. The findings may not apply to neonates, infants, or high-risk pediatric populations with comorbidities requiring different airway strategies. The small, homogeneous sample and single-center design further restrict external validity. Second, the study lacked long-term follow-up on airway-related complications. While both devices showed good intraoperative safety, postoperative issues such as stridor, persistent sore throat, or mucosal injury were not assessed beyond 24 hours. Future studies should incorporate extended follow-up to detect delayed adverse events. Third, operator experience may have influenced the results, as all insertions were performed by two experienced anesthesiologists. While this approach ensured procedural consistency and minimized confounding factors, it may limit the generalizability. Whether the findings are replicable among less experienced clinicians remains uncertain. Including a broader range of providers in future studies would help evaluate the external validity of these results. Moreover, exploring the learning curve and implications for clinical training could enhance the practical applicability of both devices in routine pediatric anesthesia. Finally, cost-effectiveness was not evaluated, although it could provide valuable insights for resource-limited settings. Addressing these limitations in future research would enhance the clinical applicability and broader relevance of these findings.
CONCLUSIONS
Both the LTS-D and i-gel are effective and safe for pediatric airway management in non-paralyzed children undergoing short elective surgical procedures. Both ensured adequate oxygenation and ventilation, but their design differences offer distinct advantages. The i-gel allows faster insertion and better anatomical positioning, ideal for time-sensitive cases, while the LTS-D provides higher oropharyngeal leak pressures, benefiting patients needing enhanced sealing capacity (e.g., reduced pulmonary compliance).
Device selection should be context-driven, considering time constraints, airway seal needs, and provider experience. Future studies should assess high-risk pediatric populations, long-term complications, and usability among less experienced clinicians to improve clinical applicability.