
Despite significant advancements in emergency medicine in recent years, mortality rates from cardiac arrest (CA) still remain unacceptably high. According to the European Resuscitation Council registry, survival rates after out-of-hospital cardiac arrest (OHCA) reach an average of 8% at discharge from hospital [1]. Accurate identification of patients with reversible causes of circulatory arrest and implementation of appropriate therapies to improve outcomes continue to present significant challenges for medical teams [2]. Importantly, a substantial proportion of patients fail to regain spontaneous circulation despite advanced life support. These individuals may benefit from the addition of extracorporeal membrane oxygenation (ECMO) to standard advanced life support. Studies have shown that, in carefully selected patient populations, extra-corporeal cardiopulmonary resuscitation (ECPR), compared to conventional cardiopulmonary resuscitation (CPR), leads to improved restoration of systemic perfusion and oxygenation and reduces tissue hypoperfusion, ultimately increasing the likelihood of return of spontaneous circulation and reducing the risk of poor prognosis [3, 4]. Although ECPR is emerging as an attractive method of advanced care for patients with refractory CA, its implementation remains limited to a few centres in Poland, primarily those with cardiothoracic surgery capabilities.
Furthermore, there is a growing consensus that such advanced procedures should be performed exclusively in high-volume, specialized centres with extensive experience. This presents a significant barrier to initiation of ECPR programmes by other institutions that have not yet implemented this intervention. However, in 2023, according to the Extracorporeal Life Support Organization (ELSO), there were 570 extracorporeal life support (ECLS) centres registered and a total number of 18 992 ECPR treatments were carried out, including 17 444 procedures in adults, with survival at hospital discharge reaching 31% [5]. This means that even experienced centres perform ECPR therapy no more than a dozen times yearly. Moreover, the consensus among experts and the available evidence suggest that a minimum of 12 procedures per year performed by a centre is associated with an adequate quality of ECPR, resulting in improved survival rates among patients receiving this intervention [6]. Thus, building upon our extensive experience with veno-venous ECMO therapy over recent years, we decided to expand our efforts to improve outcomes for patients with refractory CA. We have undertaken organizational initiatives and implemented an ECPR programme at our centre. The objective of this study was to document our initial experience with the implementation of the ECPR programme at the University Hospital in Kraków, with a particular focus on analysing the periprocedural results and outcomes of consecutive patients who were determined to be eligible for ECPR according to our established protocol during the first year of our ECPR programme. In addition, we aimed to compare our results with those from other experienced centres.
METHODS
Setting
The University Hospital in Kraków is the largest supraregional, 1100-bed university hospital in Poland and serves as a referral centre for refractory CA in the region. In May 2023 we initiated an ECPR programme to improve survival of patients with OHCA. A dedicated ECPR team was established among Intensive Care Unit (ICU) personnel consisting of anaesthesiology and intensive care specialists, senior ICU nurses and paramedics. The team collaborated closely with specialists from the Emergency Department, Cardiology and Cardiovascular Interventions Clinical Department and Vascular Surgery Clinical Department.
ECPR eligibility protocol and patient flow
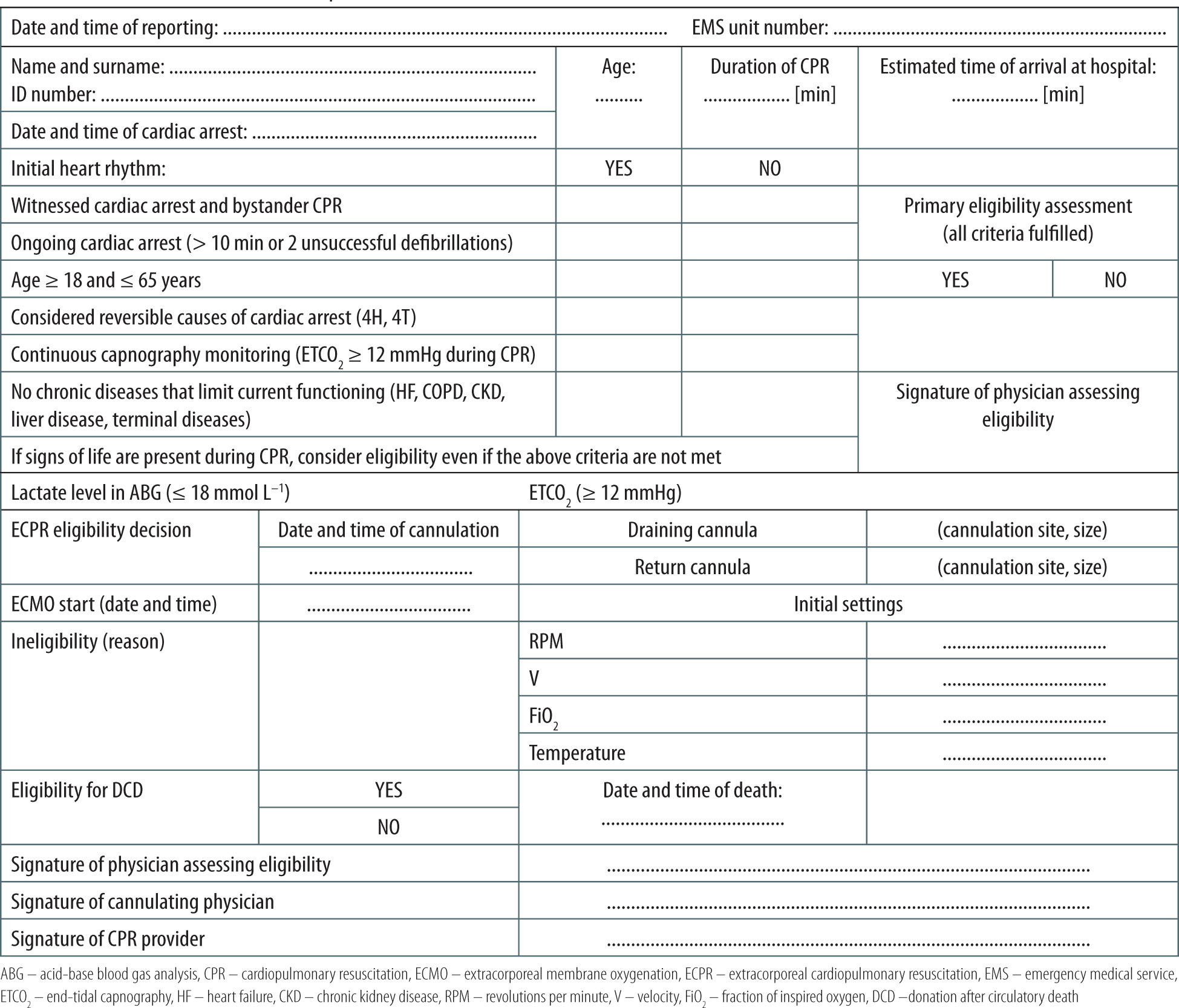
A detailed eligibility protocol was developed prior to the start of the ECPR programme in accordance with ELSO guidelines and based on an analysis of analogous protocols from experienced domestic and foreign ECPR centres. The detailed inclusion/ exclusion criteria are presented in Table 1.
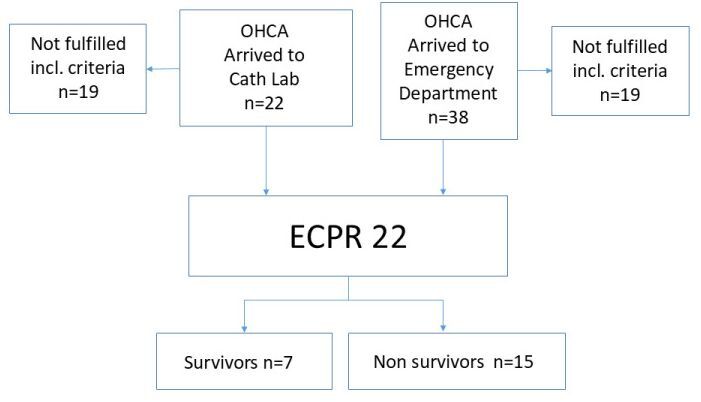
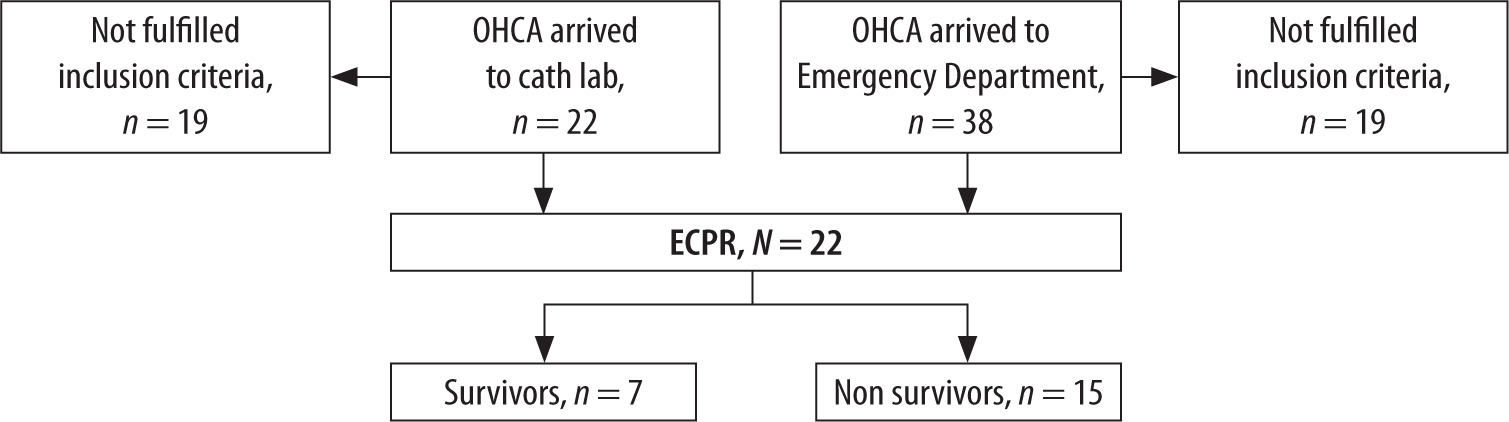
During the analysed period, 60 patients undergoing resuscitation due to OHCA were admitted to the University Hospital (38 to the Emergency Department, 22 to the Catheterization Laboratory). Among them, 22 patients met the inclusion criteria and did not meet the exclusion criteria for ECPR. The patients’ flow chart is presented in Figure 1.
Task allocation during ECPR procedure
To ensure effective coordination of the entire ECMO team during ECPR in patients with OHCA, a standardized protocol – adapted to situational demands – should be established and consistently applied. The ECPR team consists of two anaesthesiology and intensive care specialists dedicated to vascular cannulation, an experienced physician in training responsible for securing the airway, a para-medic conducting Advanced Life Support (ALS), and an anaesthetic nurse assisting with the cannulation procedure. Upon receiving a telephone alert, the team transports a cart with essential cannulation equipment and the ECMO console to the designated location in the hospital. The ECMO circuit is pre-primed and ready for immediate deployment, ensuring rapid response when needed. While awaiting the patient, roles are clearly assigned among the personnel. Two of the most experienced vascular cannulation specialists on duty are assigned to perform the procedure. Upon patient handover from the emergency medical services team, vital signs are assessed. The paramedic assumes responsibility for ALS, and the anaesthesiologist responsible for airway management secures the airways, conducts mechanical ventilation, collects arterial blood for point-of-care testing and initiates direct arterial blood pressure monitoring. Meanwhile, the cannulation team gathers a history from the emergency medical team, confirming the duration and circumstances of CA. After arterial blood gas analysis, the patient undergoes final eligibility assessment for ECPR based on established criteria (Table 1). If the patient is deemed eligible, the cannulation team proceeds with the procedure. Under ultrasound guidance, guidewires are inserted into the femoral vein and artery in the same groin. After confirming the correct placement of guide-wires, the cannulas are inserted into the femoral vessels. Upon successful insertion and verification of the cannulas’ position and patency, the anaesthesiologist managing the airway hands over sterile tubing to connect to the ECMO system. The console is gradually activated until a flow of 3 L min–1 is achieved and chest compressions are discontinued. Post-resuscitation care for ECPR patients is provided by anaesthesiology and intensive care specialists in the ICU.
Data collection and study endpoints
A prospective registry of consecutive patients managed by our ECPR team has been undertaken since initiation of the ECPR programme. Herein, we performed a detailed analysis of periprocedural results and the outcomes from the first year of this registry. Specifically, we studied clinical data of all consecutive refractory OHCA patients who were treated with ECPR in the University Hospital in Kraków between May 2023 and May 2024. Baseline patients’ characteristics, pre-hospital and in-hospital care, time intervals from CA to ECMO flow, neurological and survival status and peri-procedural complications were collected in our registry. The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Committee on Research Ethics of Jagiellonian University, decision number 118.0043.1.50.2024.
Primary and secondary outcomes
Primary outcomes included survival at 3 months and survival with a good neurological outcome, defined as a score of 1 or 2 on the Cerebral Performance Category (CPC) Scale [7] at 3 months. The CPC Scale is a standardized five-point scale used to assess neurological outcomes, particularly in evaluating post-resuscitation cerebral function. Among the five categories of the CPC Scale, CPC 1 is considered the most favourable neurological outcome. It reflects a state of good cerebral performance, where the patient is fully conscious, alert, and functionally independent.
In contrast, CPC 2 corresponds to moderate cerebral disability, indicating a less favourable, though still acceptable, neurological outcome. Patients classified as CPC 2 are conscious and able to perform independent activities of daily living, such as eating, dressing, and walking without assistance.
Secondary outcomes included the time interval between CA and ECMO flow initiation and the occurrence of serious traumatic or haemorrhagic adverse events due to the ECPR procedure, including pneumothorax, pulmonary haemorrhage, intra-abdominal bleeding, cardiac tamponade, aortic dissection or vascular injury/cannula site bleeding.
Statistical analysis
Categorical variables were presented as numbers and percentages. Continuous variables were expressed as means and standard deviations (SDs) or medians and interquartile ranges (IQRs). Due to the descriptive nature of the study and lack of control group, no advanced statistical analyses were performed. All calculations were performed using IBM SPSS Version 22 (IBM Corp.).
RESULTS
Baseline characteristics of study subjects
The study enrolled 22 consecutive patients who received ECPR for OHCA. There were 17 males (77.0%), and the median age of the study group was 44.5 (38.3–62.0) years. The primary cause of CA was acute myocardial infarction (n = 7), while other aetiologies included massive pulmonary embolism (n = 5), drowning (n = 2), electrical storm (n = 2), and electrolyte imbalances (n = 2). All 7 patients with acute myocardial infarction underwent coronary angiography, and percutaneous coronary intervention was performed in all of the cases. In addition to ECMO, 1 patient received an intra-aortic balloon pump (IABP) and 2 patients received an Impella CF device as an additional mechanical circulatory support. The mean length of ECMO therapy in the ICU was 1.5 days. Demographic and clinical characteristics of patients with OHCA are presented in Table 2.
Primary and secondary outcomes
The survival rate at 3-month follow-up was 31.8%. Survival with a good neurological outcome (score of 1 or 2 on CPC Scale) at 3-month follow-up was 27.3%. All the patients were cannulated with a percutaneous technique either in the Emergency Department (54.5%), ICU (31.8%) or Catheterization Laboratory (13.6%), and ECMO flow was established after a median of 15.0 (10.0–30.0) minutes from hospital admission. As part of our institutional ECPR eligibility protocol, we included the measurement of end-tidal carbon dioxide (ETCO2). A value below 12 mmHg, in the absence of signs of life, was considered an exclusion criterion for initiating ECPR. Notably, there was a difference in mean ETCO2 values between survivors (14 mmHg) and non-survivors (17 mmHg). The time from the onset of cardiac arrest to the initiation of extracorporeal circulation (achieving ECMO flow of at least 3 L min–1) also differed considerably between the groups. In the overall study cohort, the median duration was 59.5 minutes, with a marked difference observed between survivors and non-survivors (36 minutes vs. 63 minutes, respectively).
TABLE 2
Demographic and baseline characteristics of patients who received extra corporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest
A 100% cannulation success rate was achieved for ECPR during the analysed time period. In one case, cannulation was complicated by a perforation of the right femoral artery, requiring endovascular repair. Additionally, four cases of bleeding from the ECMO cannulation site were observed, but all of them were minor and did not require surgical intervention. No pneumothorax, pulmonary haemorrhage, intraabdominal bleeding, cardiac tamponade or aortic dissection related to ECPR procedure was observed in our study group (Table 3).
DISCUSSION
Our satisfactory periprocedural results and outcomes obtained after 1 year since implementation of ECPR prove that it is possible to launch an ECPR programme with initial results consistent with those coming from experienced centres. In our opinion, adequate training, attainment of the necessary clinical skills, and efficient communication between team members, a carefully designed organization and strict eligibility criteria are crucial for success.
Although ECPR is a high-risk medical procedure, it has been shown to offer the possibility of saving a selected group of patients experiencing refractory OHCA with favourable neurological outcomes [8]. According to current analyses, the use of ECPR in cases of refractory OHCA can increase patient survival rates from an average of 8% to approximately 30% [1, 5]. However, the implementation of this new and advanced type of intervention in the hospital should be preceded by a thorough analysis of demand, as an adequate volume of interventions annually is necessary to ensure quality [8]. In the case of ECPR, experts suggest that high-volume ECMO centres with more than 12 ECMO cases annually have demonstrated improved survival rates [6]. To define the needs related to OHCA care in our hospital, we analysed all admissions due to OHCA over several preceding years and confirmed that at least a dozen patients annually are likely to fulfil the inclusion criteria for ECPR according to ELSO guidelines. These results are in concordance with studies on OHCA based on a population from our region and town indicating that there are approximately 50 cases of cardiac arrest (CA) per 100,000 residents with the frequency rate for bystander CPR initiation before the arrival of the emergency medical team reaching 52.2% of cases and with absence of ROSC in 57.2% of patients with OHCA [9, 10]. Consequently, we concluded that, firstly, there is a need to implement such a programme in our region, and secondly, that we would be able to perform in our hospital a sufficient number of procedures annually to ensure that our volume guarantees obtaining adequate quality required for conducting ECPR.
TABLE 3
Periprocedural results and remote outcomes
TABLE 4
Comparison of outcomes in our registry (ECPR for Kraków) and in studies from experienced extra corporeal cardiopulmonary resuscitation centres (ARREST, Prague OHCA, and INCEPTION studies)
[i] aLack of data for survival irrespective of neurological outcome at 3-month follow-up for Prague OHCA and INCEPTION studies; available data for survival with good neurological outcome (CPC 1 or 2) at 30-day follow-up. bLack data for neurological outcome at 3-month follow-up. cAvailable data for survival with favourable neurological outcome (CPC 1 or 2) at 30-day follow-up. dLack of data for interquartile range. e For generalizability issues and reporting of overall study numbers, median and IQR were converted to median and SD.
CPC – Cerebral Performance Category Scale, CA – cardiac arrest, ECMO – extracorporeal membrane oxygenation
Implementing the ECPR programme presents a significant challenge for the entire team and requires extensive theoretical and practical training before this procedure can be launched. This is in accordance with the expert consensus document outlining the necessary training and accreditation requirements for performing extracorporeal cardio-pulmonary resuscitation [11]. Our team members had pre-existing proficiency in advanced vascular access procedures and were involved in managing patients with severe acute respiratory distress syndrome (ARDS) using veno-venous ECMO during the COVID-19 pandemic when our hospital was converted temporarily into an infectious disease hospital dedicated to COVID-19 treatment of patients from the whole macro-region. Thus, our experience encompassed the entire spectrum of care, from cannulation and console management to troubleshooting, weaning from ECMO, and eventual decannulation [12].
Before the initiation of the ECPR programme, our team actively participated in training courses at renowned ECMO institutions both domestically and internationally. To further enhance our preparedness, we have organized multiple ECPR simulations within the University Hospital in Kraków, as well as in external settings such as the 12th Polish University Championships in Medical Rescue and through collaborative sessions with ECMO company personnel.
Precise selection criteria and the establishment of an appropriate inclusion/exclusion protocol are essential for every ECPR programme. Based on the ELSO guidelines and the results from recent studies (INCEPTION [15], ARREST [14], Prague OHCA [14]), in addition to the patient’s prior functional status and absence of severe comorbidities, time is a critical factor in the success of ECPR [13–15]. Consequently, it seems to be reasonable to deem patients eligible if CA occurred in the presence of witnesses, no-flow time was less than 5 minutes, and the time from CA to the initiation of ECPR did not exceed 60 minutes [13–15]. After careful revision of the expert consensus and the findings from the abovementioned studies, our institution developed a precise inclusion and exclusion protocol for ECPR in order to attain comparable outcomes to those achieved by centres with extensive experience.
Our outcomes were comparable to those achieved by high-volume centres with extensive experience in ECPR. In the first year of our hospital’s ECPR programme, we observed a 31.8% survival rate, with 27.3% of patients achieving a favourable neurological outcome. This is noteworthy in light of the survival rates reported in three major randomised trials conducted by expert centres: 43.0% in ARREST [13], 23.9% in PRAGUE OHCA [14], and 20.0% in INCEPTION [15] (Table 4). Cannulation time during conventional CPR is an additional benchmark of ECPR team efficiency. The PRAGUE OHCA [14] trial reported a median cannulation time of 12 minutes, INCEPTION 20 minutes [13], and ARREST 7 minutes [15]. A 10-year experience from a high-volume ECPR centre in Milan reported a median of 15 minutes [19]. During the initial year of the ECPR programme at University Hospital in Kraków, the median cannulation time during CPR was 15.5 minutes, indicating that we quickly reached a level of performance comparable to established centres. Notably, our ICU is staffed 24/7 by at least two physicians trained in cannulation and ECPR initiation.
Interdisciplinary collaboration among a diverse range of specialists, including anaesthesiologists, intensivists, emergency physicians, interventional cardiologists, vascular surgeons and emergency medical teams, is essential for the successful implementation of such advanced procedures. Our centre, unlike most other academic ECPR centres, lacks both cardiac surgeons and perfusionists. Despite these limitations, an analysis of our outcomes and safety endpoints demonstrates that with appropriate organization and commitment from a carefully selected team, a successful high-level ECPR programme can be implemented even in centres without cardiac surgery capabilities. However, considering the high incidence of CA secondary to myocardial infarction, close collaboration between the ECMO team and interventional cardiologists is crucial for the successful implementation of an ECMO programme [17–19].
Despite promising initial results, we are aware that many challenges lie ahead in order to sustain and continually improve our efforts aimed at increasing the chances of survival with good neurological outcomes among patients after CA. Furthermore, we recognize the importance of continuous education and training for our team to minimize periprocedural adverse events and cannulation failures.
LIMITATIONS
This study has several limitations. First, its retrospective and single-centre design limits generalisability, and no control group was included for comparison. The follow-up was censored, and neurological outcomes were assessed retrospectively. Importantly, the study cohort was clinically heterogeneous in terms of prehospital management, arrest aetiology, and time intervals to ECMO initiation, which may have influenced outcomes and limits the interpretability of subgroup findings. Furthermore, no direct comparison was made between our results and those reported by other centres, which restricts broader contextualization. The absence of detailed patient histories and long-term quality-of-life data in survivors further limits the depth of analysis and highlights the need for more comprehensive, standardised data collection in future prospective studies.
CONCLUSIONS
The results from the first year of our ECPR programme demonstrate that the implementation of this advanced resuscitative strategy is feasible in a newly established centre, with encouraging short-term survival and neurological outcomes. Further prospective evaluation with larger patient cohorts and long-term follow-up is warranted to validate these findings and guide the future development of ECPR programmes in similar settings.