
Due to the high heterogeneity of this population, providing anaesthesia for paediatric patients poses distinct challenges, especially those who perform anaesthesia mainly on adults. A completely different group is children under 3 years of age, for which the Section of Paediatric Anaesthesiology and Intensive Therapy of the Polish Society of Anaesthesiology and Intensive Therapy has prepared a consensus statement on anaesthesia for children under 3 years of age. Nevertheless, the recommendations contained in this statement, concerning children over 3 years of age and adolescents, are an integral and compatible part of the document cited above.
The standards for the provision of services in the field of paediatric anaesthesiology are regulated by the principles contained in the uniform text of the Regulation of the Minister of Health on the organizational standard of health care in the field of anaesthesiology and intensive care of 2016, containing requirements regarding the conditions and equipment of the anaesthesia workstation for patients, taking into account differences resulting also from their age, as well as the principles of comprehensive perioperative care in hospitals where procedures are performed on children. The hospital is obliged to create appropriate conditions for hospitalization of children before and after surgery, also by establishing a Department of Paediatric Anaesthesiology or a Department of Paediatric Anaesthesiology and Intensive Therapy [1]. The principle in perioperative medicine is the concept of enhanced recovery after surgery (ERAS) to improve the results of surgical treatment through a comprehensive approach to the patient in pre-, intra-, and postoperative periods [2]. It was initially developed for the adult patient population, but for many years, the process of implementing the above principles has also been observed in the paediatric population. Some elements of this concept also concern anaesthetic measures, such as shortening the fasting time before anaesthetic administration, avoiding pharmacological premedication, multimodal analgesia including regional anaesthetics, etc., which should be implemented already in the preoperative period. In the postoperative period, the following measures are recommended: early introduction of oral nutrition, prevention of postoperative nausea and vomiting, pain treatment with non-opioid analgesics or continuous regional analgesia techniques.
This holistic approach improves the effectiveness and safety of the patient in the perioperative period and, moreover, contributes to increased treatment efficiency and satisfaction – both for the child and their parent/legal representative/de facto guardian.
Anaesthesia in children over 3 years of age carries a risk of adverse events, although lower compared to younger children, as confirmed by the APRICOT (Anaesthesia PRactice In Children Observational Trial) study from 2017 [3]. It has been shown that the frequency of serious adverse events in the perinatal period decreases by 12% with each year of the child’s life. However, it should be noted that in this group, patients with complex congenital defects and/or severe systemic diseases requiring multiple and repeated anaesthetic procedures, often with coexisting multi-organ failure resulting from a chronic disease and/or long-term treatment with the use of burdensome pharmacotherapies (e.g., chemotherapy, immunotherapy), are qualified for anaesthesia.
Technological progress and pharmaceutical development have increased the possibilities and hopes for treating diseases that were not so long ago considered incurable in children. Therefore, the range of diagnostic and therapeutic methods has increased, which has forced anaesthesiologists to adapt to the conditions and requirements of modern medicine. Often, these procedures are performed in different centers specializing only in selected disciplines, for example radiology, orthopaedics, ophthalmology, dentistry and others, which prompted the Expert Panel of the Section of Paediatric Anaesthesiology and Intensive Therapy of the Polish Society of Anaesthesiology and Intensive Therapy to update its position on anaesthesia for children over 3 years of age, taking into account anaesthesia in specific selected fields, i.e. dentistry, ENT, orthopaedics, ophthalmology, diagnostics outside the operating room [computed tomography (CT), magnetic resonance imaging (MRI), endoscopy], and in emergency situations.
We hope that this consensus statement, which is a continuation of the consensus statement on anaesthesia for children up to 3 years of age (2025) and an updated document on general and specific recommendations for anaesthesia in children over 3 years of age (2016), will be of interest to physicians undergoing specialist training in anaesthesiology and intensive therapy, as well as all anaesthesiology and intensive therapy specialists who perform anaesthesia in children and adolescents. Some gene ral information concerning the entire child population is described in detail in the first part, referring to children under 3 years of age, while in this document it is supplemented with specific conditions concerning older children. The detailed section contains additional and important tips on anaesthesia in selected areas.
EQUIPMENT IN THE ANAESTHESIA WORKSTATION AND POST-ANAESTHESIA CARE ROOM
The equipment of anaesthesia workstation in facilities providing paediatric anaesthesia services is regulated by the provisions of the 2016 Regulation of the Minister of Health, which is described in detail, taking into account the specificity of the paediatric population, in the “Consensus statement on anaesthesia in children under 3 years of age” [1]. This description includes requirements for both the equipment of the anaesthesia station and the postoperative care room. In addition, special attention should be paid to providing separate rooms for patients from this population, which is especially important when older children and adolescents are operated on in adult hospitals.
PREPARATION FOR ANAESTHESIA
All children, regardless of age, must have a medical history taken and a physical examination performed at least 24 hours before the planned surgery by a specialist in anaesthesiology and intensive therapy, or a physician undergoing specialist training in anaesthesiology and intensive therapy. Most often, an anesthesiology questionnaire is used, containing questions regarding:
current diagnosis and planned type of procedure,
previous course of the disease (which is an indication for surgical treatment or diagnostic testing),
comorbidities,
infectious diseases – especially infections in the 2 weeks preceding anaesthesia, which are a contra-indication to performing the procedure in an elective manner due to the increased risk of intra- and postoperative respiratory complications, although the risk of these complications is much lower in the group of older children and adolescents in whom the process of maturation of the respiratory system has been completed (7–8 years of age),
previous anaesthesia and any events related to it, such as allergic reactions, postoperative nausea and vomiting, postoperative agitation/delirium syndrome, etc.,
family history of hereditary diseases,
vaccinations – for children over 3 years of age; the list includes:
– mandatory vaccinations:
– recommended vaccinations:
a) inactivated: against human papillomavirus (HPV), coronavirus disease 2019 (COVID-19), influenza, hepatitis A virus (HAV), tick-borne encephalitis, meningococcal disease caused by group B meningococci (MenB) and meningococcal disease caused by meningococci of groups A, C, W-135 and Y (MenACWY), or against meningococcal disease caused by group C meningococci (MenC),
b) live: against measles.
The recommended delay in anaesthesia for inactivated vaccines is 2 days, and for live vaccines – 2 weeks.
During this visit, the anaesthesiologist must review the required laboratory and other test results, which are essential for selecting the type of anaesthesia and for determining the risk of intubation due to anatomical abnormalities and/or concomitant pathological changes, such as neoplastic, vascular, or post-traumatic ones. If significant abnormalities are found in the patient’s medical history or physical examination, the anaesthesiologist may order additional tests or specialist consultations.
It is always important to verify that the requested tests and consultations have been completed before initiating anaesthesia.
In patients qualified for anaesthesia and elective surgery, laboratory test results should gene rally be within the age-appropriate reference ranges. The only possible exception concerns children and adolescents with haemato-oncological diseases, for which there are separate recommendations. The patient’s condition should always be optimized and, if possible, the procedure should be postponed until the abnormalities have resolved. In children and adolescents in good general condition and without comorbidities, tests performed within the last three months may be accepted, provided their health status is stable. The scope of tests should be considered individually for each patient. Exclusion from elective anaesthesia and surgery includes, but is not limited to, undiagnosed and uncorrected anaemia, severe electrolyte disturbances, thrombocytopenia, and coagulation disorders. Exact reference values of laboratory tests are described in the section on anaesthesia for children under 3 years of age.
During this visit, the patient’s medications, supplements, and diet (vegan, vegetarian, etc.) must be reviewed to determine which medications should be continued and which require temporary discontinuation or replacement (e.g., anticoagulants). Detailed recommendations for perioperative pharmacological management are described in the aforementioned consensus statement on children under 3 years of age. The physical examination should include, in particular, an assessment of the respiratory, circulatory, and nervous system function. If significant abnormalities are found, additional imaging or functional tests should be considered. An important point of this visit is the assessment of the difficulty of intubation, which in older and cooperative children can be assessed using traditional tools such as the Mallampati test or the Cormack-Lehane scale.
During the anaesthesiological consultation, the principles of child care in the perioperative period, the choice of anaesthesia method, the need for premedication or not, the pain management plan, the principles of prevention and treatment of postoperative nausea and vomiting, the risks and strategies for managing postoperative agitation and/or delirium, as well as the principles of food withdrawal should be explained.
The anaesthesiological consultation concludes with obtaining informed, written consent for anaesthesia. As a rule, in the case of a minor (under 16 years of age) or incapacitated patient, the consent of a parent/legal representative/de facto guardian is required. For patients over 16 years of age, cumulative consent, meaning double consent, must be obtained, allowing the patient to either give or refuse consent. Any disagreement in obtaining cumulative consent should be resolved by the guardianship court.
PREOPERATIVE FASTING
In paediatrics, the 6–4–3–1 feeding withdrawal rule applies, although in the group of patients over 3 years of age, the provision regarding the consumption of mother’s milk is not generally justified. For several years now, a more liberal approach to fluid and/or food intake in the preoperative period has been observed, without evidence of an in creased incidence of aspiration or regurgitation. Therefore, some exceptions are suggested regarding the consumption of a light breakfast or non-clear fluids 4 hours before the planned anaesthesia [4]:
6 hours before anaesthesia: solid foods – R,
4 hours before anaesthesia: light breakfast or unclear liquids (toast with butter and jam or chocolate, natural or fruit yogurt 150 g, oatmeal, cereal or se molina with 3% milk max. 150 g, apple or apple puree max. 150 g, cup of chocolate or flavored milk) – S,
1 hour before anaesthesia: clear fluids (water with or without sugar, clear apple juice, coffee and tea without milk) – R.
However, it is important to emphasize that this exception regarding a light breakfast is only a suggestion (S), not a recommendation (R), and concerns the mode of planned anaesthesia in a healthy child (ASA I). The expert panel of the European Society of Anaesthesiology and Intensive Care recommends developing the local procedure, taking into account the specificity of the hospital, the patient profile, and the range of surgical procedures.
PREMEDICATION
The ERAS concept assumes minimizing or even abandoning pharmacological premedication and replacing it with non-pharmacological methods [2, 5, 6]. These include:
behavioral training (positive reinforcement, repetitive),
systemic desensitization (gradual exposure to stressful stimuli),
mirror techniques (e.g., demonstration on toys or videos),
simulation methods (e.g., diagnostic device simulator – MRI, CT),
distractors (virtual reality [VR], tablets and other electronic devices, games),
PPIA.
However, it seems that it is not possible to eliminate premedication and discontinue its administration, especially in patients with high levels of anxiety (in particular, uncooperative ones). The need for premedication should be discussed with parents/legal representatives/de facto carer(s) and/or patients in whom standard methods may prove ineffective, especially in those with disorders such as autism spectrum disorder, Asperger syndrome, Down syndrome, etc. This group also includes children:
who have undergone repeated anaesthesia,
who have been scheduled for extensive and/or prolonged surgery,
who have been diagnosed with emergence agitation (EA) or postoperative cognitive dysfunction.
In these particularly specific groups of patients, the presence of parents during premedication and induction of anaesthesia may play a particularly beneficial role.
Additionally, it is recommended to use benzodiazepines (midazolam), α2-adrenergic agonists (dexmedetomidine and clonidine), or ketamine. In recent years, α2-adrenergic receptor agonists have been particularly preferred, as their pharmacokinetic and pharmacodynamic profiles are similar to those in adults, allowing standard dosing without age restrictions, and their action after intranasal administration is comparable to that after intravenous administration; however, they require a longer time to achieve the desired effectiveness [7]. Although in this age group of patients, the risk of neurotoxicity of hypnotic drugs is much lower than in children under 3 years of age, reverse/paradoxical reactions, especially to midazolam, can also be observed in older children and adolescents. The choice of this drug may or may not be made by the anaesthesiologist after collecting a detailed medical history from the parent/legal representative/actual guardian and/or patients, who are often able to define their own needs. In this group, rectal administration seems to be unacceptable to most patients, hence the limitation to the following drugs (Table 1).
TABLE 1
Drugs used in premedication in patients over 3 years of age
PREOPERATIVE FLUID THERAPY
Due to the fact that currently preoperative fasting should be very short (1 hour for clear fluids), in the case of anaesthesia for elective surgery, children should not have a fluid deficit and do not require fluid therapy before arrival at the operating theater. Before emergency anaesthesia, the anaesthesiolo-gist should assess the patient in advance to correct any pre-anaesthetic fluid deficiency.
If this is not possible, administering balanced isotonic crystalloid fluids shoul be considered as a bolus or in repeated bolus or in repeated boluses of approximately 10 mL kg–1 intravenously before induction, which may reveal previously hidden hypovolemia. Further fluid therapy depends on the type of surgery and the fluid loss.
INTRAOPERATIVE FLUID THERAPY
The goal of intraoperative fluid therapy is to maintain adequate tissue perfusion during the procedure [8, 9]. It should take into account baseline requirements, ongoing losses, and any prior deficits. Approximate baseline requirements are presented in Table 2.
During anaesthesia, it is recommended to use balanced isotonic crystalloid solutions (fluids containing sodium at a concentration of 130–155 mmol L–1), preferably balanced, without glucose or containing 1% glucose. Balanced crystalloids contain physiological concentrations of chlorides and organic anions, for example: acetate, lactate, gluconate, and malate, which constitute a substrate for the systemic production of bicarbonates, thus providing a buffering effect. In contrast, large volumes of NaCl-based fluids (e.g., 0.9% NaCl, Ringer’s solution) may cause hyperchloremic metabolic acidosis. As a result of the hormonal response to the stress associated with surgery, glucose levels during anaesthesia most often increase despite the supply of glucose-free fluids. However, some patients, due to age, additional health burdens, and the type of surgery and anaesthesia used, may require intraoperative glucose administration and/or frequent monitoring of its concentration (Table 3).
The volume of fluids should be determined by the type of surgical procedure and the patient’s response to fluid therapy, i.e., measured by assessing haemodynamic parameters, tissue flow indicators, and cellular metabolism. Its assessment should be guided by trends in changes of parameters, both physiological – blood pressure, heart rate, diuresis, capillary refill, and laboratory – blood gas values, lac-tate concentration, hemoglobin concentration, and in the case of extensive surgery, additional imaging methods should be used, such as transesophageal echocardiography.
It is usually assumed that the imperceptible losses that should be added to the standard basal requirement are 1–2 mL kg–1 b.w. h–1 for superficial procedures, which generally do not require supplementation, 4–7 mL kg–1 b.w. h–1 for thoracotomy, and 5–10 mL kg–1 b.w. h–1 for abdominal surgery.
TABLE 3
Conditions/situations requiring intraoperative glucose administration and/or glycemic control
POSTOPERATIVE FLUID THERAPY
It is recommended to resume oral fluid (and food) intake as soon as possible. If this is not possible due to surgical reasons or the child’s general condition, it is advisable to transfuse balanced isotonic crystalloids, preferably balanced ones (e.g. Ringer’s lactate, solutions such as Optilyte, Plasmalyte, or Sterofundin) in combination with 5% glucose or a ready-made preparation with 1% glucose, i.e. Benelyte. The starting point for calculating the volume of fluids to be trans-fused should be the basic requirement (Table 2). This volume, depending on the circumstances, should be increased if fluid loss continues or, more frequently, reduced by 30–50%, particularly after extensive surgery when an inappropriately high antidiuretic hormone (ADH) level is expected.
In the case of prolonged fluid therapy, it is necessary to maintain fluid balance, monitor glucose and electrolyte levels (sodium, potassium), and monitor the child’s body weight at least once a day.
In general, in the principles of intra- and postoperative fluid therapy, the use of hypotonic solutions (e.g. 5% glucose, mixtures of 5% glucose with 0.9% NaCl: in volume ratios of 4 : 1, 2 : 1, 1 : 1) is strongly contraindicated due to the risk of developing acute hyponatremia and, consequently, cerebral oedema. This risk is additionally conditioned by potentially inappropriate secretion of the stress hormone, ADH, in the perioperative period. Therefore, the risk of acute hyponatremia also exists in the case of properly conducted fluid therapy with isotonic crystalloids, although it is much less likely.
GENERAL PRINCIPLES OF ANAESTHESIA
Operation plan
The age of the patients should be taken into account when planning the order of operations in the operating theatre and procedures requiring anaesthesia performed outside the operating theatre. The smaller the child, the earlier they should be scheduled for surgery, meaning they should be placed at the top of the schedule to reduce the risk of dehydration and hypoglycemia. However, if fluids are administered, according to guidelines, up to 1 hour before the start of anaesthesia, this risk should not be significant.
Methods of induction
Methods of induction of anesthesia include:
Inhalational induction
Inhalational induction is considered a method that allows for the anaesthesia of children with a high level of needle phobia or in whom establishing vascular access is very difficult (Table 4). The child should be instructed on how to breathe (“like a cosmonaut” or “like a pilot” through a mask, “inflating” a balloon). Induction using physical coercion should be avoided. Inhalational induction in children uses an oxygen-air mixture and an inhalational anaesthetic. The advantages of inhalational induction are its painlessness and reversibility, while the disadvantages include the risk of glottic spasm and a more frequent occurrence of transient postoperative agitation [10–13].
Three methods of inhalational induction are suggested. The first involves gradual increasing the concentration of the inhalation agent, the second involves initially using high concentrations of the inhalation anaesthetic, and the third involves the single-breath or triple-breath vital capacity technique. The second method allows for rapid induction of anaesthesia, which is particularly important in the case of uncooperative patients, but is associated with a much higher risk of undesirable effects (Table 5).
The only anaesthetic suitable for inhalational induction of anaesthesia in children is sevoflurane, which is used at a concentration of 5–8 vol%. For inhalational anaesthesia, concentrations of 6 vol% are recommended for anticipated difficult intubation. Maintaining full airway patency is essential for the safety and effectiveness of this induction method.
Intubation is indicated for procedures lasting longer than 1 hour, performed in the lateral or prone position, and for procedures involving the head and neck.
TABLE 4
Indications and contraindications for inhalational induction in children
| Indications for inhalational induction | Contraindications for inhalation induction |
|---|---|
| Difficult intubation expected | Child’s fear of needles |
| Full stomach | Risk of malignant hyperthermia |
| Difficult vascular access |
TABLE 5
Methods of inhalational induction*
Volatile agents can be used both for induction and maintenance of anaesthesia. An inhalational agent can also be used as the sole anaesthetic drug throughout the entire anaesthesia (VIMA – volatile induction and maintenance anaesthesia), provided that the procedure is not painful. The adopted sequence of procedures should ensure the smooth course of anaesthesia, without disturbing any body functions. Inhalational anaesthetics, as basic elements of anaesthesia, allow for a high degree of flexibility thanks to the rapid control of the depth of anaesthesia and, if necessary, easy transition to more complex techniques using opioids and muscle relaxants. They also allow for rapid recovery from anaesthesia.
TABLE 6
Drugs used for intravenous induction in children and adolescents
TABLE 7
Opioid dosage for intravenous induction
| Drug | Dosage (μg kg–1 b.w.) |
|---|---|
| Fentanyl | 2–5 |
| Remifentanil | 0.5−1 |
| Sufentanil | 0.5−1 |
Inhalational induction is contraindicated in children with hypovolemia, circulatory failure, and right-to-left shunting because myocardial depression and vasodilation may lead to profound hypoperfusion and cardiac arrest in these patients [10, 11].
Intravenous induction
Intravenous induction is possible in children of all ages but requires prior vascular access, which can be difficult and painful in the youngest children. Pain associated with venipuncture should be alleviated by prior application of cream/gel containing a local anaesthetic.
In children, it’s beneficial to have intravenous access established outside the operating room. This reduces unnecessary stress in the operating room for both the child and the staff, and improves workflow. If it is not possible to insert a cannula into the child’s vein in the primary ward and an attempt to insert it in the preparation room is unsuccessful, the induction of anaesthesia is performed by inhalation, and then an intravenous access is established in the already anaesthetized patient. In cases where intravenous access is very difficult to establish, intraosseous access may be used. Drugs used during intravenous induction are presented in Table 6.
To reduce pain at the injection site, analgesics may be administered in advance, before intravenous administration of propofol: fentanyl (1–2 μg kg–1 b.w.) or lidocaine (1–2 mg kg–1 b.w.).
The induction of anaesthesia should be smooth – without fluctuations in blood pressure or heart rate, regardless of the use of intravenous or inhaled agents. The induction should include the following steps:
oxygenation of the patient with a mixture of oxygen and air under the control of arterial blood saturation (saturation of haemoglobin with oxygen; SpO2) (100% oxygen should be avoided),
administration of an induction dose of an anal-gesic,
induction of anaesthesia with an intravenous drug or sedation with a volatile agent,
muscle relaxation,
intubation.
Before administering a hypnotic agent, if intubation is planned, fentanyl (1–2 μg kg–1 b.w.) or sufen- tanil (0.25 μg kg–1 b.w.) must be administered. Strong opioids, such as fentanyl, should be administered by titration to avoid chest muscle stiffness that may occur when the drug is administered too quickly, which may impair proper ventilation of the child (Table 7).
Intranasal induction
This type of induction, which involves administering an anaesthetic and/or analgesic into the nose using a special applicator, in practice means sedation rather than induction of anaesthesia. For this reason, it can be used as a prelude to general or regional anaesthesia, as it facilitates deepening anaesthesia, for example with sevoflurane, in children with severe anxiety and fear of applying a face mask [10, 11].
In children over 3 years of age, vagal stimulation and reflex bradycardia may frequently occur during manipulation in the induction of anaesthesia. Prophylactic administration of atropine is not recommended in this group of patients; however, a syringe with an appropriately prepared solution of this drug should always be prepared before the start of anaesthesia in case its use is necessary urgently.
Intubation
Before performing endotracheal intubation, it is necessary to ensure that the child is anaesthetized and provide adequate oxygenation with a recommended concentration of less than 100%. Due to the rapid onset of action and minimal risk of electrolyte and circulatory disturbances, the use of nondepolarizing agents is recommended. Depolarizing agents, with succinylcholine (suxamethonium) as the only commercially available representative, can be used in exceptional situations, for example a patient undergoing anaesthesia with a full stomach or when difficult intubation is expected, as well as in overweight or obese patients. It should not be used in patients with a diagnosis of muscular dystrophy, such as Duchenne muscular dystrophy (DMD), myopathy, malignant hyperthermia, or in patients with a genetic disorder consisting of the presence of an atypical gene encoding plasma cholinesterase (homo- and heterozygotes). If rapid intubation is necessary in this age group, the following regimen can be used: propofol (2–3 mg kg–1 b.w.)/fentanyl (1–2 μg kg–1 b.w.)/rocuronium (1.2 mg kg–1 b.w.), with the possibility of reversing the neuromuscular blockade with sugammadex (according to the SPC: 2–4 mg kg–1 b.w., depending on the type of preparation, although this dose is usually not sufficient and even 16 mg kg–1 b.w. is recommended, as in adults). In patients who are overweight (BMI > 85th percentile [> 1 standard deviation (SD]) or obese (BMI > 97th percentile [> 2 SD]), it is necessary to dose the drugs based on the ideal body weight.
It is also possible to intubate a child without muscle relaxation, but always under deep sedation and with sufficient analgesia.
Choosing a muscle relaxant
In children over 2 years of age, the dose of succinylcholine is 1–1.5 mg kg–1 b.w.
An alternative to succinylcholine is rocuronium at a dose of 0.6–1.2 mg kg–1 b.w., which allows intubation after 60 seconds. A dose of 1.2 mg kg–1 b.w. of rocuronium is equivalent to a dose of 1 mg kg–1 b.w. of succinylcholine. The effect of rocuronium can be reversed with sugammadex at a dose of 2–4 mg kg–1 b.w., although if sudden reversal of the blockade is required, 16 mg kg–1 b.w. is recommended. It is also worth mentioning a drug from the benzylisoquinoline group, mivacurium, which may be particularly useful in short-term procedures when the most important is a rapid spontaneous recovery of neuromuscular conduction (Table 1). Particular caution is recommended when administering mivacurium to patients with hypersensitivity to histamine, for example, with asthma, and – as in the case of succinylcholine – to patients with atypical, genetically determined plasma cholinesterase (Table 8).
Mask ventilation
Mask ventilation is always performed using a mixture of oxygen (50–80%) and air. Ventilation with 100% oxygen is reserved for the treatment of laryngospasm and in specific situations related to the patient’s clinical condition. It is important to remember about the proper position of the mask to ensure the tightness of the system. Adequate mask ventilation should be monitored using a monitor built into the anaesthesia machine, showing respiratory pressures and carbon dioxide concentrations on capnography, and achieved tidal volumes.
TABLE 8
Non-depolarizing muscle relaxants used in children
Laryngeal mask airway
Indications for laryngeal mask airway insertion include short anaesthesia (up to 60 minutes) in children without a full stomach, directoscopy in small children, anticipated difficult intubation, and a history of stridor. Laryngeal mask airway devices can be used in children of any age, after administering propofol at a dose of up to 4–6 mg kg–1 b.w. and fentanyl at a dose of 2 μg kg–1 b.w. [10, 11]. Muscle relaxation is not necessary. The laryngeal mask airway is removed when the child breaths on its own efficiently. The size of the laryngeal mask airway is selected according to the patient’s body weight; examples of recommended sizes, which may vary by manufacturer, are given in Table 9.
Endotracheal tube selection, tube sizes
Intubation ensures a clear airway and is performed in situations where less invasive methods of maintaining a patient’s airway patency cannot be used. One of the indications for the use of endotracheal intubation is the need to perform a procedure requiring mechanical ventilation and muscle relaxation. Intubation is also used when it is necessary to put the patient on the operating table in an unusual position and when the child is at high risk of aspiration.
Currently, low-pressure cuff tubes are used in children of all age groups. Low-pressure cuffs do not damage the subglottic area of the larynx and prevent pressure sores in the airways, while ensuring an effective seal of the trachea. However, in the case of procedures in which an unnatural head position is expected (e.g., lying on the stomach during spine surgery), reinforced tubes are used.
In paediatric anaesthesia, particular care must be taken to select the correct endotracheal tube size. Using a tube that is too large can lead to laryngeal and tracheal damage. A tube that is too small increases airflow resistance and reduces lung ventilation (Table 10).
In intubation, not only is the size (diameter) of the endotracheal tube important, but also the depth to which it is inserted. The end of the tube should always be positioned above the tracheal bifurcation. Below are some practical tips to help the physician select the appropriate size of the endotracheal tube and correctly estimate the depth of tube insertion [10–12].
It is good practice to prepare several sizes of endotracheal tubes – usually three are prepared: the correct one, i.e., calculated according to age, half a size smaller, and half a size larger:
Difficult intubation
There are many obvious clinical situations in which difficulties with maintaining a patent airway and inserting an endotracheal tube can be anticipated (Table 11). Adverse events that are difficult to predict include situations with unpredictable problems during intubation in children, so it is good practice to always be prepared for such an eventuality. The procedures and requirements for the necessary equipment are regulated by the consensus statement of the Polish Society of Anaesthesiology and Intensive Therapy and the Polish Society of Neonatology [14].
Maintenance of anaesthesia
During maintenance of anaesthesia, ventilation using sevoflurane, desflurane, or isoflurane, with or without an opioid and a muscle relaxant, is recommended.
TABLE 11
Risk factors for difficult intubation in children over 3 years of age and adolescents
Inhalational anaesthetics are always administered with a mixture of oxygen and air. According to the current trend, the indications for the use of nitrous oxide in children are limited due to its impact on the greenhouse effect and negative impact on the ozone layer, although, as a good analgesic, it may be useful in procedural sedation and analgesia (PSA), especially in emergency departments [15–18].
In a child, it is possible, and in justified cases even advisable, to perform total intravenous anaesthesia (TIVA) using a continuous intravenous infusion of propofol together with an infusion of an opioid, for example, remifentanil (Table 12). There are several propofol administration regimens available, most of them validated for adults, such as the Roberts manual propofol model, which can be used in older adolescents; however, the McFarlan’s model is more optimal for children, which includes:
induction dose 2.5 mg kg–1 b.w.,
I period 15 min – 15 mg kg–1 b.w. h–1,
II period 15–30 min – 13 mg kg–1 b.w. h–1,
III period 30–60 min – 11 mg kg–1 b.w. h–1,
IV period 1–2 hours –10 mg kg–1 b.w. h–1,
V period 2–4 hours – 9 mg kg–1 b.w. h–1.
It is also possible to use the TIVA technique – target-controlled infusion (TCI) drug concentration in plasma or at the effect site. The advantage of this technique is its accuracy, which is largely determined by the fact that specially developed algorithms include factors such as age, gender, body weight, and height of the patient [19]. The optimal models for paediatric anaesthesia include the Marsch, Paedfusor, or Kataria models for propofol, and the Minto model for remifentanil (> 12 years and 30 kg body weight).
Lung ventilation during general anaesthesia
Currently, anaesthetic devices with a circular system (semi-closed method) are used in children of all age groups, taking into account the size of the interchangeable breathing system depending on the age and weight of the child being anaesthetized: a paediatric system (10–40 kg) or an adult set (> 40 kg). Regardless of the choice of ventilation mode, it is important to follow the principles of lung-protective strategy of the mechanical ventilation, i.e., tidal volume (TV) of 6–8 mL kg–1 b.w., plateau pressure below 30 cmH2O, and the use of positive end-expiratory pressure (PEEP).
In patients over 3 years of age, both pressure-controlled ventilation (PCV) and volume-controlled ventilation (VCV) can be used during anaesthesia, with end-expiratory pressure typically set at 3–5 cmH2O. In children over 3 years of age, low-flow anaesthesia (LFA) or minimal-flow anaesthesia (MFA) can be used. However, it should be noted that in these techniques, the flow of the respiratory mixture is lower than the flow in minute ventilation; rebreathing requires careful control of carbon dioxide (CO2) elimination and frequent replacement of calcium in the CO2 absorber, as well as continuous monitoring of the oxygen concentration in the end-tidal mixture; in return, it guarantees less heat loss. Due to the risk of increased carbon monoxide (CO) and carboxyhemoglobin (COHb) concentrations, the LFA technique is recommended for children over 2 years of age and weighing more than 20 kg [20, 21].
Anaesthesia in a child with a full stomach
Anaesthesia in a child with a full stomach increases the risk of complications due to the risk of aspiration of stomach contents into the respiratory tract.
Conditions associated with the risk of aspiration and a full stomach are presented in Table 13.
Currently, it is recommended, whenever possible, to perform an ultrasound assessment of gastric contents [22].
If a child is qualified to general anaesthesia with a full stomach, intravenous access should always be obtained before induction, and if this is not possible, intraosseous access should be obtained. This makes it possible to perform the controlled rapid sequence induction of anaesthesia (cRSI), which is the safest in this situation. Traditional “rapid induction” involving passive pre-oxygenation, followed by rapid administration of a sedative and succinylcholine chloride, as the fastest and shortest acting muscle relaxant, and then intubation without mask ventilation, is not recommended in children [23].
Passive pre-oxygenation may be ineffective in the case of a distressed child, and ventilation with low pressures and tidal volumes does not increase the risk of aspiration; therefore, oxygenation of the child is often started only after the administration of drugs [24]. The child should be ventilated through a face mask, with a peak inspiratory pressure (PIP) of no more than 15 mmHg and a fraction of inspired oxygen (FiO2) of 0.8. Ventilation before intubation is necessary because children have a higher metabolism and a higher oxygen demand, but also a lower functional residual capacity (FRC), so their tolerance of obstructive sleep apnea syndrome (OSAS) is significantly lower.
In this cases, the anaesthetic for a haemodynamically stable child is propofol, and for a patient in shock, ketamine. Sometimes these drugs are combined. An opioid, most commonly fentanyl, is also used, although it can cause vomiting. Rocuronium is most commonly used to provide muscle relaxation, essential for efficient and non-traumatic intubation. Its advantage, in addition to the rapid onset of action, comparable to that of succinylcholine chloride, is the possibility of immediate reversal of its effect with sugammadex. An alternative is the administration of chlorsuccinylcholine, especially in patients with obesity or when sugammadex is not available. The equivalent doses of these drugs are 1.2 mg kg–1 b.w. for rocuronium, 16 mg kg–1 b.w. for sugammadex, and 1–2 mg kg–1 b.w. for succinylcholine, respectively.
Cricoid pressure is not recommended; this manoeuvre (Sellick manoeuvre) has not been proven to be effective in preventing regurgitation, but it often causes problems with ventilation or intubation, as well as vomiting if pressure is applied too early.
There is no clear indication of when a gastric tube should be inserted, or whether, if one is already in place, it should be left during induction or removed (after prior suctioning of the gastric contents). Therefore, the decision in this matter depends on the anaesthesiologist’s experience. In every case, the induction of a child on a full stomach should be performed by an experienced anaesthesiologist or at least such a specialist should be present in the operating room, ready to provide immediate assistance if needed (Table 13).
TABLE 13
Conditions associated with aspiration risk and a full stomach
In the past, it was recommended to use uncuffed endotracheal tubes until approximately 7 years of age, i.e. until the narrowest point of the larynx is the physiological subglottic stenosis. Currently available microcuff endotracheal tubes enable cuffed tube intubation even in full-term newborns (although uncuffed tubes are still often used in this age group). It is important to remember that for a cuffed tube, we should choose a size half the size of the intended uncuffed tube. Using cuffed tubes reduces the need for reintubation, which increases the safety of anaesthesia in children with a full stomach.
Postoperative pain management
Postoperative pain management is one of the fundamental elements of ERAS and therefore requires the development of a strategic plan throughout the perioperative period. The general principles and recommendations do not differ from the standard accepted and applicable principles described in the consensus statement paper regarding children under 3 years of age. However, drugs that are not recommended in the SPC for newborns, infants, or younger children can be used in older children and adolescents.
The dosage of analgesics is described in Tables 14–19.
TABLE 14
Dosage of opioid drugs
TABLE 15
Patient-controlled analgesia
TABLE 16
Paracetamol dosage in children and adolescents with particular emphasis on age differences
TABLE 17
Metamizole dosage in children and adolescents, with particular emphasis on age differences
TABLE 18
Dosage of nonsteroidal anti-inflammatory drugs (NSAIDs) in children and adolescents
ANAESTHESIA IN CHILDREN OVER 3 YEARS OF AGE IN SPECIALIZED MEDICAL FIELDS
Anaesthesia in dentistry
Dental procedures under anaesthesia typically involve uncooperative children – both healthy individuals whose dental phobia, anxiety, and emotional instability prevent treatment, and those with comorbidities, communication difficulties, intellectual disabilities, or various forms of neurodivergence (e.g., autism, cerebral palsy, Down syndrome, etc.). Adequate sedation or general anaesthesia is intended to ensure complete comfort and safety for such patients, while also facilitating the dentist’s precise execution of the procedure.
A sedation method sometimes used in dental offices is minimal sedation (according to the ASA classification), which does not require the presence of an anaesthesiologist. In such cases, inhaled nitrous oxide or oral sedative medications (hydroxyzine, midazolam, etc.) are used for short-term procedures. This form of sedation usually requires the support of local anaesthesia. During such a procedure, the patient should respond to the doctor’s verbal commands, open the oral cavity independently, and maintain protective reflexes from the larynx in response to the water cooling the dental turbines, flowing saliva, or blood [25].
Unfortunately, this type of procedure will not work in paediatric patients whose level of anxiety or intellectual disability effectively precludes any co operation. Therefore, the vast majority of dental procedures in children should be performed by a qualified anaesthesiology team (a specialist in anaesthesiology and intensive therapy, and an anaesthesiology nurse) using general anaesthesia, in a setting that meets basic anaesthesia standards.
It is also important that general anaesthesia allows for comprehensive dental treatment in just a single visit [25–27].
Preparation for anaesthesia
The assessment of a patient qualified for general anaesthesia, moderate and deep sedation should be performed by an anaesthesiologist in accordance with the standards of preoperative assessment. In the case of healthy children, blood count and an activated partial thromboplastin time (aPTT) tests are required (especially in children undergoing tooth extraction and/or oral cavity sanitation procedures, and in those with a history of complications). In children with comorbidities, it may be necessary to perform additional tests or specialist consultations. Patients with concomitant diseases should have an anaesthetic consultation well in advance of the day of the procedure, as this allows for the selection of the optimal procedure (Table 20). During the examination, special attention should be paid to any loose teeth, and the airway should be assessed to ensure it remains clear during the procedure, especially since a fundamental feature of dental surgery is “sharing the airway” with the dentist and/or oral surgeon. It is also necessary to follow a strict dietary regimen according to the 1–3–4–6 rule [4].
Premedication
Midazolam is primarily used in pharmacological premedication; it can be administered orally or rectally 20–30 minutes before the planned procedure or administered intranasally (0.2–0.6 mg kg–1 b.w.) 10 minutes before the start of anaesthesia. Recently, dexmedetomidine has been increasingly used in clinical practice and may also prove useful in the premedication phase, especially in hyperactive children; it can be used intranasally at a dose of 1–2 μg kg–1 b.w. or orally at a dose of 1–4 μg kg–1 b.w. (off-label). In children with congenital heart defects, oral ketamine is a good option, providing relative cardiovascular stability and minimal impact on the respiratory system.
TABLE 19
Recommended doses of local anaesthetics for the most frequently performed peripheral blocks in children and adolescents using ultrasound imaging
TABLE 20
Neurodevelopmental disorders/comorbidities and their impact on preparation for surgery
In some patients, especially those with behavioral disorders such as aggression, in whom premedication may be difficult to administer, or in children with autism, in whom the effect may be unpredictable, non-pharmacological premedication methods play an auxiliary role. These may include various distraction techniques, such as video games, movies, personal toys, or simply the presence of a parent [27, 28].
Anaesthesia
Induction of anaesthesia is typically initiated by inhalation using sevoflurane. Alternatively, if intravenous access is available, propofol remains the drug of choice. In children with cyanotic heart defects, ketamine is the preferred induction agent. Anaesthetics are combined with small doses of opioids – fentanyl or remifentanil. Due to the high risk of aspiration during the procedure and the patient’s shared airway with another operator, the principle of instrumental airway protection applies in dentistry/oral surgery. The decision regarding the type of airway management technique is made taking into account the scope of dental procedures, the expected duration of the procedure, and the patient’s respiratory risk. In cases of long-term and more complex procedures, endotracheal intubation is the treatment of choice, whereas during short-term procedures (< 45 minutes) involving single teeth, especially in the upper jaw, a laryngeal mask airway can be used. Endotracheal intubation is preceded by the administration of a short- or medium-acting muscle relaxant, depending on the type of procedure or the anaesthesiologist’s preference. The use of a muscle relaxant can be omitted provided that the induction of anaesthesia is sufficiently deep to ensure a smooth intubation. Some anaesthesiologists prefer nasal endotracheal intubation, but minimal trauma remains the priority. The nasal/ nasopharyngeal mucosa is highly vascularized and quite often responds to any injury with profuse bleeding, requiring additional vasoconstrictor therapy (nasal drops should be administered 15–20 minutes before intubation – xylometazoline 0.05% in infants and young children, 0.1% in older children). Nasal intubation is not recommended for children with suspected third adenoid hypertrophy, recurrent inflammation of the nasal mucosa, a deviated nasal septum, or a cleft palate. Endotracheal intubation through the mouth does not hinder the performance of the dental procedure; it only requires cooperation with the operator and, if necessary, moving the tube from one corner of the mouth to the other during the procedure. In dental surgery, tubes with a sealing cuff are preferred, and it is also advisable to pack the area around the laryngeal entrance with a moist seton. This prevents blood, secretions, and any other contaminants from leaking into the trachea. It is common practice in oral surgery to use regional analgesia before extractions, root canal treatment, or other more painful procedures. Concomitant administration of a local anaesthetic drugs reduces the need for intravenous opioids.
Since most dental procedures are performed on an outpatient basis, it is important to ensure that the patient is given anaesthesia on time, allowing for rapid recovery and relatively quick readiness for discharge home.
For maintenance of anaesthesia, TIVA with propofol is preferred. Ketamine or dexmedetomidine can also be used for specific indications. The latter is particularly beneficial in reducing post-anaesthetic anxiety. When using dexmedetomidine, one should always remember the risk of bradycardia, which is further increased by the occurrence of a reflex from the trigeminal nerve stimulated during dental work.
Typically, high doses of opioids are not necessary for maintaining anaesthesia. Sevoflurane can be used for maintenance of anaesthesia, but it should be remembered that it is a common cause of EA or delirium during awakening, especially in young children [26, 27].
Anaesthesia recovery period
Before waking up, the child must first be provided with pain relief. Most dental procedures do not carry the risk of severe postoperative pain; therefore, non-opioid drugs (paracetamol, metamizole) and non-steroidal anti-inflammatory drugs (NSAIDs) (ibuprofen) are sufficiently effective. Antiemetic prophylaxis (ondansetron and/or dexamethasone) is also recommended. Before waking up, the sealing seton must be removed from the oral cavity; it is also necessary to thoroughly clean the oral cavity and throat from any remaining contents, dental rolls, or teeth, and in the case of their extraction, special attention should be paid to maintaining hemostasis. It is preferable to extubate the patient in the lateral position and avoid excessive coughing.
Patients can be discharged home after the procedure if they meet the appropriate criteria: they are conscious, establish proper contact (adequate to the state before anaesthesia), with stable respiratory and circulatory system, they do not experience nausea and vomiting, and do not report any pain [27, 28].
Anaesthesia in otolaryngology
ENT procedures are the most commonly performed surgical procedures in children. They range from simple, one-day surgeries, such as myringotomy, to complex airway reconstructions performed in specialized centres [3]. Preoperative assessment in this group of patients serves to identify, apart from comorbidities, specific risk factors for perioperative complications, such as respiratory tract infection in the last 2 weeks, respiratory diseases such as asthma, snoring, airway obstruction (tonsillar hypertrophy), age below 3 years, passive smoking, obesity, craniofacial defects or neuromuscular diseases, and to implement appropriate preventive measures [29].
Preparation for anaesthesia
From the anaesthesiologist’s point of view, there is no need to perform additional tests for typical procedures such as adenoidectomy, adenotonsillotomy or adenotonsillectomy in children in good general condition and with no history of bleeding incidents [29]. However, in practice and after consultation with an otolaryngologist, it is worth assessing the blood count, aPTT or C-reactive protein concentration, especially in children with frequent and recurrent respiratory tract infections. Coagulation testing may be necessary if there is a history of bleeding (nose, gums, ear, etc.). Blood typing may be useful prior to tonsillotomy or tonsillectomy due to the higher risk of intraoperative and postoperative bleeding. It is important to determine if the child has symptoms of OSAS. These patients are at increased risk of desaturation, laryngospasm, and airway obstruction during induction of anaesthesia. They are also characterized by increased sensitivity to the effects of opioids and sedatives, and a reduced response to increased CO2 concentrations. These patients may also have circulatory system disorders (arterial hypertension, sometimes pulmonary hypertension) requiring additional cardiovascular examination [29]. In a child with suspected and/or diagnosed foreign body aspiration, an X-ray examination must be performed.
Premedication
In children in good general condition, the drug can be administered orally – mainly midazolam at a dose of 0.3–0.5 mg kg–1 b.w., 20–30 minutes before anaesthesia. Dexmedetomidine can also be administered intranasally at a dose of 1 μg kg–1 b.w., 60 minutes before induction of anaesthesia [30].
In patients with OSAS, it is best to avoid premedication with sedative medications. In cooperative children and/or those with previously established intravenous access, premedication may be omitted.
Induction of anaesthesia
Before intubation, it is beneficial to administer dexamethasone (0.1−0.15 mg kg–1 b.w., max. 4 mg), mainly to reduce the risk of postoperative nausea and vomiting (PONV), but also to reduce the need for non-opioid analgesics in the postoperative period [31]. In the case of surgeries with a high risk of PONV, intravenous administration of ondansetron at a dose of 0.10–0.15 mg kg–1 b.w. or TIVA may be beneficial. In children in good general condition, the following induction may be used:
inhalational (in the absence of intravenous access) – sevoflurane in a mixture of oxygen and air. In children with OSAS, this route of induction is preferred, and it is also beneficial to maintain continuous positive airway pressure (CPAP) to prevent upper airway obstruction,
intravenous – propofol, thiopental or ketamine – the latter especially in children with unstable circulatory system, with accompanying bleeding or when it is necessary to maintain spontaneous breathing.
Most procedures require endotracheal intubation preceded by the administration of a short- or medium-acting muscle relaxant (mivacurium, rocuronium or atracurium), depending on the type of procedure or the anaesthesiologist’s choice. For procedures such as adenotonsillectomy, it is advisable to use a tube with a sealing cuff or to seal the area around the laryngeal entrance with a moist bandage, as well as to use tubes with a facially adapted curvature (RAE – right-angle endotracheal) or reinforced tubes. The sealing cuff prevents blood from entering the trachea from the surgical site, and the use of appropriate endotracheal tubes prevents them from kinking.
Maintenance of anaesthesia
For maintenance of anaesthesia, combined general endotracheal anaesthesia is preferred. TIVA with propofol and remifentanil can also be used, especially in older children, for middle ear, nasal septum, or sinus surgery (functional endoscopic sinus surgery, FESS) or in patients at high risk of PONV. The method of choice when inhalation medications are contraindicated is TIVA. For short procedures (e.g., tympanic membrane incision), VIMA is usually sufficient. It should also be remembered that anaesthetics for ENT procedures are associated with an increased risk of ED, especially in the age group of 2–5 years [32].
Optimal intraoperative analgesia is usually easily achieved with synthetic opioids – fentanyl (1–3 μg kg–1 b.w.) or sufentanil (0.1–0.3 μg kg–1 b.w.). Long- acting opioids should be avoided in patients with OSAS. Remifentanil (0.1–0.5 μg kg–1 b.w. min–1) may also be used as an analgesic, administered by infusion, with or without an initial bolus dose (risk of bradycardia, drop in blood pressure, and chest stiffness). Opioid analgesia is supplemented with ibuprofen (intravenously 10 mg kg–1 b.w. in children > 6 years of age) and/or paracetamol (intravenously 15 mg kg–1 b.w.) or metamizole (intravenously 15 mg kg–1 b.w.), preferably in advance. Following pharyngeal surgery, waking in the lateral position is preferred, with minimal catheter irritation (no-touch technique), which reduces the risk of laryngeal spasm. Additionally, intravenous lidocaine at a dose of 1 mg kg–1 b.w. may be administered prior to extubation. After the procedure, nalbuphine at a dose of 0.1–0.2 mg kg–1 b.w., paracetamol, and optionally metamizole are recommended to reduce pain. Special situations include removal of a foreign body from the trachea or bronchi, and repeat adenotonsillectomy due to bleeding. In the former case, it is recommended to use a ventilation bronchoscope inserted into the airway after induction of anaesthesia (using any method). For maintenance, a combined intravenous-inhalation method is preferred. In the event of bleeding following adenotonsillotomy, the patient should be treated as if in shock and with a “full stomach”. Intravenous infusion (propofol, ketamine) using the cRSI method is recommended.
Anaesthesia in orthopedics
Procedures performed in paediatric orthopedics include the treatment of congenital defects, developmental defects, injuries, and tumors of the musculoskeletal system.
A key aspect of obtaining informed consent from the patient and parents/guardians is providing reliable information about anaesthesia and surgical procedures. Patient education is consistent with the ERAS protocol. It can be adapted to the specific needs of paediatric orthopedics, given its collaborative nature with the child and parent. The benefits of the ERAS protocol are particularly noticeable in long-term surgeries involving high blood loss. It has been proven that the use of protocolised care improves postoperative outcomes, shortens hospital stay, and reduces costs [33].
Preparation for anaesthesia
Before qualifying for anaesthesia, the patient must be examined by an anaesthesiologist. The decision regarding laboratory tests should be based on a risk assessment of the planned surgical procedure and an assessment of the child’s general condition and comorbidities. The scope of testing is consistent with generally accepted guidelines [34, 35]. Orthopaedic procedures that involve the risk of significant blood loss and a long duration of the operation include spinal corrections, pelvic and femoral osteotomy, and oncological procedures. Blood type, complete blood count, serum electrolyte concentration, and coagulation testing are necessary. Procedures that require echocardiography and spirometry include corrections of defects of the spine and anterior chest wall. In these cases, advanced monitoring should be used: invasive blood pressure measurement with assessment of haemodynamic parameters, monitoring of the depth of anaesthesia, diuresis, core temperature, and assessment of the degree of relaxation.
Elective paediatric orthopaedic procedures can be properly systematized by analyzing the risk of postoperative complications resulting from blood loss, long duration of the procedure, or damage to nearby important structures (Table 21).
Low-risk procedures most commonly performed on children under 3 years of age include foot correction. In the age group over 3 years of age, high-risk procedures include:
large bony outgrowths,
pelvic and femoral osteotomy,
simple (open) reduction of the hip joint,
treatment of early childhood scoliosis.
The main reasons for emergency surgery are open fractures and fractures with neurovascular injury. Other types of fractures, as well as ligamentous and capsular injuries, are treated on an expedited basis [36].
TABLE 21
Division of orthopaedic procedures according to the perioperative risk
High-risk procedures are most often performed in specialized departments of paediatric orthopaedics. Contracted procedures exclusively for these departments include PZH03 – comprehensive pelvic and lower limb procedures for patients under 18 years of age (e.g., pelvic osteotomy, comprehensive foot reconstructions) and PZH08 – comprehensive corrective spine procedures for patients under 18 years of age (e.g., scoliosis, Scheuermann’s disease – juvenile thoracic kyphosis, congenital spine defects). Other types of surgeries can be performed within the pediatric surgery department or the orthopedics and traumatology department.
Anaesthesia
The commonly recommended and preferred method of anaesthesia is general anaesthesia combined with regional analgesia. Although central blocks in sedation are not always readily chosen by patients and their caregivers, there is a clear positive trend towards an increase in their use due to the benefits of regional analgesia.
For longer-term operations, it is worth considering the use of TCI. Propofol infusions using this technique are particularly useful in paediatric scoliosis surgery, where spinal cord protection and the ability to precisely monitor neural function via intraoperative motor evoked potentials (MEPs) are key priorities. Compared to traditional dosing models, the TCI technique allows for a reduced total propofol dose, which is important in the paediatric population due to the larger volume of distribution and faster metabolism in children. Precise dosing helps reduce undesirable effects such as circulatory depression or prolonged recovery time. In addition, TCI provides greater control over propofol plasma concentration, which reduces the risk of intraoperative awakening by reducing the likelihood of bispectral index (BIS) values exceeding 60. TCI makes this method more effective and safe, as it supports the rapid awakening of the patient after the completion of surgery, which is particularly important in the context of rapid assessment of neurological function.
Interdisciplinary, protocolised perioperative care provided by a permanent team (doctors, nurses, physical therapist, dietitian, psychologist) is particularly important in the case of spinal surgery. The use of the ERAS protocol has been shown to be particularly beneficial in this group of patients, including reduced complications, shorter hospital stays, and improved patient comfort [37]. The use of an anaesthetic protocol for spinal surgery in children increases the safety of the procedure. Routine use of intraoperative neuromonitoring requires the anaesthesiologist to be familiar with the effects of drugs and parameters on the nervous system and neuromuscular transmission. Table 22 presents the type of impact of the most commonly used drugs on somatosensory evoked potentials (SEP) [38]. For this reason, many centres use dexmedetomidine instead of midazolam for premedication before scoliosis correction procedures.
TABLE 22
Effects of drugs and other factors on sensory and motor evoked potentials
Pain management
Orthopaedic surgeries cause acute pain of moderate to severe intensity, lasting from several days to several weeks. The risk of chronic postsurgical pain (CPSP) may reach 30% in the cases of thoracoscopic correction of anterior chest wall deformities and 10–40% in the case of correction of spine defects [39]. Therefore, the pain management plan should be based on the principles of multimodal analgesia using analgesics, co-analgesics, regional analgesia techniques, and alternative methods (e.g., cryoanalgesia). For most procedures with low and moderate risk, paracetamol, metamizole, and NSAIDs should be used at regular intervals, in doses appropriate to age and body weight, along with opioids and local anesthetics for regional blocks. In the case of the most painful procedures, i.e., osteotomy, correction of spine and chest wall defects, additional analgesic doses of ketamine, α2-adrenergic agonists, and co-analgesics (magnesium sulfate, steroids) should be used, as well as a continuous intravenous opioid infusion in the postoperative period, in older children using patient-controlled analgesia (PCA) [40]. A beneficial effect of intravenous lidocaine infusion has been proven in the surgical correction of anterior chest wall deformities and spine defects. An appropriate time interval must be maintained in accordance with applicable rules if a regional block with a long-acting anaesthetic has been used before surgery.
The principles of pain management include preemptive analgesia, protective analgesia, and preventive analgesia (extending protective anal-gesia with drugs that prevent hyperalgesia and central sensitization, such as α2-adrenergic receptor agonists, ketamine, lidocaine, and gabapentin) [41–45]. In children, regional anaesthesia should be performed under general anaesthesia or deep sedation, which may mask the neurological complications of the blockade. The techniques used for regional anaesthesia are the same as in the adult population and include central blocks, anaesthesia of peripheral nerves before the procedure, or infiltration of the surgical site with a long-acting local anaesthetic. To improve quality and safety, regional blocks should be performed under ultra-sound guidance. Regional anaesthesia should be used whenever possible, as it significantly reduces the need for opioid drugs in the postoperative period and controls pain to a degree acceptable to the patient. It also enables functional recovery in terms of cooperation, early rehabilitation, meal tolerance, full function of the digestive and excretory systems, and proper sleep cycles, as well as effective postoperative pain relief. Important factors that facilitate pain control include managing stress and separation anxiety and reducing the risk of procedural pain.
Anaesthesia in ophthalmology
Ophthalmic surgeries and diagnostic or therapeutic procedures are performed in children of all ages, most often under general or combined anaesthesia (general anaesthesia combined with regional block or local anaesthesia with drops) [46, 47].
Children undergoing ophthalmic surgery are usually healthy (ASA I or II). However, eye diseases can sometimes be accompanied by congenital diseases or syndromes, including heart defects, difficult airways, or metabolic disorders. Identification of hazards and appropriate preparation (including video laryngoscopy, endocarditis prophylaxis in patients with heart defects) will increase the child’s safety in the perioperative period.
Pathophysiology
The scope of knowledge and skills of an anaesthesiologist who undertakes anaesthesia of a child for ophthalmic procedures must include the following issues: anatomy of the eyeball and orbit, physiological conditions of intraocular pressure (IOP), the effect of drugs used during anaesthesia on IOP, the mechanism of development of ocular reflexes, and the physiological effect of intraoperative surgical manipulations.
Intraocular pressure
IOP is the result of the balance between the production and drainage of aqueous humor in the eyeball. There are many factors that influence this value (Tables 23 and 24).
If intraocular hypertension is confirmed, appropriate treatment should be implemented (Table 25).
Drugs used during anaesthesia for ophthalmic surgery may cause an increase or decrease in IOP and thus affect the measurements performed (Table 26).
TABLE 24
Factors influencing intraocular pressure (IOP)
Ocular reflexes
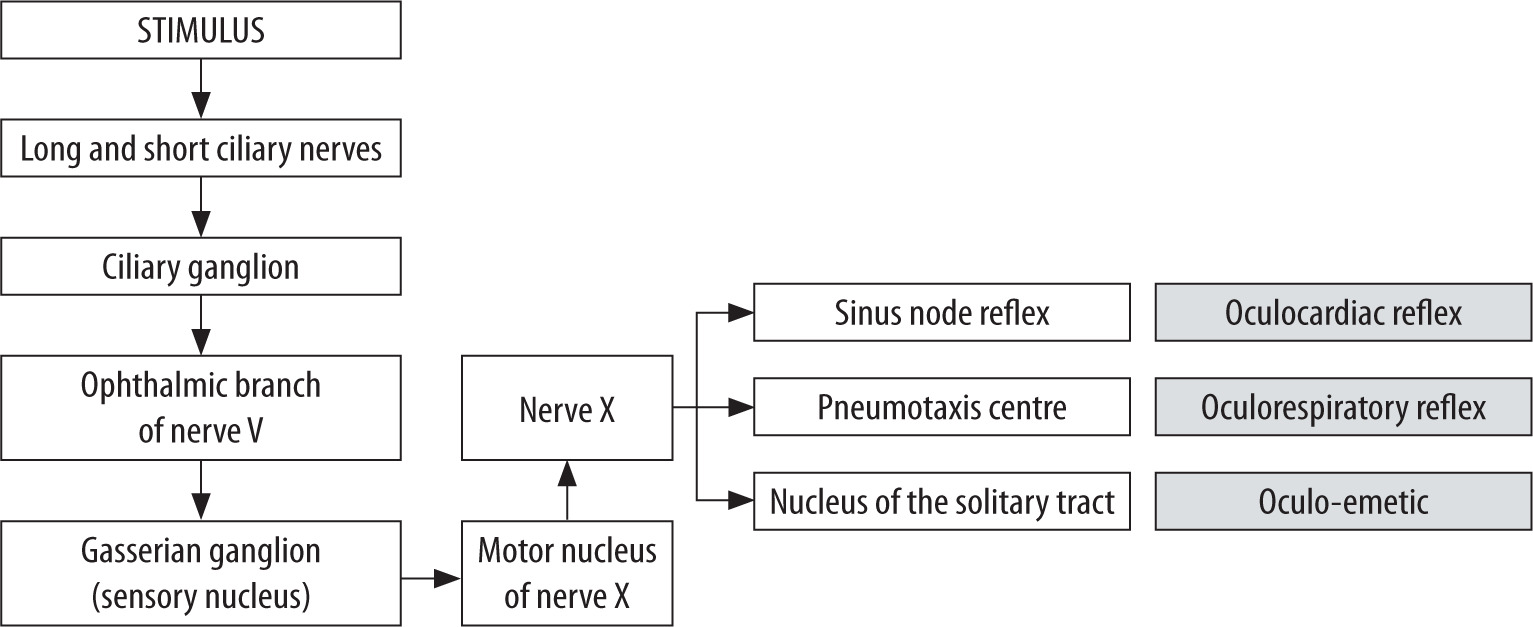
Oculocardiac reflex: Repeated traction of extra-ocular muscles during surgery (strabismus surgery, vitreoretinal surgery, enucleation, banding), regional blocks, and ocular compressions can cause reflex cardiac arrhythmia (bradycardia, ventricular extra-systole, sinus arrest, ventricular fibrillation) (Figure 1).
The risk of cardiac arrhythmia increases with the coexistence of hypercapnia and high concentrations of inhaled anaesthetics.
Prophylactic use of anticholinergic drugs does not prevent the occurrence of arrhythmia. A syringe with atropine or glycopyrronium solution must be kept ready for use at the anaesthesia station in case of bradycardia.
Oculorespiratory reflex: This reflex occurs during strabismus surgery. The afferent limb of the reflex is the same as the oculocardiac reflex, originating in the pneumotaxis centre in the pons, and leading to shallow breathing, acceleration, slowing, or even cessation of breathing. Atropine does not prevent this reflex.
Oculo-emetic reflex: The oculo-emetic reflex occurs most frequently during strabismus surgery and is a consequence of stimulation of the vagus nerve when the operator pulls the extraocular muscles.
Eye medications taken by the patient
Many children undergoing eye surgery take eye drops [48]. These drops may flow into the throat or through the nasolacrimal ducts into the nasal cavity, be absorbed through the mucosa into the systemic circulation, and cause undesirable effects (tachycardia, hypertension, bradycardia, or bronchospasm) (Table 27).
TABLE 25
Management of increased intraocular pressure during surgery
TABLE 26
Effect of anaesthetic drugs on intraocular pressure (IOP)
Regional blocks for ophthalmic surgery
For safety reasons, peribulbar and retrobulbar blocks are rarely performed in children [49]. The eyeball in children occupies more than twice the orbital space of the eyeball in adults. However, subcapsular blocks (sub-Tenon’s block) are performed. This is typically done by the surgeon to block the ciliary nerves (short and long ones). This block ensures ocular im-mobility during surgery, provides good analgesia, prevents the oculocardiac reflex, and reduces the risk of postoperative nausea and vomiting. A small volume of local anaesthetic is used for the block to avoid pressure on the eyeball and an increase in IOP; 1% or 2% lidocaine or 0.5% bupivacaine is used in volumes of 1.5–2 mL in children 5–10 years of age and 2–3 mL in older children, respectively.
TABLE 27
Ophthalmic medications taken by the patient
Local anaesthetics are also administered directly into the conjunctival sac in the form of drops. This provides effective, inexpensive analgesia without the complications associated with puncture with a curved needle.
Anaesthesia for emergency ophthalmic surgery
Penetrating ocular injuries and the presence of a foreign body require urgent treatment. If the prescribed waiting period after a meal cannot be maintained, the trachea must be intubated as part of the cRSI procedure. The induction and relaxation of the muscles must be sufficiently deep to prevent pressure build-up and leakage of the contents of the eyeball through the holes created by the injury, as this may result in complete loss of vision. Succinylcholine chloride has long been recommended to be avoided because it causes a transient, significant increase in IOP and the need for intubation after administration of a high dose of a non-depolarizing muscle relaxant. In fact, there are no well-documented reports describing vitreous leakage after succinylcholine chloride administration, and the risks and benefits of its use should always be considered [50, 51]. Underestimated level of induction may trigger a cough reflex, which also causes an increase in intraocular pressure.
Anaesthesia for ophthalmological examination and measurement of intraocular pressure
In children undergoing ophthalmological treatment, IOP measurements and ophthalmological examinations are typically performed repeatedly and regularly. Children rarely cooperate during the examination, and suboptimal conditions prolong the examination and perpetuate the associated stress.
During general anaesthesia, a proper airway can be maintained using a face mask or supraglottic devices. The ophthalmologist measures IOP after inhalation induction before inserting the supraglottic device to minimize the effect of anaesthesia on the measured pressure.
Anaesthesia for glaucoma surgery
The cause of glaucoma in children is impaired drainage of aqueous humor from the anterior chamber of the eye. This is most often a congenital defect involving underdevelopment of the trabecular meshwork. Untreated intraocular hypertension can lead to vision loss. Pharmacotherapy (timolol drops) is usually insufficient. The patient may breathe spontaneously during the procedure (goniotomy, trabeculectomy, trabeculotomy), but the operator usually prefers to keep the eye not moving. Remifentanil infusion provides adequate analgesia and helps avoid the use of muscle relaxants.
Anaesthesia for cataract surgery
Cataract in children can be congenital or acquired (post-traumatic or secondary to infection). Surgical treatment of congenital cataract (aspiration or removal of the lens) is performed in the neonatal period (6–8 weeks of age – vision-saving surgery). The requirement is to ensure immobilization of the eyeball during surgery and to avoid an increase in IOP during the waking phase.
Anaesthesia for strabismus surgery
During strabismus surgery, the oculocardiac reflex and PONV are relatively common. According to the 2016 British recommendations, the patient should receive two antiemetic drugs (ondansetron and dexamethasone) intraoperatively [52]. The anaes thetic and strabismus surgery plan should include rescue therapy. In Poland, this may involve a subcapsular block performed by an ophthalmologist at the beginning or end of the procedure. Dehydrobenzperidol, used in rescue therapy, is still unavailable in Poland. Since 2019, the drug has been approved for use on the US market by the Food and Drug Administration (FDA) under the name Inapsine, but it is not possible to order it as a direct import. Effective postoperative analgesia is provided by NSAIDs, paracetamol, metamizole, and eye drops containing a local anaesthetic (0.5% tetracaine or 0.4% oxybuprocaine). Ocular myopathies rarely lead to malignant hyperthermia, but it is recommended to avoid succinylcholine, monitor exhaled CO2, and measure temperature during anaesthesia.
Anaesthesia for vitreoretinal surgery
Retinal detachment can be limited ot multi-site, and most often occurs following trauma. It can also occur in congenital conditions (e.g., Marfan syndrome, Sticler syndrome, Knobloch syndrome, and others). Cryotherapy and laser photocoagulation are the treatment of choice for minor detachment and telangiectasia (Coats disease). To treat larger detachments, silicone oil or absorbable gas is injected into the eyeball, a scleral brace is used, or the eyeball is ringed. Procedures are performed on a stationary eyeball. Intraoperatively, opioid analgesia or preoperative subcapsular block is required. If gas such as air, sulfur hexafluoride (SF6), or octafluoropropane (C3F8) is administered into the eyeball, the use of nitrous oxide should be avoided during anaesthesia and for the following 12 weeks or until the gas is completely absorbed.
Anaesthesia for the treatment of retinopathy in premature infants
Abnormal retinal vascular growth can lead to retinal detachment, blurred vision, amblyopia, and vision loss. Early stages of the disease are treated with laser photocoagulation, while stages IV and V require vitreoretinal surgery. Premature infants may suffer from numerous comorbidities (heart defects, bronchopulmonary dysplasia, intraventricular haemorrhage, periodic bradyarrhythmia, anaemia, necrotizing enterocolitis). In the postoperative period, premature infants are more likely to experience hypothermia, bradyarrhythmia, and apnea than full-term infants.
General anaesthesia with endotracheal intubation is preferred, as postoperative ventilation may be necessary. However, depending on the severity of the disease, procedures under intravenous or inhalation anaesthesia have been described, performed without intubation, with or without supraglottic devices, in combination with subcapsular block or local anaesthesia. Laser photocoagulation is less painful and better tolerated than cryotherapy. Both therapies may cause cardiorespiratory instability in the child; therefore, both procedures and intravitreal injections (antibody against vascular endothelial growth factor) are performed under combined anaesthesia (general, combined with regional).
Anaesthesia in patients with retinoblastoma
Retinoblastoma is the most common eye cancer in children. In young children up to 3 years of age, an ophthalmological examination under anaesthesia is performed every 4–8 weeks.
Depending on the stage of the disease, small tumors are treated with laser photocoagulation, cryotherapy, or epidural brachytherapy under general anaesthesia. For larger tumors, the treatment of choice is intravitreal chemotherapy or selective intra-arterial chemotherapy. Intra-arterial administration of the drug requires precautionary heparin coverage (75 μg kg–1 b.w.). The procedure is performed under general anaesthesia with intubation and muscle relaxation. After the procedure, the patient has a pressure dressing applied to the cannulated artery. Coughing and increased IOP should be avoided upon awakening. Melphalan causes ocular swelling and postoperative vomiting; therefore, every patient should be treated with dual PONV prophylaxis.
Anaesthesia to unblock the nasolacrimal ducts
Nasolacrimal duct unblocking is a short procedure performed under general anaesthesia, using a laryngeal mask airway and suction (0.9% NaCl or fluorescein may flow into the nasopharynx). Open classical and endoscopic dacrocystorhinostomy are more painful procedures and require the use of short-acting opioids, intubation with a profiled or reinforced tube, and pharyngeal setonization. Mucosal bleeding can usually be controlled with vasoconstrictor eye drops (lidocaine with phenylephrine).
ANAESTHESIA FOR DIAGNOSTIC PROCEDURES – MAGNETIC RESONANCE IMAGING, COMPUTED TOMOGRAPHY, GASTROINTESTINAL ENDOSCOPIC PROCEDURES
Anaesthesia for diagnostic tests and procedures is usually performed outside the operating theatre in a CT, MRI, or endoscopy room. The main goals of anaesthetic activities in this case include reducing or eliminating the child’s anxiety and fear, eliminating pain if a given procedure is painful, and eliminating the child’s motor activity to enable the examination to be performed safely, minimizing psychological trauma, and increasing the so-called amnestic potential. Diagnostic and endoscopic procedures are usually performed as day cases, and anaesthesia must be administered safely so that the patient can quickly regain consciousness and be discharged home or to their primary care unit.
The organisation and equipment of the anaesthesia station located in each of the above-mentioned diagnostic laboratories are regulated by the same regulations as apply to stations located within the operating theatre. The same requirements apply to the availability of all medications used in emergency situations. For anaesthetic procedures performed in diagnostic laboratories, it is also necessary to provide children with a competent and adequately monitored position in the post-anaesthesia monitoring room.
ANAESTHESIA OUTSIDE THE OPERATING ROOM – CT SCAN ROOM, MRI ROOM, ENDOSCOPY ROOM
CT scan room and MRI room
In both the CT and MRI rooms, the anaesthesiologist administering and supervising the anaesthesia is located at a considerable distance from the child being anaesthetized, which means that the child is out of direct supervision and control. This makes it even more necessary to have very good quality monitoring equipment ensuring continuous monitoring of basic vital parameters, including capnometry measurement in an anaesthetized child with preserved spontaneous breathing [53].
It should be emphasized that in the case of an anaesthesia station located in the MRI room, all equipment must be adapted to work in a strong electromagnetic field, which means that it cannot contain ferromagnetic elements. This applies to both the anaesthesia machine and the cardiac monitor itself, as well as other equipment such as the laryngoscope, infusion pumps, and even the drip stand.
Due to the enormous noise generated by the MRI machine, the intensity of which reaches 95 dB, ear-plugs or special headphones are essential equipment, which must be used in the examined child.
Preparation for anaesthesia
No special preparation of the child for these imaging tests is required. Before the MRI examination, it is necessary to make sure that the child does not have any implants containing ferromagnetic materials (acceptable and safe: aluminum, nickel, high-quality steel, and titanium alloys), and in case of doubt, check whether the given material/implant is approved for placement in a ferromagnetic field: ventriculoperitoneal valves (yes), reinforced endotracheal tubes (no), orthopedic implants (not all).
A child with an implanted pacemaker should not be considered for an MRI scan due to the high risk of device dysfunction, including complete reprogramming. Serum creatinine levels must be measured before any contrast-enhanced examination.
Premedication
Premedication is not always necessary; if it is, the most common treatment is intravenous, oral, or intranasal midazolam. Other agents, such as dexmedetomidine or ketamine, can also be used.
Anaesthesia
The diagnostic examination is painless; therefore, in this case anaesthesia should be used to ensure the child’s comfort and minimize their anxiety and stress, as well as to ensure the patient’s immobility, as movement artifacts prevent the examination from being performed and assessed. Both inhalational (sevoflurane) and intravenous (propofol, thiopental, ketamine, dexmedetomidine) anaesthetics can be used. The lack of pain stimulation leads to discontinuation of opioids, but in some patients, they may be helpful in achieving stable anaesthesia.
A CT scan takes a very short time, usually a few minutes, and therefore requires short-term sedation while maintaining the child’s spontaneous breathing. Propofol is most often used in fractionated doses, but medications such as midazolam or ketamine may also be useful.
During an MRI examination, a much deeper and longer-lasting anaesthesia is necessary (from 20 min to even 1–2 h), which can be achieved by the TIVA method using propofol infusion at a rate adapted to the age and condition of the child (often ≥ 10 mg kg–1 b.w. h–1). Instrumental maintenance of airway patency is not necessary; however, in practice, long-term sedation and body position (the examination is performed with the patient lying on their back) predispose to limiting the airway patency. Therefore, in children with spontaneous breathing during anaesthesia, monitoring the concentration of exhaled CO2 is necessary for early diagnosis of respiratory disorders [52–54].
GASTROINTESTINAL ENDOSCOPY LABORATORY
Gastroscopy and colonoscopy are performed in children, and the number of these procedures performed in endoscopy laboratories in paediatric patients is gradually increasing. The endoscopy room where examinations are performed in children under sedation or general anaesthesia should have anaesthetic equipment ensuring safe anaesthesia, in accordance with the principles presented above [53].
The most invasive of the procedures discussed is gastroscopy. The insertion of a gastroscope is highly irritating, causing violent gag reflexes accompanied by spasm of the palate and throat muscles, coughing, and retching. Irritation of the laryngeal inlet may cause respiratory distress or reflex glottic spasm, and insertion of a gastroscope may be associated with difficulties maintaining a patent airway, further complicated by the often enlarged pharyngeal tonsils and/or palatine tonsils in these patients. However, routine endotracheal intubation for this procedure is not necessary in children unless there are additional indications, such as removal of a large foreign body, gastrointestinal bleeding, esophageal stricture, or a child with ASA score above II.
Anaesthesia
Gastroscopy under light sedation is rarely possible in children; they usually require deep sedation or general anaesthesia.
Currently, intravenous anaesthesia with propofol administered in fractionated doses or TIVA is most commonly used. To reduce the propofol dose and stabilize analgesic sedation, ketamine, dexmedetomidine, midazolam, or an opioid may be used to achieve satisfactory anaesthesia. Inhalation anaesthesia using sevoflurane can also be performed.
Colonoscopy is a procedure associated with significant discomfort and pain, but airway instrumentation is not routinely necessary. In children, the procedure is most often performed under deep sedation with the patient breathing spontaneously [55].
EMERGENCY ANAESTHESIA IN CHILDREN
Children with life-threatening conditions requiring urgent surgical intervention and anaesthesia may be taken to the hospital closest to the scene of the incident, which may not have fully equipped surgical or anaesthesiological facilities for paediatric patients.
However, every anaesthesiologist should be familiar with the basic principles of stabilization and anaesthesia for a child in a life-threatening situation, especially when urgent surgery and anaesthesia are necessary for unplanned indications, defined as immediate, urgent, or expedited. This most often applies to children who have sustained trauma requiring urgent surgical intervention. Another group includes patients with airway obstruction due to inflammation, foreign bodies, bleeding, or impaired consciousness/awareness, for example, due to valvular- ventricular dysfunction. Patients with such disorders are often rated ASA IIIE (emergency) or higher. In turn, children diagnosed with acute appendicitis, mild gastrointestinal obstruction and/or perforation, testicular or ovarian torsion – in the absence of significant comorbidities – may be assessed ASA IIE. It should be remembered that children and adolescents qualified for emergency anaesthesia may constitute a non-heterogeneous group and require individualized treatment.
PREPARING THE MEDICAL TEAM AND EQUIPMENT FOR UNPLANNED ANAESTHESIA IN A PAEDIATRIC PATIENT
In the vast majority of cases, it is possible to prepare the team and equipment before the patient arrives. This principle applies to both the emergency department and the operating theatre. The following safeguards should be in place:
possibility of assistance from a second anaesthesiologist, a second nurse, an otolaryngologist in the event of a potentially difficult intubation, a surgeon to perform an emergency thoracostomy or needle thoracentesis, or a thoracotomy, or to prevent external bleeding,
preparation of pediatric charts/tapes or the possibility of using a mobile device application [56, 57] to determine the correct values of vital signs for a given patient and to select appropriate equipment and calculate drug doses, both those used during anaesthesia and for resuscitation. Equipment for alternative airway management, i.e., a bronchofiberoscope and a video laryngoscope, should also be prepared. It is important to remember that, for example, the Broselow tape is accurate, but its use is associated with a tendency to underestimate body weight in populations with a high prevalence of obesity. Conversion systems adjusted for body composition (e.g., Pawper) are more accurate:
– preparing the device for point-of-care ultrasound (POCUS) to diagnose/exclude pneumothorax, pulmonary oedema, pleural effusion, pericardial tamponade, assess cardiac contractility, identify internal bleeding, and estimate the degree of vascular bed filling [58],
– considering preparation of a portable X-ray device (C-arm) based on knowledge of the mechanism of injury,
– notifying the radiology department, serology department, laboratory, and intra-hospital transport, if this has not been done before.
PREPARING THE PATIENT FOR EMERGENCY ANAESTHESIA
When a patient arrives at the hospital, it is first necessary to exclude immediately life-threatening conditions, such as airway obstruction, tension pneumothorax, massive external haemorrhage, and pericardial tamponade. If the intervention was performed by the emergency department team, it should be confirmed whether a second intervention is necessary before general anaesthesia is administered.
The general rule is to strive for maximum stabilization of the patient’s condition before transport or anaesthesia.
The “load and go” principle is used in exceptional situations when improvement is only possible in a specialist hospital, or due to the lack of immediate surgical intervention, which may lead to a significant deterioration of the patient’s condition, including death. Even in such a situation, it does not release the doctor from the obligation to examine the patient, protect basic vital functions, and try to stabilize their condition [59].
ABCDE PROCEDURE
Preparation for anaesthesia is facilitated by the ABCDE formula, commonly used in emergency medicine. Importantly, many of the following steps are performed simultaneously, and the formula allows for the memorization of all components.
A – Airway
In emergencies, especially if transport or surgery is anticipated, it is necessary to secure the airway by intubation (Table 28). Intubation should always be performed after preparation/stabilization of the patient [59, 60]. The only exception is when the airway is obstructed and cannot be cleared by other methods. In particular:
more equipment should always be prepared than is required for the weight or age of the paediatric patient,
in emergencies, it may be justified to use a tube with a cuff one size smaller than expected in case of difficult intubation,
the cuff pressure should be monitored and adjusted according to the manufacturer’s recommendations (usually < 20–25 cmH2O),
oral intubation is recommended unless the intubating person is experienced in nasal intubation and there are no contraindications to nasal intubation, such as suspected skull base fracture or coagulopathies,
after intubation, the endotracheal tube must be attached very carefully,
in children with suspected cervical spine injury, excessive head tilt should be avoided and intubation should be performed by two people, with the second person providing manual in-line stabilization of the head,
currently, the routine use of a rigid cervical collar is not recommended as it may cause problems with airway obstruction or impede cerebral perfusion (pressure on vessels),
if possible, movement of the entire spine should be minimized to prevent secondary cervical spine injuries,
after intubation, the patient should have a gastric catheter inserted through the nose to decompress the contents,
in the presence of contraindications, the same as for nasal intubation, the catheter should be inserted through the mouth,
the endotracheal tube must not be obstructed by residual contents in the respiratory tract (e.g., as a result of aspiration).
B – Breathing
Ventilation after tracheal intubation must be adjusted to the patient’s body weight and potential lung injury. A suitable initial target tidal volume should be 6–8 mL kg–1 of ideal body weight, taking into account the dead space (of the machine). It is necessary to check whether a tension pneumothorax has occurred, and in addition:
an intubated child must not be left breathing spontaneously through the endotracheal tube,
the use of a precordial/esophageal stethoscope during anaesthesia should be considered,
the use of capnography and maintenance of normocapnia is mandatory.
TABLE 28
Indications for intubation in emergency situations
C – Circulation
If pre-hospital or emergency department staff have not established intravenous access in the patient, this should be done immediately before anaesthesia. If intravenous access cannot be obtained, intraosseous access should be established as soon as possible (within 5 minutes or after 2 unsuccessful attempts to establish peripheral access), which can be used until the patient is stabilized and intravenous access is obtained (preferably via a central vein). Next, the following should be done:
blood should be taken for basic tests (acid-base balance, lactate, complete blood count, coagulation system including fibrinogen concentration, electrolyte analysis, biochemical tests) as well as blood type determination and crossmatching,
in the case of bleeding, blood products should be ordered,
the laboratory should be informed about the type of blood sample to be submitted for testing (arterial, venous, capillary, bone marrow), as in most cases the critical parameter analyser does not allow for a bone marrow blood gas test,
in the case of non-cardiogenic shock, fluid resuscitation should be started in boluses of balanced crystalloid fluids without glucose, in a volume of 10 mL kg–1 b.w.; after each bolus, the effectiveness of fluid resuscitation should be assessed; if there is no response to fluid therapy, vasoactive drugs should be introduced,
in the case of hemorrhagic shock, the use of crystalloid boluses should be limited to a minimum (max. 20 mL kg–1 b.w.) and blood products should be used as soon as possible (red blood cell concentrate combined with plasma and platelet concentrate) [54],
in the case of massive bleeding and the simultaneous lack of appropriately selected preparations for the patient, universal blood of group O Rh negative and/or fresh frozen plasma of AB group should be transfused,
pain relief treatment should be initiated as soon as possible if it has not been done before,
in children with circulatory failure whose clinical condition has not improved despite repeated fluid boluses, vasoactive drugs should be administered early by continuous infusion and continued during anaesthesia; the vasoconstrictor of choice is noradrenaline or adrenaline (0.01–0.05 μg kg–1 b.w. min–1); the vasodilator inotropic drug is dobutamine (5–10 μg kg–1 b.w. min–1) or milrinone (0.4–0.7 μg kg–1 b.w. min–1), which, unlike dobuta-mine, does not cause tachycardia. Dopamine use is permitted in the absence of both adrenaline and noradrenaline availability [60, 61],
in children with cardiogenic shock, the use of diuretics should be considered.
In some situations, albumin is at least as effective as crystalloids in terms of treatment outcomes, but due to its high cost, it should be considered a second-line fluid.
Stress-dose corticosteroids may be considered in children with septic shock who are unresponsive to fluids and require vasoactive drugs (moderate to high doses), regardless of any biochemical or other parameters. In such situations, the administration of hydrocortisone is recommended [59–61].
D – Disability
Before initiating anaesthesia, the patient’s neurological status should be assessed using the (paediatric) Glasgow Coma Scale (GCS) or the motor part of this scale. Pupils should be assessed (diameter, symmetry, and reaction to light), glucose levels should be measured, and the results of a CT/MRI of the head, if performed, should be reviewed.
INDUCTION OF ANAESTHESIA
All paediatric patients with life-threatening conditions requiring urgent surgical intervention and general anaesthesia should be treated as patients with a full stomach. Whenever possible, passive pre-oxygenation should be used; in children with upper respiratory tract obstructions, this is possible in a sitting position. This is the only situation in which inhalation induction with sevoflurane in 100% oxygen, after establishing intravenous access, is the preferred method. In all other cases, intravenous or intraosseous induction is used in children on a full stomach. Intubation is the treatment of choice. The principles of anaesthesia in a child with a full stomach are described in the general section [62].
Ketamine is the drug of choice for the induction of anaesthesia in mild shock; however, even with ketamine, unpredictable cardiovascular decompensation is possible. Etomidate may be administered to older children. In haemodynamically stable children with a full stomach, propofol is recommended, and for muscle relaxation – rocuronium or, in exceptional situations, succinylcholine chloride. It is important to remember about absolute contra-indications to the use of succinylcholine chloride, such as muscular dystrophy (Becker or DMD), severe neuromuscular disease (e.g. severe cerebral palsy), more than 48–72 hours after burns, multiple organ injuries or acute spinal cord injury, crush injury with rhabdomyolysis, positive family history of malignant hyperthermia, and severe hyperkalemia [63].
MAINTENANCE OF ANAESTHESIA
In patients classified as ASA III or at higher risk according to the ASA classification, especially those with severe baseline conditions or prior to extensive surgery, it is advisable to introduce an intra- arterial line for invasive blood pressure measurement, a central venous catheter (both preferably guided by ultrasound), and a urinary bladder catheter after induction of anaesthesia and stabilization. Minimally invasive cardiac output monitoring should be considered.
TABLE 29
Pre-transport/anaesthesia checklist
[i] ECG – electrocardiographic examination, ETCO2 – end-tidal carbon dioxide concentration, f – respiratory rate, FiO2 (fraction of inspired oxygen) – amount of oxygen in the respiratory mixture, NaCl – sodium chloride, PEEP – positive end-expiratory pressure, SBP – systolic blood pressure, SpO2 – blood saturation (saturation of hemoglobin with oxygen)
Excessive fluid intake should be avoided, but untill surgical supply of bleeding, the patient should be provided with adequate tissue perfusion. Permissive hypotension (mean arterial pressure at the 5th percentile for age) should only be considered in children who are not at risk of concomitant brain injury. In the latter, it may lead to decreased cerebral perfusion pressure.
In children classified as ASA I or II with stable circulation and respiration, who are qualified for appendectomy, standard monitoring is sufficient.
To maintain anaesthesia in a child in serious condition, combined anaesthesia is used, including opioid drugs, inhalational anaesthetics in a mixture of oxygen and air, titrated according to blood pressure, and non-depolarizing muscle relaxants. In addition, it is necessary to maintain normoxemia and normocapnia (except in the event of a sudden increase in intracranial pressure threatening herniation, in which case hyperventilation is temporarily indicated). In emergencies involving critically ill children, regional anaesthesia is rarely used, sometimes only in the postoperative period. In such cases, continuous regional analgesia may also be used. Every child with severe trauma who requires blood product transfusion should be given tranexamic acid (TxA) as soon as possible, within the first 3 hours after the injury and/or the occurrence of severe bleeding. The initial dose is 15–20 mg kg–1 b.w. (max. 1 g), followed by an infusion of 2 mg kg–1 b.w. h–1 for at least 8 hours or until the bleeding stops (max. 1 g) [64].
Furthermore, during anaesthesia, the patient should be protected from heat loss or actively warm ed. Central and peripheral temperature should be monitored (optimally, the difference should not exceed 1°C). In children with shock, there is an increased risk of intraoperative awakening; therefore, monitoring the depth of anaesthesia is recommended.
ANAESTHESIA RECOVERY PERIOD
Children in serious condition usually do not wake up immediately after the procedure, but continue treatment in intensive care or postoperative intensive care units. If the surgical procedure aims to initially stabilize the paediatric patient (e.g. to control bleeding), the patient should be transported to a specialist centre using appropriately prepared medical transport designed for the transport of paediatric patients (Table 29).
In special situations, it may be necessary to use extracorporeal life support (ECLS) techniques (e.g. refractory septic shock, cardiomyopathy, or myocarditis with refractory low output syndrome, severe hypothermia, poisoning with drugs that impair myocardial contractility).