
Hip surgery is frequently associated with significant pain in the postoperative period [1]. Several regional analgesic techniques have been proposed to manage postoperative pain after hip surgery [2]. However, mobility disorders are associated with the femoral nerve block, fascia iliaca block, lumbar plexus block, and epidural anesthesia [3]. Hip surgery is related to the risk of peripheral nerve injury, and prolonged sensory block can delay the recognition and treatment of nerve impairment [4]. Motor-sparing blocks such as the lumbar erector spinae plane block (L-ESPB) and pericapsular nerve group (PENG) block prevent this complication [2, 5].
The literature on L-ESPB and PENG block for use in total hip arthroplasty is limited, and its effectiveness and the amount of local anesthetic used are controversial [6, 7].
Regional anesthesia inhibits the stress response associated with the surgical intervention by modulating the neuroendocrine system, causing the secretion of neuroendocrine hormones and cytokines [8]. Postoperative pain, described as neuropathic, inflammatory, and nociceptive, is often associated with a reaction to surgical stimuli [9]. Systemic changes in leukocyte count, including lymphopenia, leukocytosis, and neutrophilia, frequently develop in response to surgery.
Platelet-to-lymphocyte ratio (PLR) and neutrophil- to-lymphocyte ratio (NLR) are often used as immune system markers against various non-infectious sti-muli. Surgical trauma and the method of anesthesia influence the stress response [10].
We designed this randomized, double-blinded, controlled trial to compare the effects of L-ESPB and PENG block on postoperative analgesia after total hip arthroplasty. Our primary endpoint was total opioid consumption. Secondary endpoints included pain scores, time to first rescue opioid anal-gesia, quadriceps muscle strength, and NLR and PLR levels.
Methods
Study design
This double-blinded, prospective, randomized controlled trial was conducted in a single orthopedic center in Poland. The Poznan University of Medical Sciences Bioethics Committee approved the study on March 7, 2023, protocol number 104/24, and on October 16, 2023, the trial was registered at ClinicalTrials.gov (NCT06083428). Written informed consent was obtained from all patients for these scientific contributions. Enrollment occurred from 17.10.2023 to 11.06.2024. The study was conducted in line with the Declaration of Helsinki.
Participants
Enrollment was proposed before surgery to patients scheduled for total hip arthroplasty under spinal anesthesia, aged 20–90 years, and American Society of Anesthesiologists physical status (ASA) I, II, or III.
Patients were not included in this study if they refused to participate, had a history of bleeding diathesis, took anticoagulant therapy, had a history of chronic pain before the surgery, had multiple traumas, could not assess their pain, had been operated on under general anesthesia, had an infection in the puncture site, had ASA > III, or did not accept the procedure.
Randomization and concealment
Computer software randomly assigned patients 1 : 1 : 1 to receive ultrasound-guided PENG block, L-ESPB, or to the Control group, using a randomization list generated by the nQuery Advisor program (Statistical Solutions, Boston, MA, USA).
The double-blinding in this study was accomplished via the strict design of the work tasks for the researchers, who were unaware of each other’s final scores. One researcher, uninvolved in the study, prepared the randomization list and enclosed sheets containing group assignments in opaque and serially numbered envelopes. The “first” consultant anesthesiologist received and opened the envelopes before the orthopedic procedures and applied the PENG block or lumbar ESPB according to group assignments. The “first” consultant was then replaced by a “second” consultant who supervised all subsequent procedures associated with the surgical procedure without any knowledge regarding using PENG or ESPB block. Consequently, the anesthesia team, surgeons, operating room staff, and patients were blinded to the study group assignment. The group blinding was unmasked after the statistical analysis was completed.
All patients underwent hip surgery under spinal anesthesia performed by one surgical team (four surgeons) at the Orthopaedical Hospital at Poznan University of Medical Sciences. The same surgical technique (direct superior approach) and uncemented implant (Smith-Nephew Polarstem/R3, Watford, UK) were used in all patients. The day following the procedure, radiographs were taken, and patients followed standardized rehabilitation and pain management protocols (as described below). Walking was allowed with two crutches, and weight bearing as tolerated was encouraged.
The patients underwent at least two days of active follow-up after surgery. An independent researcher gathered the primary and secondary outcomes during in-patient hospital visits.
Procedures
In all three groups, the patients received midazolam 7.5 mg PO 30 minutes before surgery as part of the multimodal preemptive analgesia protocol. All patients received standardized spinal anesthesia under mild sedation, as is common practice in our hospital. Mild sedation was performed with continuous propofol infusion at 5 mg kg–1 hour–1, which was continued throughout the entire surgery. Spontaneous ventilation was maintained with an oxygen mask at 2 L min–1. Spinal anesthesia (L3/4, Sprotte needle 27 G, 90 mm, PAJUNK, Geisingen, Germany) was performed with 4 mL of 0.5% ropivacaine spinal. There was no surgeon-delivered periarticular infiltration during surgery. The “first” and “second” anesthesiologists involved in this study had at least five years of post-specialty clinical expertise focused on regional anesthesia and nerve blocks.
PENG block procedure
After the spinal anesthesia and before the surgical incision, the PENG block was performed. The patient was placed in the supine position. A curvilinear, low-frequency 4–8 MHz sonographic ultrasound probe and a 22-gauge needle (Stimuplex Ultra 360, 80 mm, BBraun, Melsungen, Germany) were used. The puncture was performed in the lateromedial direction. To avoid quadriceps weakness, the needle was placed away and more laterally to the iliopsoas tendon between the ilio-pubic eminence and anteroinferior iliac spine [11–13]. Hydro-location positioning was performed with 0.5 mL of 0.9% isotonic saline. After the negative aspiration, 20 mL of 0.2% ropivacaine was slowly placed laterally to the iliopsoas tendon [14].
Lumbar ESPB procedure
After the spinal anesthesia and before the surgical incision, the ESPB was performed at the L4 vertebral level. The patient was placed in the lateral position with the operated side up. We used a curvilinear, low-frequency 4–8 Hz probe and a 22-gauge needle (Stimuplex Ultra 360, 80 mm, BBraun, Melsungen, Germany). The transducer was placed in a paramedian sagittal orientation at the level of the spinous processes. The needle was inserted in-plane from cranial to caudal direction until the needle tip contacted the transverse process. Then 2 mL of 0.9% isotonic saline was injected to confirm the proper injection plane by visualizing the spread deep to the erector spinae muscles and superficial to the transverse process. After negative aspiration, 20 mL of 0.2% ropivacaine was injected into the confirmed fascial plane between the transverse process and the erector spinae muscle [15].
Postoperative analgesia management
Postoperative analgesia included the adminis-tration of acetaminophen 1.0 g every 6 hours, meta-mizole 1.0 g every 6 hours, and ibuprofen 400 mg every 8 hours. Additionally, if the patient’s NRS (Numerical Rating Scale) score was 4 or above, a 5 mg oxycodone bolus injection was administered for rescue analgesia. Daily enoxaparin was given postoperatively for four weeks to all patients as thromboembolism prophylaxis. After the first ten postoperative hours, patients were ambulated with the assistance of a walker.
Although oxycodone IV was used as rescue opioid analgesia, total opioid consumption is presented in morphine milliequivalents (mEQ) to standardize the results and facilitate comparison with other studies. The conversion was performed using the accepted conversion ratio of 1 mg oxycodone = 1.5 mg morphine.
Outcome measures
Primary outcome
The total opioid consumption was accessed from the orthopedic wards by the residents and fellows, who were blinded to the study. The total consumption data, initially recorded in milligrams of oxycodone, were converted into morphine milliequivalents (mEq) for consistency with other studies and ease of comparison.
Secondary outcomes
At all postoperative time points (3, 6, 12, 18, 24, 48 hours after surgery), the pain score was assessed using the NRS score (0 meaning no pain and 10 meaning the worst pain imaginable). Two independent physicians evaluated the subject during the examination. The final score was agreed upon at the end of the examination. The quadriceps strength score was assessed using the Medical Research Council (MRC) Scale for Muscle Strength, where grade 5 means normal muscle strength, grade 4 means movement against gravity and resistance, grade 3 means movement against gravity over (almost) the entire range, grade 2 means movement of the limb but not against gravity, grade 1 means visible contraction without movement of the limb (not existent for hip flexion), and grade 0 means no visible contraction. Two independent physicians evaluated the quadriceps muscle strength during the examination, and the final score was agreed upon at the end of the examination. Blood samples for PLR and NLR were obtained 24 h and 48 h after surgery by nurses who were blinded to the study. Two researchers blinded to the group allocation assessed the outcomes.
Statistical analysis
The sample size was based on our primary hypo-thesis that the lumbar ESPB improves pain management compared to the PENG block and no-block analgesia. The total opioid consumption 48 hours after surgery was the primary outcome variable. Based on our hospital’s retrospective analysis of unpublished data, we assumed a mean total opioid consumption over 48 hours after surgery of 4.0 ± 4.183 mEq (mean ± SD) in the PENG group and 3.0 ± 4.472 (mean ± SD) in the L-ESPB group. Assuming a = 0.05 and power = 0.8 using a two-sided c2 test with Bonferroni correction, the calculated sample size was 74. To ensure robust block randomization and account for up to 10% potential dropouts, we recruited 90 patients (30 per group). While the initial sample size calculation was performed for two groups, post hoc power analysis confirmed that our study remained adequately powered for three independent groups.
Statistical analysis was performed using GraphPad Prism 10.1.1 (270) software (GraphPad Software Inc., San Diego, CA, USA). The parametric distribution of numerical variables was evaluated using the Shapiro-Wilk normality test. The ANOVA or Kruskal-Wallis test with post hoc Tukey’s or Dunn’s test was used to assess group differences. Categorical variables were compared with the Kruskal- Wallis test, and an analysis of contingency was compared with Fisher’s exact test. A P-value <0.05 was considered statistically significant.
Delta NLR and delta PLR values were calculated by subtracting the baseline (preoperative) values from the corresponding postoperative values at 24 and 48 hours. The ANOVA or Kruskal-Wallis test was used to compare delta values among the groups, depending on the normality of data distribution. Post hoc pairwise comparisons were performed using Tukey’s test for parametric data or Dunn’s test for nonparametric data. These methods were chosen to ensure an accurate interpretation of changes in inflammatory markers over time. Statistical significance for comparison of delta values was set at P < 0.05.
Results
Of the 112 patients assessed for eligibility, 17 did not meet the inclusion criteria, and 5 refused participation. The remaining 90 were randomly allocated to three groups and analyzed, as seen in Figure 1. No clinically relevant differences were apparent from group characteristics, as shown in Table 1.
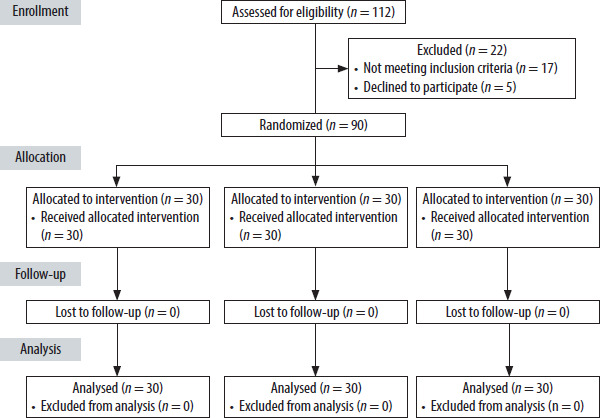
TABLE 1
Baseline characteristics
a P-value compares the control group to the PENG group. bANOVA or Kruskal-Wallis test with post-hoc Tukey’s or Dunn’s test used to compare means between the groups; or Fisher’s exact test. cP-value compares the control group to the ESPB group. dP-value compares the PENG group to the ESPB group. eP-value compares all three groups.
Primary outcome
The total opioid consumption within 48 hours after surgery, expressed in milliequivalents of intravenous morphine, was significantly lower in the L-ESPB compared to the control group (3.4 ± 3.8 vs. 16.07 ± 3.8, P < 0.00001) and in the PENG group compared to the Control group (3.5 ± 4.0 vs. 16.07 ± 3.8, P < 0.000001). However, total opioid consumption was similar in the PENG group and L-ESPB group, with P = 1.0, as seen in Table 2.
TABLE 2
Primary and secondary outcomes
a P-value compares the control group to the PENG group. bANOVA or Kruskal-Wallis test with post-hoc Tukey’s or Dunn’s test used to compare means between the groups. cP-value compares the control group to the lumbar ESPB group. dP-value compares the PENG group to the lumbar ESPB group. eP-value compares all three groups.
Also, 14 patients in the L-ESPB and 14 patients in the PENG group did not require opioids after surgery, unlike the Control group, where all the patients needed opioids postoperatively, P < 0.00001.
Secondary outcomes
The time to first rescue opioid analgesia was significantly longer in the L-ESPB group (11.2 ± 2.9) and the PENG block group (12.3 ± 3.2) compared to the Control group (4.2 ± 1.1), with P < 0.001. The time to first rescue analgesia was similar between the L-ESPB and PENG block groups, with P = 1.0.
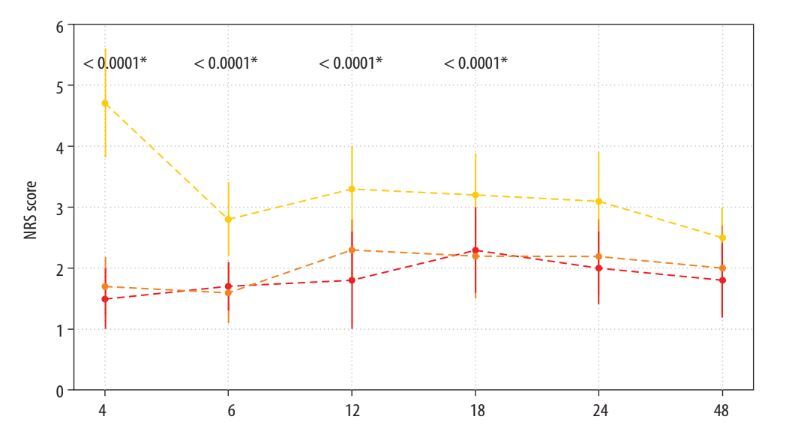
The L-ESPB and PENG block group patients had lower NRS scores at all time points (3, 6, 12, 18, 24, and 48 hours after surgery) than the Control group, as seen in Figure 2.
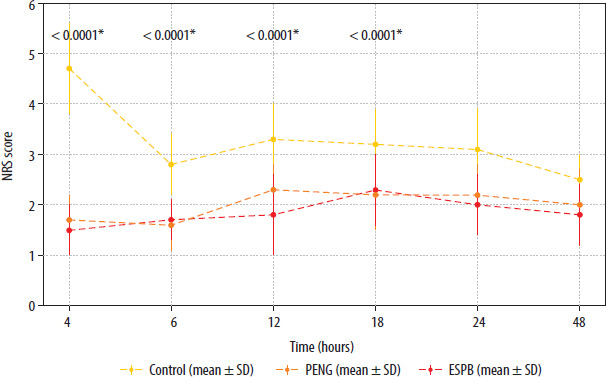
The NRS scores did not differ between the L-ESPB and the PENG block groups at all time points.
The NLR levels did not significantly differ between all three groups, with P = 0.9532. However, 24 hours after surgery, the NLR values were significantly lower in the L-ESPB compared to the Control group (3.6 ± 0.7 vs. 4.3 ± 0.9, P = 0.0047) and in the PENG group compared to the Control group (3.6 ± 0.6 vs. 4.3 ± 0.9, P = 0.0106). There was no difference in the NLR levels between the L-ESPB and PENG groups, with P = 1.0. Delta NLR (24 h − baseline) values were significantly lower in both the L-ESPB and PENG groups compared to the Control group (L-ESPB: 1.8 ± 0.6, PENG: 1.8 ± 0.5 vs. Control: 2.4 ± 0.9, P = 0.0023 and P = 0.0029, respectively). The delta NLR values at 48 hours were also significantly lower in the L-ESPB and PENG groups compared to the Control group (L-ESPB: 1.2 ± 0.5, PENG: 1.1 ± 0.6 vs. Control: 2.0 ± 0.8, P = 0.0015 and P = 0.0031, respectively). Also, 48 hours after surgery, the NLR levels were significantly lower in the L-ESPB and the PENG block groups than in the Control group. Also, there was no difference between the L-ESPB and the PENG block groups (P = 1.0).
The PLR values before surgery were similar in the L-ESPB group compared to the control group and in the PENG block group compared to the PENG block group. There was a significant difference in PLR levels between the L-ESPB and the PENG block groups before the surgery, P = 0.0004. The PLR levels 24 h and 48 h after surgery were significantly lower in the L-ESPB and the PENG block groups compared to the Control group (all P < 0.001). Delta PLR (24h – baseline) was significantly lower in the L-ESPB group (142.7 ± 70.3) compared to both the Control group (227.2 ± 78.7, P < 0.001) and the PENG block group (90.1 ± 56.3, P = 0.0018). Similarly, delta PLR at 48 hours was significantly lower in the L-ESPB group (76.9 ± 55.8) compared to the Control group (143.2 ± 62.3, P < 0.001) but not significantly different from the PENG group (41.9 ± 52.2, P = 0.0042). There was no difference in the PLR between the L-ESPB and the PENG block group levels 24 h (P = 0.9997) and 48 h (P = 1.0) after surgery.
The quadriceps muscle strength measured by knee extension was significantly lower in the PENG group 3 h after surgery compared to the control group (3.9 ± 0.8 vs. 4.5 ± 0.7, P = 0.0144) and 6 hours after surgery compared to the L-ESPB group (4.7 ± 0.5 vs. 5.0 ± 0.0, P = 0.0050).
The quadriceps muscle strength measured by hip adduction was significantly lower in the PEG block group 6 hours after surgery compared to the Control group (4.6 ± 0.6 vs. 4.9 ± 0.3, P = 0.0166) and the L-ESPB group (4.6 ± 0.6 vs. 5.0 ± 0.0, P = 0.0012).
Discussion
Our study showed that preoperative L-ESPB and PENG block significantly lowered the total opioid consumption, prolonged the time to first rescue opioid analgesia, lowered the pain level, and lowered the stress response expressed by the NLR and PLR in patients undergoing total hip arthroplasty. Our results suggest that preemptive L-ESPB preserves motor function better than PENG block in patients undergoing total hip arthroplasty.
Our study is one of the few comparing the effectiveness of L-ESPB and PENG block for pain management following total hip arthroplasty. Two published randomized controlled trials compare L-ESPB and PENG block in patients undergoing total hip arthroplasty [16, 17].
Medhat et al. [16] and Küçük et al. [17] rando-mized 69 elderly patients to three equal groups: the PENG block, L-ESPB, and Control groups.
In our study, the total opioid consumption was similar in the PENG block group and the L-ESPB group. Unlike Medhat et al. [16] and Küçük et al. [17], in our research, the total opioid consumption was lower and very similar in the PENG block and L-ESPB groups compared to the Control group.
Unlike our research, Medhat et al. [16] found that PENG block significantly prolonged the time to first rescue opioid analgesia up to 13.3 h. Still, the pain scores were significantly higher in the PENG block group compared to the L-ESPB group. Küçük et al. [17] found that PENG block and L-ESPB prolonged the time to first rescue opioid analgesia up to 9.8 h in the PENG group and 8.0 h in the L-ESPB group. In our study, the time to first rescue opioid analgesia in the PENG block group was 12.3 h and 11.2 h in the L-ESPB group.
As in our research, the pain scores in the study by Küçük et al. [17] were similar in both groups but much lower than in the control group.
Küçük et al. [17] and Medhat et al. [16] did not evaluate quadriceps muscle strength following L-ESPB or PENG block in total hip arthroplasty. We found that L-ESPB preserved quadriceps muscle strength better than PENG block. The quadriceps muscle strength was slightly reduced up to 12 h after surgery in our trial, similar to other studies [13], despite modification of the technique by Tran et al. [11] and Peng et al. [12]. Our results are consistent with those of other randomized trials where PENG block caused slight quadricep impairment [18]. However, the quadriceps muscle weakness related to PENG block is much lower than that associated with femoral nerve block [19] or fascia iliaca block [20]. According to Girón-Arango et al. [21], the motor-sparing effect of PENG block is volume-dependent. The volumes of local anesthetics of 15 to 20 mL are optimal for achieving the best analgesic effect. However, these volumes bring the risk of femoral nerve impairment, probably due to the extensive spread of the local anesthetic leading to hip bursa rupture and femoral nerve flood [22]. Our results suggest that L-ESPB, better than PENG block, promotes functional recovery following total hip arthroplasty.
Küçük et al. [17] and Medhat et al. [16] did not evaluate the stress response following L-ESPB or PENG block in total hip arthroplasty. Our study showed that not only did PENG block and L-ESPB significantly reduce NLR and PLR levels at 24 and 48 hours compared to the Control group, but delta NLR and delta PLR values also provided more profound insights into the extent of postoperative inflammation control. The delta NLR values at 24 hours and at 48 hours were significantly lower in both the L-ESPB and PENG groups compared to the Control group, reflecting superior attenuation of the inflammatory response in the intervention groups. Similarly, delta PLR values at 24 hours and at 48 hours indicated a significantly lower inflammatory response in both block groups compared to the Control group.
These findings are clinically significant, as they suggest that both blocks, especially L-ESPB, reduce acute postoperative pain and the systemic inflammatory response following major orthopedic surgery, potentially leading to better outcomes and faster recovery.
As shown in previous studies, ESPB reduces the stress response caused by surgery and opioids [23, 24]. ESPB also reduced IL-6 and IL-10 levels associated with the stress response following significant spine surgery [25]. However, no studies have examined the influence of PENG block on the surgery stress response. Regional anesthesia influences the sympathetic and inflammatory response that occurs perioperatively due to vascular permeability, elevated blood flow, and leukocyte aggregation [26, 27]. The complete blood count estimates NLR and PLR from lymphocyte, neutrophil, and platelet values. PLR and NLR are inflammatory signs anticipating subclinical inflammation, mortality, and morbidity [28, 29]. Duran et al. [28] stated that NLR levels of 3.0 and above suggest infection, inflammation, stress, or cancer. Increasing NLR values express the severity of illness and level of stress [29, 30].
Limitations
The main limitation of this study was the small sample size. Additionally, the primary outcome, opioid consumption, was assessed using rescue bolus dosing instead of patient-controlled analgesia (PCA). While we acknowledge that PCA is widely considered a standard approach for postoperative pain mana-gement, in our center, PCA is not routinely used for elderly patients due to the increased risk of misuse and potential technical issues related to cognitive impairment. Therefore, we opted for rescue bolus dosing under close clinical supervision, which reflects our standard clinical practice. Furthermore, we did not obtain the NLR and PLR levels 6 and 12 hours after surgery, monitor the hospital discharge times, or monitor adverse effects. Further trials are required for local anesthetic solutions and doses.
Additionally, we acknowledge that the lack of preoperative pain data is a limitation of our study. Since hip replacement patients often experience chronic pain while waiting for surgery, not accounting for baseline pain levels may influence postoperative outcomes. Future studies should include preoperative pain assessments to better understand the effect of regional blocks on postoperative pain management.
As in all studies involving patients undergoing arthroplasty, there were variations in preoperative pain and hip joint functions, which could affect these parameters in the early postoperative period.
Conclusions
The PENG block and the L-ESPB provide efficient postoperative analgesia in elderly patients undergoing total hip arthroplasty. They lower total opioid consumption, the time to first rescue opioid analgesia, pain scores, and stress response to surgery, expressed by NLR and PLR levels. The L-ESPB block preserves quadriceps motor function better than the PENG block. This study found that both blocks significantly enhanced the quality of recovery. Those two blocks can be safely applied in total hip arthroplasty.