
Dear Editor,
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are a novel class of drugs that have emerged in the treatment of patients with type 2 diabetes mellitus and obesity. GLP-1RAs imitate the endogenous hormone GLP-1, which is normally released after meal ingestion [1]. Endogenous GLP-1 has a short half-life (2–3 minutes) and is rapidly metabolised after its secretion via the enzyme dipeptidyl peptidase (DPP-4), while GLP-1RAs have a prolonged half-life of approximately 7 days [2, 3], resulting in some long-lasting effects. Activation of the GLP-1 receptor results in increased insulin secretion and reduction of glucagon secretion [4]. Furthermore, these agents lead to a delay in gastric emptying [5], resulting in satiety and consequently reducing food intake. Therefore, the initiation of therapy with GLP-1RAs contributes to significant weight loss.
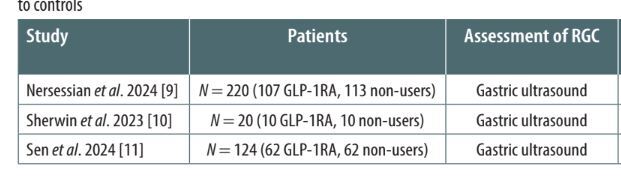
Among the effects of this class of drugs, slowing gastric emptying is the most notable concern for anaes thetists because of its potential increased risk of gastric regurgitation and subsequent pulmonary aspiration during induction of general anaesthesia. Although the evidence is accumulating rapidly, we think it is too early to pool the published studies in a metanalysis. In this letter, we summarise the findings of the most recent studies that have reported the potential impact of GLP-1RAs on the residual gastric content (RGC), in light of an increased risk of aspiration pneumonia for patients undergoing general anaesthesia and/or deep sedation (Table 1).
TABLE 1
Studies evaluating residual gastric content (RGC) and comparing patients exposed to glucagon-like peptide-1 receptor agonists (GLP-1RAs) to controls
| Study | Patients | Assessment of RGC | Results (incidence of increased residual gastric content) |
|---|---|---|---|
| Nersessian et al. 2024 [9] | N = 220 (107 GLP-1RA, 113 non-users) | Gastric ultrasound | 40% of users compared to 3% of non-users |
| Sherwin et al. 2023 [10] | N = 20 (10 GLP-1RA, 10 non-users) | Gastric ultrasound | 70% of users compared to 10% of non-users |
| Sen et al. 2024 [11] | N = 124 (62 GLP-1RA, 62 non-users) | Gastric ultrasound | 56% of users compared to 19% of non-users |
A retrospective observational study performed by Silveira et al. [6] in patients undergoing esophagogastroduodenoscopy under deep sedation or general anaesthesia revealed that RGC was present in 8 (24.2%) patients in the semaglutide group as compared to 19 (5.1%) among the non-users (P < 0.001). In this study, RGC was defined as the presence of any amount of solid or a fluid content with a quantified volume > 0.8 mL kg–1 measured from suction canister.
Wu et al. [7] performed a retrospective cohort study to assess the RGC during esophagogastroduodenos-copy in patients receiving GLP-1RAs and non-users. RGC was reported in 17 (19%) of the GLP-1RA users as compared to 5 (5%) of the non-users, with an associated adjusted odds ratio (OR) increased by almost 6-fold (5.8 with 95% confidence interval [95% CI]: 1.7–19.3, P = 0.004). Both Silveira et al. [6] and Wu et al. [7] reported one case of pulmonary aspiration in GLP-1RA users and none in the control group.
Baig et al. [8] performed a systematic review aimed at comparing the risk of RGC in GLP-1RA users and non-users undergoing endoscopy. RGC was reported in 20 out of 23 studies. The GLP-1 group users had significantly higher odds of having RGC during endoscopy as compared to the nonGLP-1 group (7% vs. 0.53%; OR 4.54, 95% CI: 3.30–6.24, P < 0.001).
The first 2 studies were performed in patients undergoing endoscopy procedures; hence, it was possible to directly quantify the presence of RGC. However, other studies have attempted to address the delayed gastric emptying in patients treated with GLP-1RAs with a different and novel approach, the use of point-of-care ultrasound (POCUS). In 2024 a prospective observational study, performed by Nersessian et al. [9] enrolled 220 patients, 107 in the semaglutide group and 113 in the non-semaglutide group. RGC was assessed by preope rative gastric ultrasound and determined the presence of solid content or a volume of clear fluid above 1.5 mL kg–1.
The authors noted increased RGC in 43 (40%) patients receiving subcutaneous semaglutide within the previous 10 days, as compared to 3 (3%) in the control group (P < 0.001). Their propensity-weighted analysis showed an extraordinary increased risk of increased RGC in the semaglutide users, with an OR of 37 [95% CI: 16.5–99.3].
Another study [10] was conducted in 20 healthy volunteers (half of them treated with GLP-1RAs) and assessed for RGC after 8 hours of fasting. The authors assessed volunteers in both supine and lateral positions with gastric ultrasound and then performed a second ultrasound 2 hours after approximately 350 mL of water intake. In the supine position the authors found that 7 (70%) of the semaglutide participants and one (10%) of the controls had solids on gastric ultrasound (P = 0.02). The prevalence increased on ultrasound performed in the lateral position (9 [90%] semaglutide vs. 2 [20%] controls, P = 0.005). After drinking water, the groups did not differ in the assessment in the lateral position, but in the supine position a significantly lower proportion of GLP-1RA volunteers had an empty stomach as compared to controls (30% vs. 90%, respectively; P = 0.02).
Subsequently, in a population of 124 patients undergoing elective surgery, Sen et al. [11] studied the influence of GLP-1RAs on the presence of RGC measured by gastric ultrasound and defined as the presence of solids, thick liquids, or more than 1.5 mL kg–1 of clear liquids. In this study 35 (56%) patients exposed to GLP-1RAs had an increased incidence of RGC as compared to 12 (19%) of the non-users, a finding that persisted after adjustment for confounders. However, the authors did not find an association between the timing of GLP-1 RA interruption and the occurrence of increased RGC, with an OR of 0.86 [95% CI: 0.65–1.14].
The above studies confirm, to varying extent, the presence of higher RGC in patients exposed to GLP-1Ras; there are also various case reports that have detailed the presence of retained solids in gastric ultrasound or endoscopy assessment [12–14]. Furthermore, there are also several reports describing episodes of pulmonary aspiration in appropriately fasted patients on GLP-1RA therapy [7, 15–18]. From the above evidence, it is clear that the best approach for the management of patients on GLP-1RAs still needs further investigation.
In 2024 consensus-based guidance was formulated by representatives from the American Society of Anesthesiologists (ASA), the American Gastrointestinal Association (AGA), the American Society for Metabolic and Bariatric Surgery (ASMBS), the International Society of Perioperative Care of Patients with Obesity (ISPCOP), and the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) [19], according to which, use of GLP-1RAs and the management in the perioperative period should be based on shared decision-making of the patient, the anaesthetist, the prescribing care team, and the surgeon [19, 20]. The first step in the pre-operative care of a patient on GLP-1RAs should involve an assessment of the risk of aspiration, taking into account factors that may increase this risk, including the escalation phase of GLP-1RA dosing or a high-dose protocol, the presence of gastrointestinal symptoms of delayed gastric emptying (e.g. nausea, vomiting, and abdominal discomfort), as well as other medical conditions that might delay gastric emptying such as Parkinson’s disease, multiple sclerosis, amyloidosis, and scleroderma [19, 20]. According to the above consensus, patients without risk factors may continue their GLP-1RAs therapy in the perioperative period. Conversely, in patients considered at high-risk of aspiration, a liquid diet is recommended for at least 24 hours before surgery [19, 20]. If the decision to withhold GLP-1RAs is indicated, the duration of cessation should follow the guidance of the ASA: on the day of the procedure for daily formulations, and one week prior for weekly formulations [20, 21]. However, anaesthetists must be aware that withholding the therapy in patients with type 2 diabetes mellitus may increase the risk of perioperative hyperglycaemia, which can, in turn, elevate the likelihood of postoperative complications, such as wound infections [22]. Due to the increasing popularity of GLP-1RAs in patients with obesity, it seems crucial to recognise the peri-operative management in this group of patients. Multi-society consensus advises that withholding therapy in patients without the risk factors described above should be avoided [20]. Nevertheless, such consensus is not an evidence-based guideline. As an example, Nersessian et al. [9] showed that 10-day cessation of semaglutide was still insufficient in some cases, and 40% of the patients presented RGC in gastric ultrasound. Meanwhile, performing a preoperative assessment for RGC using gastric ultrasound in patients continuing GLP-1RA therapy appears reasonable, given the simplicity and feasibility of point-of-care gastric ultrasound [10, 11, 23]. The implementation of this non-invasive tool may help reduce risks to patients and potentially prevent unnecessary surgical cancellations in GLP-1RA users. Some authors suggest that it might have limited application due to its variability [24]. However, given the uncertainty of the interruption interval of these medications, gastric ultrasound appears to be a crucial tool for identifying patients at high risk of pulmonary aspiration
In summary, emerging evidence suggests that perioperative use of GLP-1RAs is associated with delayed gastric emptying and greater RGC, which in turn may increase the risk of pulmonary aspiration. Current recommendations remain based on experts’ opinions, and the evidence is rather limited. Due to the increasing popularity of GLP-1RAs in patients with obesity, we call for further high-quality studies to address the optimal perioperative care of patients on GLP-1RAs.