
Maintaining control over the airway is crucial during general anesthesia (GA). One of the most dangerous scenarios for both the patient and the anesthesiologist is an unanticipated or anti- cipated difficult airway [1], with risk of failure to intubate increasing when difficult laryngoscopy prevents the vocal cords from being observed after multiple attempts [2]. Appropriate choices to re- duce potential hazards to the patient are made by preoperative airway risk assessment and planning for challenging airway management [3].
Improved laryngeal views, a higher rate of suc- cessful intubation, a higher rate of first attempts, and fewer intubation maneuvers with the aid of video laryngoscopy (VL) were reported in mul- tiple meta-analyses of randomized controlled tri- als comparing VL with direct laryngoscopy (DL) in patients with predicted difficult airways [4, 5]. Multiple studies have been carried out to compare different kinds of VLs in order to enhance the effi- cacy of intubation [6]. Ultimately, conflicting find- ings about the laryngeal view, overall success rate, first attempt success rate, and intubation time were published.
Currently, more and more experts advise rou- tinely using VL rather than DL as the main intubation technique. Increasing evidence demonstrates that VL is superior in enhancing the success rates of first intubation attempts, reducing the risk of esophageal intubation, and decreasing the overall time required for a successful intubation. This shift from DL to VL reflects a broader pattern in modern anesthetic care that emphasizes the use of cutting-edge technology to improve patient outcomes [7].
The Sanyar video laryngoscope (SL) is a new, portable VL with LED lights at the blade’s end, a high-resolution camera with a wide field of view, and a hyper-angulated blade. The camera at the end of the blade provides a close-up of the glottis as well as a large, clear image. Images taken by the camera can be viewed and recorded on the operator’s mobile device via Wi-Fi networks. The blade has an 11-de- gree left angle, which causes the tongue to move to the left side as it enters the mouth, making it easier to see the glottis and place a tracheal tube (Figure 1).
FIGURE 1
The Sanyar video laryngoscope. 1) Cap with on/off button, 2) blade, 3) camera, 4) mobile LCD display

The efficacy of the SL in comparison with the di- rect laryngoscope in a normal population under- going GA has been demonstrated in our previous studies [8, 9].
This study aimed to assess the non-inferiority of the SL in comparison to the GlideScope video la- ryngoscope (GL) in patients with difficult airways. We considered the success rate of intubation in the first attempt at laryngoscopy as the primary outcome. Blood pressure (BP) and heart rate (HR) changes during laryngoscopy and intubation, and the dura- tion of intubation from the time the laryngoscope blade entered the patient’s mouth to the placement of the tracheal tube in the trachea were the second- ary outcomes.
METHODS
This study was a randomized, controlled, two- armed, parallel clinical trial that aimed to compare the effectiveness of the SL with the GL for intuba- tion in patients with predicted difficult airways.
Following research approval from the ethics committee of Tehran University of Medical Sciences (ethical code: IR.TUMS.SINAHOSPITAL.REC.1401.099; January 24, 2023), this trial was officially registered in the Iranian Clinical Trials Registry (IRCT) with the IRCT number of IRCT20130304012695N15. In accordance with the Declaration of Helsinki, every participant gave written informed consent prior to being enrolled.
Study population
Participants in the study were those between the ages of 18 and 65 who met at least one criterion for a difficult airway, with an ASA of ≤ 3 based on the airway physical examination and history.
Patients were classified as potentially difficult for tracheal intubation if they met at least one of the fol- lowing criteria: restricted cervical spine mobility re- sulting from pathological conditions or precautions, specifically limited flexion and extension of the neck; Mallampati classification grade III or IV; diminished mouth opening (less than 3 cm); previous difficulties with direct laryngoscopy; thyromental distance; and thyromental height less than 5 cm.
The study’s exclusion criteria included patients with impaired airways and emergency cases neces- sitating rapid sequence induction.
Sample size calculation
Considering that the SL increases the first intuba- tion success rate by 5%, a sample size of 45 patients was required for each of the analyzed groups with a statistical error of 0.05% and study power of 80%.
Intervention
The eligible patients were randomly assigned to two groups: the intervention group intubated by SL, and the control group intubated by GL.
The anesthesia induction process was the same in all groups, using midazolam at a dosage of 0.02 mg kg–1, fentanyl at a dosage of 2 µg kg–1, pro- pofol at a dosage of 1.5 mg kg–1, and atracurium at a dosage of 0.5 mg kg–1.
Both of the highly skilled anesthesiologists who conducted this investigation had at least ten years of expertise. Before the trial, they had used the GL for at least three years and the SL for a year. This level of experience with both devices guaranteed that the operators were skilled in their usage, which is crucial for effective intubation results.
Laryngoscopy was conducted after confirming full neuromuscular blockade using train-of-four stimulation of the ulnar nerve and was carried out by two highly experienced anesthesiologists who had a minimum of 10 years of experience. They had been performing intubation procedures using the GL for at least three years and the SL for one year.
Following two unsuccessful efforts at laryn- goscopy and unsuccessful intubation, the trial was terminated in all patients, and LMA (laryngeal mask airway) was utilized for airway management.
Randomization
Block randomization was performed through the website https://www.sealedenvelope.com. The sample size was organized into 4 blocks. An independent researcher, not involved in the study, generated a random list to assign participants to different groups. The principal investigator then ensured that participants were placed in the correct group according to the eligibility criteria.
Monitoring
All patients were fitted with intravenous cathe ters and underwent standard monitoring, which includ- ed electrocardiogram, non-invasive blood pressure measurement, pulse oximetry, and capnography.
The airway physical examination includes modified Mallampati scores, thyromental distance, thyromental height, interincisal distance, and neck extension.
BP and HR were continuously measured during the laryngoscopy and intubation operations. The success rate of intubation at the first attempt during laryngoscopy was the main outcome that was measured. The duration of intubation, glottic visualization based on the Cormack-Lehane (CL) score, HR and MAP after intubation were assessed as the secondary outcomes.
The duration of intubation was determined from the entry of the laryngoscope into the oral cavity until the observation of the capnography waveform. Additionally, the success of the intubation proce- dure was validated by the presence of the capnography waveform.
Glottis visualization during laryngoscopy was evaluated using the CL scoring system.
During the laryngoscopy phase, the following outcomes were recorded: number of intubation at- tempts, laryngeal view according to the CL scoring system, incidence of complications, including hypo- xemia, dental trauma and laryngeal injuries.
Statistical analysis
SPSS version 24 was used to analyze the data. Using the Kolmogorov-Smirnov test, the norma lity of the data distribution was evaluated. The c2 test and Student’s t-test were applied to compare base- line data. Additionally, the relationship between the study variables and the intubation time was exa mined using multiple linear regression.
For quantitative variables, data are expressed as mean ± SD, and for qualitative factors, as number (%). A significance threshold of 0.05 was chosen.
RESULTS
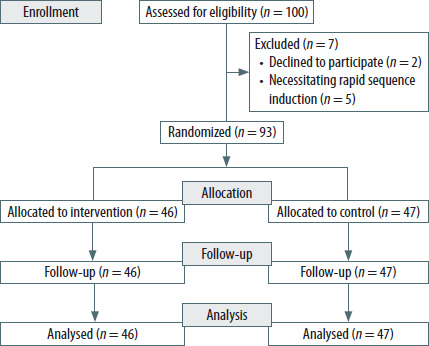
Between February 1, 2023, and December 25, 2023, a total of 100 adult patients who were sche- duled for elective surgery under GA and required oral tracheal intubation participated in the study. Following the exclusion of seven patients from the study, data analysis was conducted on 93 par- ticipants, with 46 assigned to the SL group and 47 to the GL group (Figure 2).
Demographic and baseline characteristics
The average age of participants in the SL and GL groups was 41.30 ± 12.19 and 41.16 ± 7.15 years.
The hemodynamic status of patients in both groups, as indicated by HR and mean arterial pres- sure (MAP), showed comparable stability through- out the intubation procedure, with no significant differences (P = 0.2; 0.12, respectively). The average thyromental distance of individuals in the SL and GL groups was 3.86 ± 1.30 and 5.30 ± 0.59 cm re- spectively. Furthermore, the thyromental heights were 5.44 ± 0.50 and 4.26 ± 0.90 cm for the GL and SL groups, respectively, which were both signifi- cantly lower in the SL group (P < 0.0001).
Glottic visualization
Based on the CL score, glottic visualization was compared between the two groups, and no signifi- cant difference was found (P = 0.21) (Table 1).
TABLE 1
Comparison of basic variables between the two groups
Intubation outcome
The SL group had a considerably higher first attempt success rate of tracheal intubation than the GL group (93.4% vs. 85.2%; P = 0.002). The mean intubation time was also notably shorter for the SL group, averaging 29.28 ± 8.00 seconds, in compari- son with 42.73 ± 15.50 seconds for the GL group (P ≤ 0.0001) (Table 2).
TABLE 2
Association between the time of intubation and different variables in multiple logistic regression
Correlation with intubation time
The association between some variables (age, sex, mouth opening, thyromental height, and distance) and intubation time was investigated, using multiple linear regression analysis. The intubation time and these factors were found to be negatively correlated. In particular, the intubation duration decreased by an average of 0.55 seconds for every year of increasing age. Furthermore, male patients required 7.26 seconds less intubation time than fe- male patients. Reductions in intubation duration of 2.51, 3.11, and 11.25 seconds were linked to in- creases in mouth opening, thyromental height, and thyromental distance, respectively (Table 3).
TABLE 3
Comparison of outcomes via study groups
DISCUSSION
In this study, 93 patients who fulfilled the crite- ria for an expected difficult intubation during the induction of anesthesia were assessed for the per- formance of the SL and the GL. The identified criteria for difficulty in intubation in these patients includ- ed limitations in neck extension and mouth open- ing, Mallampati score III/IV, thyromental distance and thyromental height of approximately less than 5 cm.
Although both groups met the criteria for dif- ficult intubation, the intubation was more challeng- ing in the SL group because both the thyromental distance and height measurements were less than 5 centimeters, which is a cut-off reported in pre- vious studies [10, 11]. This revealed that the SL group was more challenging than the GL group. However, the SL group achieved significantly better outcomes in terms of duration of intubation and success rate on the first attempt compared to the GL group.
Visualization of the glottis is a crucial aspect for achieving successful tracheal intubation in difficult airways. While tracheal intubation will be success- ful on the first laryngoscopy attempt in cases of CL scores equal to or less than 2, cases of CL scores over 3 will require laryngeal or bogie manipulation in or- der to achieve tracheal intubation. The glottic visu- alization was similar for both laryngoscope types, but the success rate was greater, and the intubation duration was shorter for the SL group, which is con- sistent with SL’s advantage over GL.
Previous studies have documented a 94% first attempt success rate for intubation with SL in pa- tients with normal airways [8, 9]. While the present study found this measure to be 93.4% for patients with difficult airways, this still confirms the high ef- ficacy of SL in this subgroup of patients. Consistent with these findings, other studies have obtained success rates of 80–90% for first-attempt tracheal intubation with GL in patients with a known difficult airway [12, 13]. These results collectively suggest that both SL and GL can achieve high success rates for intubation, with SL potentially offering a slight advantage, particularly in patients with difficult air- ways. However, further research is needed to fully elucidate the comparative performance of these laryngoscope types across different patient popu- lations and airway conditions.
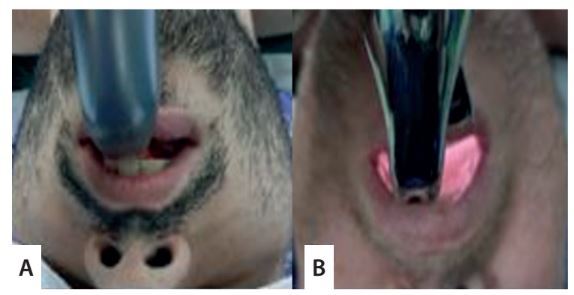
Patients with low thyromental height and dis- tance have a larynx that is in the front and upper neck, out of the laryngoscope blade’s reach. It will also be challenging to see the glottis and insert the tracheal tube through it, making this type of in- tubation situation difficult. Given that both groups’ glottis visualizations were the same, as shown in this study, the rationale for SL’s higher success rate in tra- cheal intubation may be attributed to the device’s blade design, which differs from that of the GL.
FIGURE 3
Posterior view of the blade of the GlideScope (A) and the Sanyar video laryngo-scope (B) after entering the mouth

The spoon-shaped blade surface of the SL, which is inclined around 11 degrees to the left, makes it easy to guide the tongue to the left side of the mouth. Additionally, there is a 10 mm gap be- tween the body of the laryngoscope and its blade, which will create a free space that is suitable for the tracheal tube to pass through. A skilled opera- tor can pass the tube very easily through this space until the tip is positioned in front of the glottis (Fig- ure 3). Thus, tracheal intubation will be performed swiftly on the first try.
The study utilized a multiple linear regression model to examine the correlation between various factors (age, female sex, mouth opening, thyromen- tal distance, and thyromental height) and intuba- tion time. The analysis revealed a negative relation- ship between these factors and intubation time, after adjusting for other variables. The diffe rence in intubation speed between these two groups may be attributed to the duration required to find the glottis and insert the tube from the oral cavity to the glottis. Hoshijima et al. [14] reported that the duration of tracheal intubation using a Glide- Scope ranged from 31 to 88 seconds in patients with predicted difficult airways. Of course, it should be noted that, aside from laryngoscope design is- sues, the proficiency of the operator in utilizing these devices will also impact the success rate and speed of intubation [15].
This study has certain limitations. Due to the study’s design and use of two distinct VLs, it was not possible to blind the operator; nonetheless, an independent individual in both groups objec- tively documented the final outcomes, including the glottic view, intubation time, and intubation success. Despite this limitation, the present trial is the first attempt to academically assess the SL un- der anticipated difficult airway circumstances, in contrast to a standard method.
CONCLUSIONS
The study concludes that the SL demonstrates superior performance compared to the GL in mana- ging difficult airways. The SL achieved a higher first- attempt success rate and shorter intubation time, indicating its effectiveness in enhancing patient safety and outcomes during anesthesia. These find- ings support the recommendation for using ad- vanced VL techniques, particularly in patients with anticipated difficult intubation, while highlighting the need for further research to explore the perfor- mance of these devices across various clinical sce- narios.