
Elective surgery is one of the most common causes of hospitalization in Poland and around the world. It is estimated that approximately 300 mil-lion surgical procedures are performed annually worldwide, and this number is steadily increasing [1].
At the same time, according to some sources, the rate of postoperative complications can reach up to 60% [2]. For this reason, one of the main therapeutic goals of modern anaesthesiology and periope-rative medicine is not only preparation for surgery and anaesthesia, but also to improve postoperative care that allows the patient to recover as quickly as possible and return to pre-hospitalization activities.
The comprehensive evaluation of postoperative convalescence requires consideration beyond mere clinical parameters, incorporating patient-reported outcomes (PROs). Applying PROs in clinical practice provides a holistic view on the patients’ symptom severity, general health and recovery [3]. However, despite the importance of PROs, they are frequently not reported in clinical trials [4]. Questionnaires are an important tool enabling PROs evaluation and promoting consistency in the evaluation process.
An example of such a self-reported survey is the Quality of Recovery-15 (QoR-15) questionnaire, which is a tool recommended by the European Society of Anaesthesiology and Intensive Care (ESAIC) [5]. It consists of 15 questions about the patient’s condition, and should take less than 5 minutes to complete, being convenient for both patients and healthcare providers [6]. The result of the QoR-15 is a numerical score between 0 (very poor recovery) and 150 (extremely good recovery). In addition to its ease of use and interpretation, it has scientifically demon-strated reliability, consistency and relevance and thus is widely used as an endpoint in high-quality clinical trials [7, 8].
The questionnaire has been validated in seve-ral languages, including Chinese, French, Korean and Swedish [9–12]. To date, however, the Polish language version of the questionnaire has not yet been validated. Translation and adaptation of the QoR-15 questionnaire for a Polish-speaking population would improve the assessment of postoperative recovery and enable the questionnaire score to be used as an endpoint in clinical trials in surgery and perioperative care.
The aim of the study was to validate the QoR-15 questionnaire in the Polish population.
Methods
Ethics
The project received a positive opinion from the Bioethics Committee of the Jagiellonian University in Cracow, Poland (Chairperson Prof. D. Dudek) on June 16, 2021 (no. 1072.6120.141.2021).
Translation
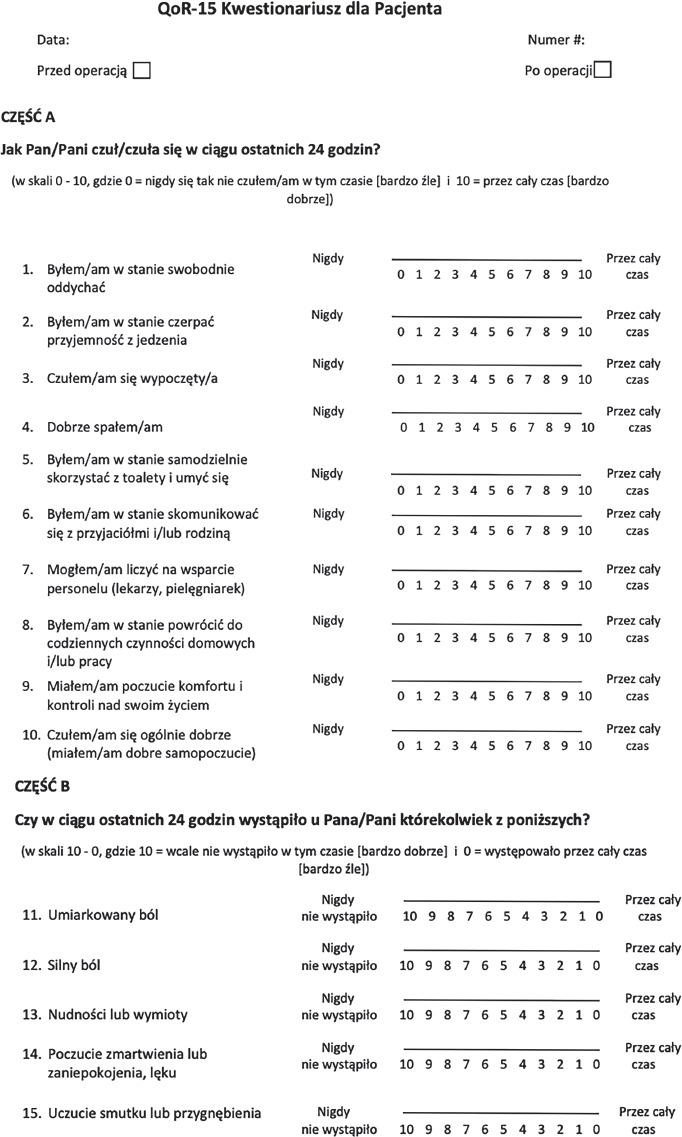
The translation process was conducted by two independent researchers with professional translation skills and appropriate medical knowledge, followed by the development of the final Polish version (QoR-15PL) by a third researcher, leveraging previously prepared translations. No specific cultural adaptations were necessary. The QoR-15PL questionnaire was subsequently validated through a pilot study involving 10 patients. The final version of QoR-15PL is presented in Figure 1.
Inclusion and exclusion criteria
The recruitment took place in the anaesthesio-logy outpatient clinic and/or hospital ward before the scheduled procedure. Patients aged over 18 years undergoing a surgical procedure with planned general anaesthesia were considered eligible for the study. The exclusion criteria were as follows: anticipated inability to complete the questionnaire after surgery (e.g., high probability of stay in intensive care unit), lack of proficiency in the Polish language, mental and/or cognitive disorders that significantly impeded cooperation with the researcher. Moreover, patients who had not completed postoperative questionnaires were excluded. Informed written consent was obtained from each patient willing to participate in the study.
Data collection
The study was conducted in 5 Polish hospitals from 22.01.2023 to 7.05.2023. The participants were asked to complete the QoR-15PL questionnaire with the assistance of the researcher, who verbally presented the questions, on two occasions pre-operatively and on the first day after surgery. Approximately one in five patients was asked to fill in the questionnaire again approximately 30 minutes after the initial postoperative survey, with the aim of evaluating the internal consistency of QoR-15PL. The 100-mm Visual Analogue Scale (VAS), ranging from ‘the worst possible health one can imagine’ to ‘the best possible health one can imagine’ was introduced pre- and postoperatively as well. In line with the original QoR-15 validation study, patients with postoperative VAS < 70 were considered to have poor recovery [11]. Moreover, comprehensive data regarding patients’ clinical characteristics, surgical procedure and postoperative complications were obtained from medical records. The Clinical Frailty Scale (CFS) and American Society of Anesthesiologists Classification (ASA) were applied to assess each patient. Each procedure was assigned to one of three risk groups according to 2022 European Society of Cardiology (ESC) guidelines on non-cardiac surgery [14]. Information about surgery duration, length of post-anaesthesia unit stay, and hospital stay length were also collected. Patient observation extended until hospital discharge, with a follow-up telephone visit conducted 30 days post-procedurally, involving another questionnaire collection and a short interview about postoperative recovery and complications.
Statistical analysis
Descriptive statistics were employed for charac-terization of the study population, with results presented as the mean with standard deviation (SD) or as the median with interquartile range (IQR). Normality of distribution was assessed using the Shapiro-Wilk test. The comparison of preoperative and postoperative results was conducted using the Wilcoxon signed-rank test. Associations were evaluated using the Spearman rank correlation coefficient. The Kruskal-Wallis test or Mann-Whitney U test was used to establish the differences between the groups. Validity was evaluated by exploring the correlation between QoR15-PL and another self-reported health assessment tool – the 100-mm VAS. Additionally, associations with perioperative factors potentially influencing recovery were established. The reliability of QoR-15PL was assessed through internal consistency, split-half reliability, and test-retest reliability. Internal consistency was examined using Cronbach’s a and Guttman’s Lambda 6, while test-retest reliability was appraised using the intra-class correlation coefficient (ICC). Responsiveness was tested through establishing Cohen’s effect size and the standardized response mean (SRM). Presence of floor or ceiling effects was acknowledged if more than 15% of participants reported either the highest or lowest possible score. The null hypothesis was rejected if two-tailed P < 0.05.
All analyses were performed using RStudio (version 1.3.1093) and IBM SPSS Statistics for Macintosh (Version 29.0).
Results
A total of 426 patients were enrolled in the study and completed a preoperative questionnaire. Among them, 342 patients (52.6% females) successfully filled in both preoperative and postoperative questionnaires and were consequently included in the analysed cohort, resulting in the completion rate of 80.3%. 185 patients (54%) participated in a 30-day follow-up.
Demographic and clinical characteristics of patients are presented in Table 1. The perioperative characteristics are shown in Table 2. Early periprocedural complications occurred in 23.2% of the patients, with major bleeding being the most common complication.
TABLE 1
Baseline characteristics of enrolled population (N = 342)
TABLE 2
Perioperative characteristics and periprocedural complications (N = 342)
Validity
Significant correlations between the preoperative and postoperative QoR-15PL scores and the corresponding VAS scores were observed: r = 0.58, P < 0.001 and r = 0.6, P < 0.001, respectively. Patients with poor recovery defined as VAS score < 70 mm had distinctly lower median QoR-15PL scores than those with good recovery (VAS ≥ 70 mm): 100 ± 27 vs. 126 ± 28.5, P < 0.0001. Men obtained a higher median postoperative QoR-15PL score compared to women: 116 ± 24 vs. 109 ± 26 (P = 0.009). No statistically significant relationship with age, ASA (American Society of Anesthesiologists) physical score or ESC (European Society of Cardiology) surgical risk was found. A negative association between the postoperative score and duration of stay in post-anaesthesia care unit (r = –0.17, P = 0.003) and general length of stay in the hospital (r = –0.17, P = 0.002) was observed, although the correlation was weak. The analysis did not detect any substantial association between postoperative complications and the postoperative questionnaire score.
23.2% of patients experienced adverse events, the majority of which were minor and transient, including nausea (n = 8), prolonged sedation (n = 10) and events related to blood pressure in the intraoperative period (n = 39), which may account for the observed outcomes.
The Cronbach’s a values for inter-dimension reliability indicated good internal consistency of QoR15-PL across all the time points. Notably, values for pre-operative and postoperative questionnaires were 0.85 and 0.86, respectively. The favourable outcomes were corroborated by Guttman’s Lambda 6 values and average split-half reliability, further emphasizing the commendable reliability. The detailed statistics are presented in Table 3. The test-retest reliability, as indicated by the intraclass correlation coefficient (ICC), was 0.91 (95% CI: 0.85 to 0.94, P < 0.01) for total score, based on a sample size of 76 patients.
TABLE 3
Internal consistency assessment
Responsiveness
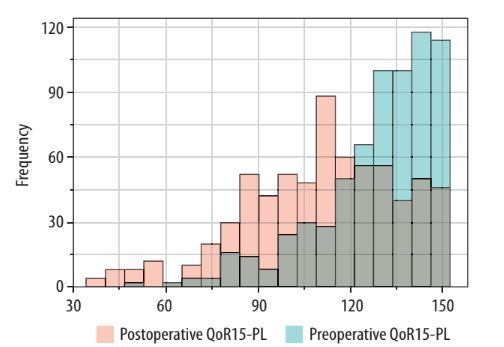
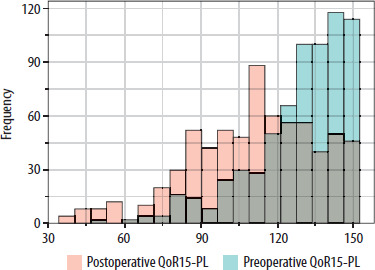
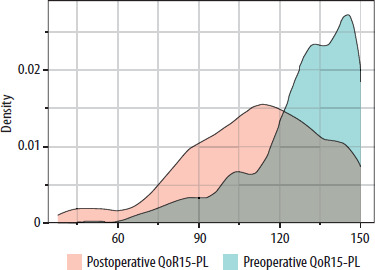
Both indicators of responsiveness calculated for total score showed satisfactory results, featuring a Cohen’s effect size of 0.78 (95% CI: 0.62 to 0.93) and a standardized response mean of –0.65 (95% CI: –0.75 to –0.54). QoR-15PL total score significantly decreased postoperatively, from 132 (IQR 121 to 143) at baseline to 113 (IQR 95 to 129) on the first post-surgery day (P < 0.001). Subsequently, the score increased again at the 30-day follow-up to 141 (IQR 132 to 147), with a significant difference compared to the postoperative score (P < 0.001). Histograms and density plots for comparing pre- and postoperative QoR-15PL results are presented in Figures 2 and 3. No floor or ceiling effect was observed – no participant reported the lowest possible score for both pre- and postoperative questionnaires, while the highest was observed for 26 (7.6%) and 9 (2.6%) patients, respectively.
Discussion
The study was the first project aimed to validate the Polish version of the QoR-15 questionnaire. The analysis confirmed the high psychometric values of the questionnaire, and thus its potential utility in assessing the quality of recovery in patients after elective surgery in the Polish population. Demographic and medical characteristics indicated a balanced representation of patients, contributing to the generalizability of the results. Therefore, the Polish version of QoR-15 can be successfully used as a valuable tool in everyday clinical practice, as well as a research tool.
In terms of construct validity, a weak negative association was observed between postoperative scores and durations of stay in the post-anaesthesia care unit and the overall hospital stay. Consistent with the original QoR-15 version and several other validation studies, no correlation between age and questionnaire results occurred, likely attributable to the tendency of older individuals to underreport their discomfort [15]. The observed sex-based differences align with existing knowledge, indicating that women typically face a more challenging postoperative recovery [18].
No substantial association was identified between postoperative complications and the post-operative QoR-15PL score, possibly reflecting the low occurrence of significant adverse events in the study cohort. Furthermore, individuals experiencing swift and uncomplicated recovery were occasionally discharged in the morning following the surgery without completing the second questionnaire, leading to their exclusion from the analysis (n = 84) and thus creating a potential bias.
Convergent validity tested by comparing the QoR-15PL score with the corresponding global VAS score was moderate and consistent with other studies [10, 17–19]. In the psychometric evaluation of the original QoR-15 version, the arbitrary categorization of patients into groups of good or poor recovery based on global VAS scores was performed in order to examine the discriminant validity. This approach, while revealing a significant difference in QoR-15PL scores between the defined groups, warrants consideration, as it is worth acknowledging that relying solely on VAS scale outcomes in such classifications may inadvertently undervalue the nuanced and multifaceted nature of actual patient experiences during the recovery process.
In terms of reliability, all of the internal consistency measures demonstrated high values exceeding the established recommendations [17]. The test-retest reliability indicated by the ICC was excellent, aligning with outcomes reported in previous investigations. The 30-minute time interval between the questionnaires, chosen based on the original QoR15 validation study, aimed to minimize the likelihood of patients recalling their earlier responses while being short enough to prevent substantial changes in postoperative recovery.
The responsiveness assessment involved comparing pre- and postoperative total scores and calculating Cohen’s effect size and the SRM. The QoR-15PL had an effect size of 0.78 and SRM of –0.65. The obtained Cohen’s d value suggests a meaningful difference between the scores, and even though it is lower than in most validation studies, it is still at a satisfactory level, as d > 0.8 is considered a large effect size [10, 20–22]. Some studies did not report Cohen’s d value, as Cliff’s effect size was chosen instead. However, the authors believe that the difference between the total score better reflects the overall impact on the construct than calculating the effect size for each questionnaire item separately.
An SRM of –0.65 suggests a moderate to large negative response, lower than in several validation studies. However, the original QoR-40 scale has exactly the same value [10, 23, 24]. The negative sign reflects the decrease in postoperative score.
The study has several limitations. The loss of patients occurred mainly for organizational reasons-patients in good condition were often discharged early the morning of the day after surgery, before the questionnaire was collected again. Among the remaining participants, there were no refusals to continue participating in the study. Another limitation of the study is the reliance on the VAS as the sole measure to assess the validity of the QoR-15. While the VAS is a widely used general health measure, it is not specifically designed to evaluate postoperative recovery. Additionally, the presence of a researcher while patients completed the questionnaires may have influenced the responses. Future studies should consider replicating this research with patients self-completing the QoR-15 independently, without any external assistance, to ensure the authenticity and reliability of the responses.
Conclusions
The QoR-15PL scale is a reliable and effective tool for assessing the quality of recovery reported by patients after surgery and general anaesthesia within the Polish-speaking population. The measurement characteristics of the QoR-15PL scale align well with the original version and other translated iterations, supporting its applicability in both clinical practice and research.