

Dear Editor,
Epidermal necrolysis (EN) is a collective term currently used to delineate Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) [1]. EN is an extremely rare disease with an annual incidence of 0.0002% [1, 2]. It is a devastating immune-mediated skin and mucous membrane disease with a mortality of around 35% [1, 2]. It is characterized by a widespread vesiculopustular rash with epidermal sloughing and necrosis. EN is categorized into SJS and TEN based on the involvement of the total body surface area (TBSA). If TBSA involvement is less than 10%, then it is called SJS, and if TBSA is more than 30%, it is called TEN. TBSA between 10 and 30% is labeled as SJS-TEN overlap [1]. EN usually occurs as an idiosyncratic reaction to medications (antiepileptics, antibiotics, nonsteroidal anti-inflammatory drugs, etc.), vaccination or some viral infection. In a minority of cases, no determinant can be identified [1, 2]. Depending on the severity of the disease, the patient can have ocular, oral, otorhinolaryngological, respiratory, gastroenterological, and genitouri-nary manifestations [1–3]. Intensivists usually encounter a case of SJS-TEN during its pulmonary complications. Recently, we observed a case of acute respiratory failure associated with SJS-TEN overlap.
This manuscript was approved by the director of our department, and we obtained consent from the patient for publication of this case report. Our patient was a 26-year-old male with no known comorbidities. He was admitted to our hospital following a road traffic accident leading to degloving injury to his left foot (Figure 1A). On admission, he underwent wound exploration and debridement. Over the next ten days, he underwent three further episodes of wound inspection and debridement.
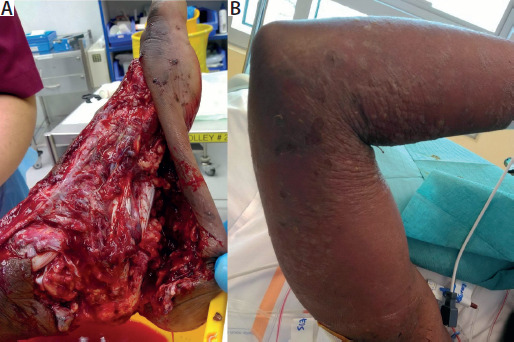
His hospital course was complicated by surgical site wound infection by Escherichia coli and Enterococcus faecium. He was switched to piperacillin-tazobactam and vancomycin antibiotics. In addition, he received paracetamol for analgesia and enoxaparin for thromboprophylaxis. Five days after starting antibiotics, he developed high-grade fever and erythematous vesiculobullous rash (Figure 1B) on his face, lips, oral mucosa, upper chest, and bilateral upper limbs (approximately 30% TBSA). He was referred to a dermatologist. A skin biopsy was taken. He was started on intravenous steroid (hydrocortisone) and fusidic acid-hydrocortisone local application on skin lesions. We reviewed his drug chart and calculated the Algorithm of Drug Causality for Epidermal Necrolysis (ALDEN) score for each administered drug [4] (Table 1). From the ALDEN score, the most probable culprit drug for EN was piperacillin-tazobactam (score 6) followed by vancomycin (score 4). Antibiotics were modified, piperacillin-tazobactam and vancomycin were stopped and he was started on tigecycline. In the subsequent 48 hours, his skin lesions showed evidence of epidermal sloughing. The patient also developed respiratory distress. He was referred to an intensivist for hypoxic respiratory failure. On auscultation, there were fine inspiratory crackles. His chest X-ray was suggestive of bilateral asymmetrical consolidation. He was intubated and mechanically ventilated. During intubation, we noticed oral mucosal ulceration and sloughing. His ventilator data/mechanics were suggestive of low lung compliance. His computed tomography of the chest was suggestive of bilateral consolidations and ground glass opacities (Figure 2). His ventilatory parameters were managed according to our institutional adult respiratory distress syndrome (ARDS) protocol. The steroid hydrocortisone was changed to methylprednisolone 1 mg kg-1 day-1 as a continuous infusion. Results from the histopathological investigation of the skin were consistent with EN (subepidermal bullae with necrosis of the epidermis and scattered necrotic keratinocytes). Bronchoscopy was performed, suggesting diffuse nonspecific inflammatory changes in the tracheobronchial tree. Bronchoalveolar lavage was negative for culture. Subsequent to the histo-pathological diagnosis of EN, in addition to steroids, we added intravenous immunoglobulins (Privigen) 1 g kg–1 day–1 as a continuous infusion for three days. The patient showed a remarkable response to the above regimen. His oxygenation improved, and he was extubated on the tenth day after ICU admission. After extubation, his methylprednisolone was changed to oral prednisolone, which was tapered over the next five days. His skin lesions were also abated. After his wound infection was cleared, his left foot wound was covered with a free latissimus dorsi flap and skin graft. The postoperative course was uncomplicated, and he was discharged from the hospital on the sixteenth postoperative day.
TABLE 1
Calculation of algorithm of drug causality for epidermal necrolysis score [4]
1: 5 to 28 days (score of 3), 29 to 56 days (2), 1 to 4 days (1), more than 56 days (–1), index day (–3).
3: Stevens-Johnson syndrome/toxic epidermal necrolysis (4), Stevens-Johnson syndrome/toxic epidermal necrolysis to a similar drug (2), other reaction to same or similar drug (1), none (0), previous use without reaction (–2).
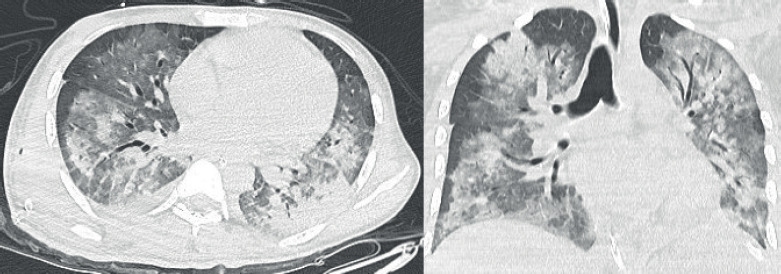
FIGURE 2
Computed tomography scan of chest showing bilateral pulmonary consolidation with ground glass opacities
Acute and chronic pulmonary complications are reported in EN [3]. The development of pulmonary complications in EN is a negative prognostic factor, resulting in a mortality of around 50–60% [2, 3]. The lung injury in EN is caused by bronchial mucosal apoptosis-necrolysis and the release of cytokines and inflammatory mediators from the skin [3]. The frequently noticed acute pulmonary complications are bronchitis, bronchiolitis obliterans, pneumonia, atelectasis, pulmonary edema, ARDS and pleural effusion [2, 3]. Occasionally, some patients after EN can develop chronic pulmonary complications such as bronchiolitis obliterans organizing pneumonia, chronic obliterative bronchitis, bronchiectasis, interstitial lung disease and obstructive pulmonary disease [2, 3].
Patients with EN are often referred to the ICU for respiratory support. There are several implications for giving respiratory support to these patients. Theoretically, the airway can be considered difficult due to the deve lopment of disease-specific lesions, mucosal slogging and edema in the oral cavity or upper airway [3]. Indications for mechanical ventilation (MV) are described in EN management guidelines, and intensivists can employ standard indications while initiating MV [3]. Endotracheal tube (ET) fixation can be troublesome due to the skin lesion. A specialized ET tube fixation device is advisable to preserve the airway [2, 3]. There are no specific guidelines about ventilatory management. The clinical course of these patients is similar to other ARDS patients [3]. Intensivists can follow their local institutional ARDS management protocols. Bronchoscopy, if feasible, is routinely required to determine involvement of the airway mucosa. Bronchoscopy is also helpful in clearing the small airways from mucosal slough [3]. Management includes identification and discontinuation of the offending agent/drug, systemic and local steroids and intravenous immunoglobulins (IVIG) [1, 5, 6]. IVIG subdues the type IV hypersensitivity reaction and cell apoptosis. Indications for IVIG include TBSA involvement of more than 10% or mucosal involvement, preferably after confirming the diagnosis by skin biopsy [5, 6]. The recommended dose of IVIG is 0.5–1 g kg–1 day–1 for 3–5 days [5, 6]. Although IVIG alone or in combination with steroids does not have mortality benefits, it helps in reducing the disease duration and severity and systemic complications [6]. IVIG is contraindicated in renal failure [5]. The role of TNF-alpha inhibitors, cyclosporin and plasmapheresis remains unknown [1].
In conclusion, severe EN is a dermatological emergency with a mortality rate of around 35%. Some patients develop systemic complications. The development of pulmonary complications will increase mortality by twofold. Intensivists are usually consulted to provide respiratory support. The multiple implications of providing respiratory support should be considered by intensivists. Management essentially includes discontinuation of the offending agent, steroid and immunoglobulins.