
In the era of multimodal anesthesia, magnesium sulfate (MgSO4) has proven to be an important adjuvant in the anesthetic arsenal due to its properties and substantial synergistic effects with other drugs commonly used in anesthetic practice, highlighting its effect on NMDA (N-methyl-D-aspartate) receptors, contributing to analgesia, reducing arousal and preventing chronic pain when used at high doses in intravenous infusion [1, 2].
Because of these properties, it has an important role in reducing the consumption of some anesthetics, such as opioids, in the intraoperative and postoperative period, and consequently avoiding their adverse effects, such as nausea, vomiting, respiratory depression, hyperalgesia, and possibly significant changes in the immune system [1, 2].
However, due to its effects on the neuromuscular junction, there are reports of dose-dependent residual neuromuscular block when combined with neuromuscular blockers intraoperatively and immediately after general anesthesia [3–5]. High plasma concentrations of magnesium inhibit the release of acetylcholine from the presynaptic nerve terminal and potentiate the effect of neuromuscular blocking agents (NMBs) [4, 5]. Nevertheless, there are limited data on the usual dose of rocuronium, safety concerns, and pharmacodynamic properties when combined with a single dose of MgSO4 for general anesthesia as an adjuvant to multimodal anesthesia.
This study aims to evaluate the influence of MgSO4 at a dose of 30 mg kg–1 as a single injection on the pharmacodynamic characteristics of rocuronium in patients undergoing total intravenous general anes thesia.
Primary outcome: Influence of MgSO4 on latency (onset time) measured as the time in seconds from the start of injection of rocuronium until 95% depression of the first twitch (T1) of the TOF [6]; clinical duration (CD25%) – the time in minutes (min) from the start of injection of rocuronium until T1 of the TOF had recovered to 25% of the final T1 value; and recovery time of 90% of T4/T1 – train of four (TOF = 0.9) [6].
Secondary outcomes: Clinical conditions of tracheal intubation [7]; hemodynamic repercussions of laryngoscopy and tracheal intubation maneuvers, assessed at different time points: control – before intervention; M1 – pre-induction; M2 – post-induction and pre-tracheal intubation (TI); and M3 – one minute post-TI. Consumption of propofol and remifentanil intraoperatively; duration of surgery, duration of anesthesia, time to recovery of consciousness, consumption of opioids during hospitalization in the post-anesthetic care unit (PACU); length of stay (LOS) in the PACU.
METHODS
This randomized study was conducted in a tertiary hospital in Campinas, Brazil. The study protocol was approved by the local Research Ethics Committees (Campinas – SP, Brazil Ref: CAAE 50852714. 7.0000.5404) and registered in the Brazilian Registry of Clinical Trials (ReBEC-U1111-1253-2766, RBR-79j38k).
The present study is a prospective, randomized- controlled, parallel, two-arm, double-blind clinical trial, following the CONSORT (Consolidated Standards of Reporting Trials) specifications. After obtaining written informed consent, 70 female patients, ASA (American Society of Anesthesiologists) physical status 1 and 2, undergoing abdominal gynecological surgery (open hysterectomies) under general anesthesia, were included in the study. The inclusion criteria were: patients with ASA physical status 1 and 2, undergoing general anesthesia using NMBs. Non-inclusion criteria were: neuromuscular, hepatic or renal diseases, hydro-electrolytic or acid-base disorders, difficult airway (Mallampati III and IV), gastroesophageal reflux, peripheral temperature lower than 32ºC and BMI > 35 or < 18.5 kg m–2.
Study protocol
Following the strategy of simple randomization (1 : 1) and respecting the confidentiality of allocation, the research subjects were distributed into two groups, using sealed brown envelopes, according to whether or not they would use MgSO4 (30 mg kg–1), based on a computer-generated list of random numbers: Group 1 (MgSO4) and Group 2 (saline).
All anesthetic procedures were performed by one of the two anesthesiologists participating in the study (C.J.R. and A.F.A.B.) and data was collected by the principal investigators (V.H.C. and G.B.). Members of the research team who were in the operating room (OR) were unaware of the randomization of the group, as well as of the intervention, since both disposables were identical and had been previously prepared by (A.P.C.F.) outside the OR.
On admission to the operating room, venous access was made with an 18G intravenous cannula to administer fluids and drugs. In the operating room, they were continuously monitored with a cardio monitor, pulse oximeter, non-invasive blood pressure monitor, capnograph, bispectral index, thermometer and neuromuscular junction monitor (TOF-GUARD). The subjects were fasting, and the pre-anesthetic medication was midazolam at a dose of 1 to 3 mg intravenously 5 min before entering the operating room. Group 1 was given MgSO4 (30 mg kg–1) at a maximum dose of 2 g, diluted in 100 mL of 0.9% saline 10 min before induction of anesthesia and Group 2 was given 100 mL of 0.9% saline without MgSO4. This MgSO4 infusion 10 min before induction can be justified by the fact that the effect of the magnesium ion on the neuromuscular end-plate is both concentration- and time-dependent. A bolus injection cannot reach the motor nerve terminal in a concentration that could interfere with rocuronium. Also, an in vitro study showed that 4 to 6 min were necessary to establish a new frequency of miniature end-plate potentials after administration of increasing magnesium concentrations [6].
The general anesthesia technique used was the same in both groups. During induction of anesthesia, sufentanil (0.3 μg kg–1), propofol (1.5 to 2.5 mg kg–1) and rocuronium (0.6 mg kg–1) were injected over 5 seconds. Patients were ventilated under a mask with 100% oxygen until a 75% reduction in the amplitude of the evoked muscle response to isolated stimulation was achieved, at which point laryngoscopy and tracheal intubation maneuvers were performed and assessed. Anesthesia was maintained with continuous infusions of propofol and remifentanil in controlled target pumps and a mixture of O2 and air (50%). Ventilatory parameters were adjusted to maintain expired CO2 (PETCO2) between 30 and 33 mmHg. The skin temperature over the thenar region was monitored continuously and kept between 30 and 32ºC.
To assess neuromuscular transmission and the pharmacodynamic characteristics of rocuronium, a TOF-Guard monitor (Organon, Swords Co., Dublin, Ireland) was used. The surface electrodes were installed in the path of the ulnar nerve, at wrist level on the side contralateral to the patient’s motor dominance, and the acceleration transducer (piezoelectric) was attached to the distal phalanx of the thumb of the limb under study. The “control” muscle response was obtained through isolated supramaximal stimuli (1 Hz) for 3 min after induction of anesthesia. After the administration of rocuronium, neuromuscular function was monitored continuously with a sequence of 4 TOF stimuli until the neuromuscular variables were fully assessed. T4 : T1 = 0.9 (90%).
The procedures for setting up, calibrating and stabilizing the neuromuscular monitoring followed Good Clinical Research Practice in pharmacodynamic studies of NMB agents [8].
Data collection
Patients were identified by numbers, and data was collected in the operating room of the Hospital Prof. Dr. José Aristodemo Pinotti – CAISM – UNICAMP. The data were collected by one of the researchers inside the operating room, where there was another anesthesiologist responsible for patient care, and later in the PACU.
Data processing
The information contained in the forms was typed up and stored in a database. The distribution frequencies and the medians of the control variables in both groups were analyzed to check their comparability. The dependent variables were then statistically analyzed.
Statistical analysis
To calculate the sample size, we used the data obtained by Czarnetzki et al. [6] regarding the effects of MgSO4 on the clinical duration of rocuronium. In the absence of MgSO4, the clinical duration was 33.2 ± 8.1 min versus 44.7 ± 14 min in subjects exposed to MgSO4. To detect a 50% difference in the increase in clinical duration (44.7 – 33.2/2 = 5.75), with a significance level of 5% (a error) and a power of 80% (b), the number of subjects needed in each group was 31. Thus, 70 patients were included in the study (margin of approximately 10%), distri buted into two groups according to whether or not MgSO4 was used.
The c2 or Fisher’s exact test was used to analyze and compare categorical variables between the two groups. The Mann-Whitney test was used to compare numerical variables, due to the lack of normal distribution of the variables. The data are presented as mean, SD, minimum, median, maximum and quartiles 1 and 3.
The significance level adopted for the statistical tests was 5% (P < 0.05), with a statistical power of 80%. For the statistical analysis, the following computer program was used: SAS for Windows (Statistical Analysis System), version 9.2. SAS Institute Inc, 2002-2008, Cary, NC, USA.
RESULTS
All 70 patients were enrolled and randomized between August 2020 and October 2021. All of them were analyzed according to the protocol. No patients were lost to follow-up.
The MgSO4 and saline control groups were well compared for baseline characteristics (Table 1).
TABLE 1
Characteristics and pre-operative data of patients receiving magnesium sulfate (MgSO4) or saline. Values are median (IQR [range]) or number (proportion)
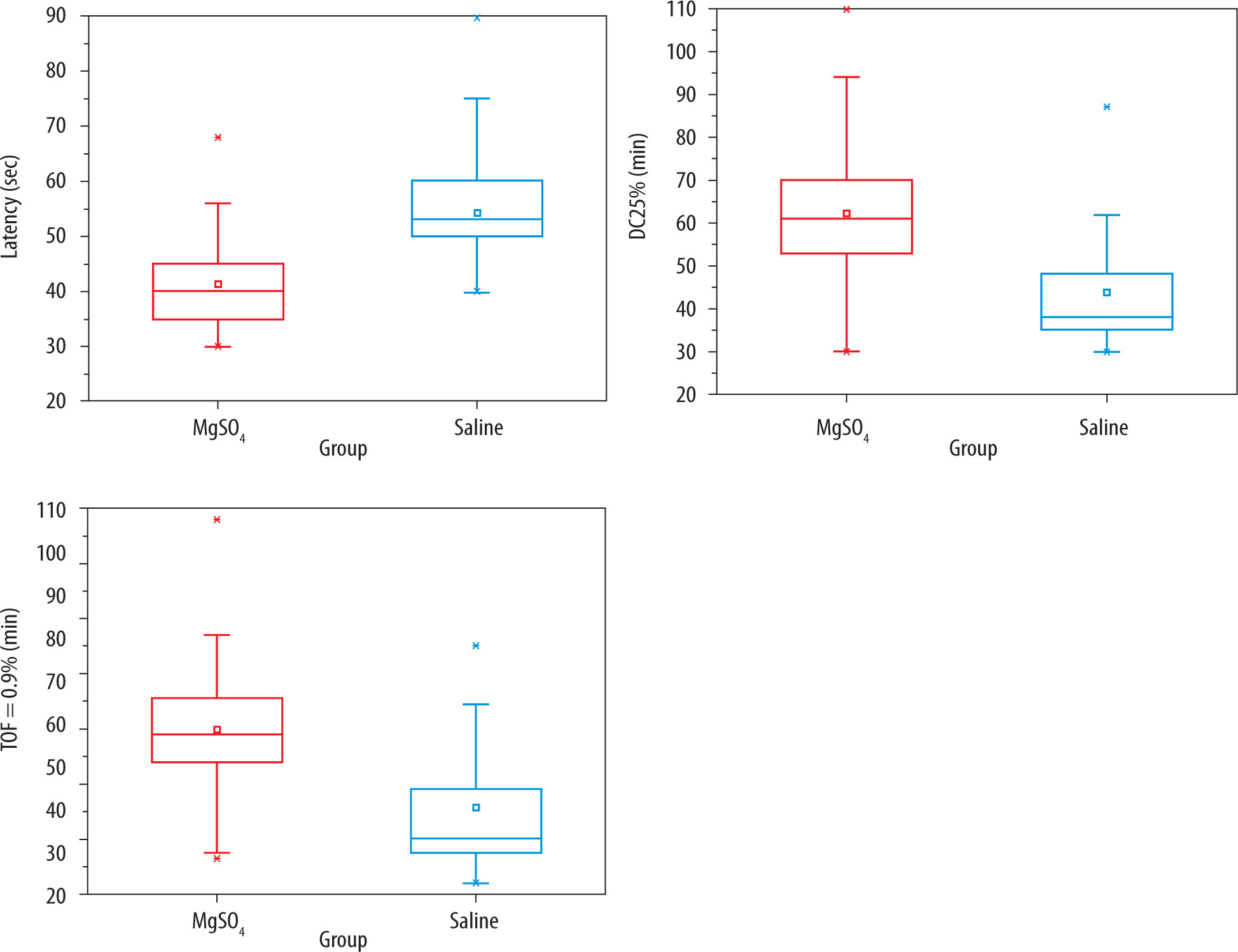
A comparative analysis showed a statistically significant difference between the groups regarding latency (lower in the MgSO4 group, 40.00 (35–45 [30–68]) compared to saline, 53.00 (50–60 [40–90]) (P < 0.001), CD25% (higher in MgSO4, 61.00, compared to saline, 38.00 (35–48 [30–87]) (P < 0.001), and TOF = 0.9 longer in the MgSO4 group, 98.00 (88–111 [53–176]) compared to saline, 60.00 (55–78 [44–130]) (P < 0.001) (Table 2).
TABLE 2
Influence of magnesium sulfate (MgSO4) in the pharmacodynamic characteristics of rocuronium. Values are median (IQR [range])
Figures 1 and 2 (boxplots) illustrate the analysis of the values observed for these variables.
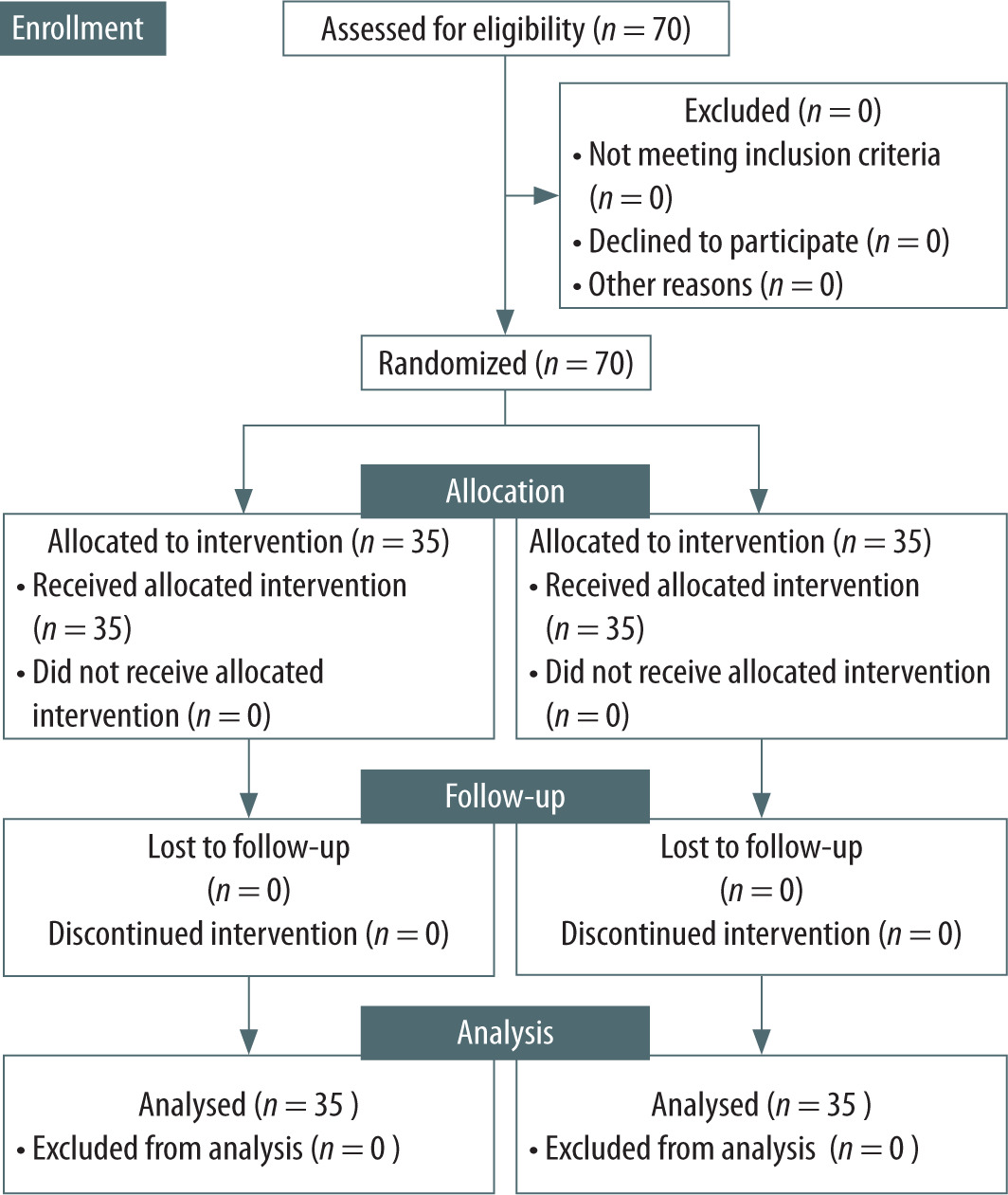
FIGURE 2
Influence of MgSO4 on the pharmacodynamic characteristics of rocuronium. Data are median with bars showing interquartile range. MgSO4 – red, saline – blue
There was no significant difference between the groups in the distribution of patients in terms of physical status (ASA) (P = 0.79), or in terms of satisfaction with tracheal intubation (TI) (P = 1.00), as well as the hemodynamic repercussions of laryngoscopy and TI, shown by heart rate, 75 (69–78 [58–104]) in the MgSO4 group compared to the saline group 78 (71–84 [47–105]), P = 0.095, and mean arterial pressure, 77.33 (65.67–80.67 [43.67–91.67]) in the MgSO4 group compared to saline, 79.33 (67.67–88.00 [44.33–108.00]), P = 0.28, at M3.
Surgical duration in minutes in MgSO4 group: 118.00 (90–150 [70–252]) compared to saline: 113.00 (85–130 [25–250]), P = 0.306; duration of anesthesia in minutes: 155.00 (135–190 [109–290]) in MgSO4 compared to saline, 150.00 (130–165 [50–269]), P = 0.190. Also, intraoperative propofol consumption (mg kg-1 min-1): 0.10 (0.09–0.11 [0.04– 0.36]) in the MgSO4 group compared to saline, 0.10 (0.08–0.11 [0.03–0.14]), P = 0.30, and intraoperative remifentanil consumption in the MgSO4 group: 0.08 (0.06–0.12 [0.01–0.36]) compared to saline, 0.10 (0.08–0.12 [0.03–0.18]), P = 0.07, showed no difference between the groups. There was also no diffe rence between the groups concerning length of stay in the PACU, 155.00 (120–186 [95–420]) in MgSO4 and 130.00 (101–200 [60–317]) in saline, P = 0.125.
There was a statistically significant difference between the groups in the time taken to recover consciousness (awake time in minutes – eyes opening spontaneously and confirming name and place), which was prolonged with MgSO4, 15.00 (10–21 [5–35]), compared to saline, 13.00 (9–15 [1–45]), P = 0.014, and opioid consumption in the PACU, measured by morphine equivalents, which was lower in the MgSO4 group 0.00 (0–0.66 [0–1.33]) compared to saline, 0.33 (0–1.00 [0–1.33]), P = 0.03 (Table 3).
TABLE 3
Intra-operative and postoperative data in patients receiving MgSO4 or saline. Values are median (IQR [range]). Mann-Whitney test
DISCUSSION
The evidence from this randomized controlled study provides a substantial understanding of the synergy between MgSO4, in the dosage of anesthetic adjuvant (30 mg kg–1), and the usual clinical dosage of rocuronium (0.6 mg kg–1). A significant interaction was observed between these substances, which could significantly influence clinical practice. It demonstrated that MgSO4 alters the pharmacological properties of rocuronium, resulting in a statistically significant reduction in latency (onset of action), a statistically significant prolongation of its clinical duration (CD25%) and a statistically significant increase in the time taken to re-establish neuromuscular transmission (TOF = 0.9%). Some authors have only observed a reduction in the latency of rocuronium with a dosage of 0.3 mg kg–1 and 0.6 mg kg–1 when combined with 60 mg kg–1 of MgSO4 [3]. Such findings highlight the potential of MgSO4 as an effective anesthetic adjuvant, capable of optimizing the conduction of anesthesia, not only the onset time of rocuronium. In times of shortage of medications such as neuromuscular blocking drugs (NMBD), in COVID-19, MgSO4 was found to be a good alternative as an anesthetic adjuvant, reducing the need for higher NMBD doses [4]. However, it must be taken into consideration that the safety margin of neuromuscular transmission may be altered due to the increase in the time required for its restoration, which may cause residual neuromuscular blockade. Because of this, it is essential to monitor neuromuscular blockade, recommended for all patients undergoing general anesthesia using NMBD [9, 10], especially when MgSO4 is associated with the anesthetic technique. Quantitative monitoring (documentation of TOF ratio ≥ 0.90) is the only method of ensuring that satisfactory neuromuscular function recovery has occurred. Furthermore, adequate monitoring allows for the correct reversal of neuromuscular blockade and the reduction of the inherent risks of residual muscular block, even with the use of sugammadex [11, 12], the direct reversal of rocuronium, since it is of utmost importance to know the degree of neuromuscular block for performing the correct reversal. In 2023, GermanoFilho et al. [13] evidenced that 60 mg kg–1 of MgSO4 could decrease the TOF ratio after deep and moderate blocks previously reversed by sugammadex. According to our results, MgSO4 can impair neuromuscular transmission and reduce its safety margin. Sun et al. [14] in a meta-analysis of eleven randomized controlled trials demonstrated that adding MgSO4 as an adjuvant in general anaesthesia altered the pharmacodynamic parameters of rocuronium. It significantly shortened the onset time and prolonged the clinical duration, as well as the recovery time of neuromuscular blockade. Various mechanisms by which MgSO4 can interfere with neuromuscular blockade have been described. Magnesium lowers acetylcholine release due to the inhibition of calcium-dependent channels, reduces the sensitivity to acetylcholine in the motor plate, and directly attenuates muscle fiber excitability [5].
Furthermore, the analysis of hemodynamic repercussions revealed an equivalence between the groups studied, indicating that the use of 30 mg kg-1 of MgSO4 did not cause abrupt effects on cardiovascular parameters during the perioperative period, as already stated by other studies [1]. Conditions during laryngoscopy and tracheal intubation were comparable in both groups, with a predominance of satisfactory conditions in the MgSO4 group, reinforcing the safety and effectiveness of using MgSO4 in this context [3, 14].
A relevant finding was the statistically significant result that awakening time was prolonged in the group that received MgSO4 compared to the control group. This result suggests a direct influence of MgSO4 on anesthetic depth with possible synergism with hypnotic drugs and opioids, as mentioned by previous authors [1, 15–18]. Our results showed a difference of 2 min (median) between groups. It is important to highlight that awakening time was a secondary outcome and probably does not have enough power to confirm this evidence; likewise, we need to think about the clinical relevance of the 2-minute (median) difference between groups. Nevertheless, intra-operative consumption of propofol and remifentanil was not significantly different between groups, in contrast to the evidence published by other authors [1, 18].
Moreover, in the PACU, the consumption of opioids was even lower in the MgSO4 group, whereas many authors have stated that there is no clinical evidence of the influence of MgSO4 on opioid activity to treat difficult types of pain, for instance, neuropathic and inflammatory [15]. Although MgSO4
reduced opioid consumption, it did not shorten the duration of the PACU stay, demonstrating that the use of MgSO4 neither shortened nor prolonged the recovery phase of patients, in agreement with other studies [1].
Limitations of the study
We did not measure the intra-operative serum concentration of MgSO4. As the groups were homogeneous, we assumed that the absence of this measure was not a major problem for comparative results. Also, our goal was to study the clinical and usual dosage of MgSO4 (30 mg kg–1), not lower or higher doses, since we wanted to correlate it with the current clinical practice. Another possible limitation is the lack of external validity for other types of surgery. Since we studied only open hysterectomies, the results may not be generalizable to other kinds of surgery.
Despite the evidence of synergistic interaction of MgSO4 and rocuronium, the residual neuromuscular block is still an unresolved concern for anesthesiologists [19]. A change of mindset is still needed to break the barriers of the lack of NMBD monitorization.
CONCLUSIONS
The conclusive results of this research offer a solid basis for considering MgSO4 as a promising and safe option as an anesthetic adjuvant, but always with the presence of quantitative neuromuscular blockade monitoring. Additional studies are needed to improve the effects of MgSO4 in different clinical contexts.