
A method that has recently become popular for administering pain relief during childbirth is the dural puncture epidural anesthesia (DPEA) technique. There is a lack of evidence addressing the utilization of DPEA in administering surgical anesthesia for caesarean section (CS), despite the fact that DPEA is a unique modification targeted at improving lumbar epidural analgesia (LEA) for patients in labor [1, 2]. Although intrathecal drug delivery is not a part of the DPEA technique, it is analogous to the combined spinal-epidural (CSE) procedure. The epidural space can be located with the help of an epidural needle during a DPEA procedure. Perforating the dura mater with a pencil-point spinal needle via the epidural needle is the next step; confirmation of the puncture is made by testing for free flow of clear cerebrospinal fluid. After that, this spinal needle is removed, followed by epidural catheter insertion into the epidural space to start the epidural anesthesia. By creating a hole in the dura mater, DPEA improves analgesia by transferring epidural medications into the intrathecal area [3].
No definitive recommendation regarding DPEA efficacy and size of the used pencil-point spinal needle is available, as some studies have suggested that DPEA could only be done with a larger gauge spinal needle, with recent studies having variable results [4–8]. It is believed that the size and type of spinal needles used during DPEA facilitate subarachnoid drug transfer, which could speed up the onset of analgesia and early bilateral sacral analgesia, as well as reducing the occurrence of asymmetric block and adverse effects on both the mother and the newborn compared to the conventional LEA technique [9]. According to certain theories, the dural hole made during DPEA facilitates subarachnoid transfer of the drugs to hasten onset of epidural analgesia [10]. It was concluded that the quantity of epidurally given medications had a direct correlation with the diameter of the dural hole, through which it could flow from the epidural space to the subarachnoid space [11–13]. Effects of DPEA on onset time of surgical anesthesia and its reliability during CS were unknown. To fill this informational void, we investigated the effectiveness of DPEA with 25-gauge (or 27-gauge Whitacre needles during elective CS in a randomized, prospective, double-blind clinical trial.
METHODS
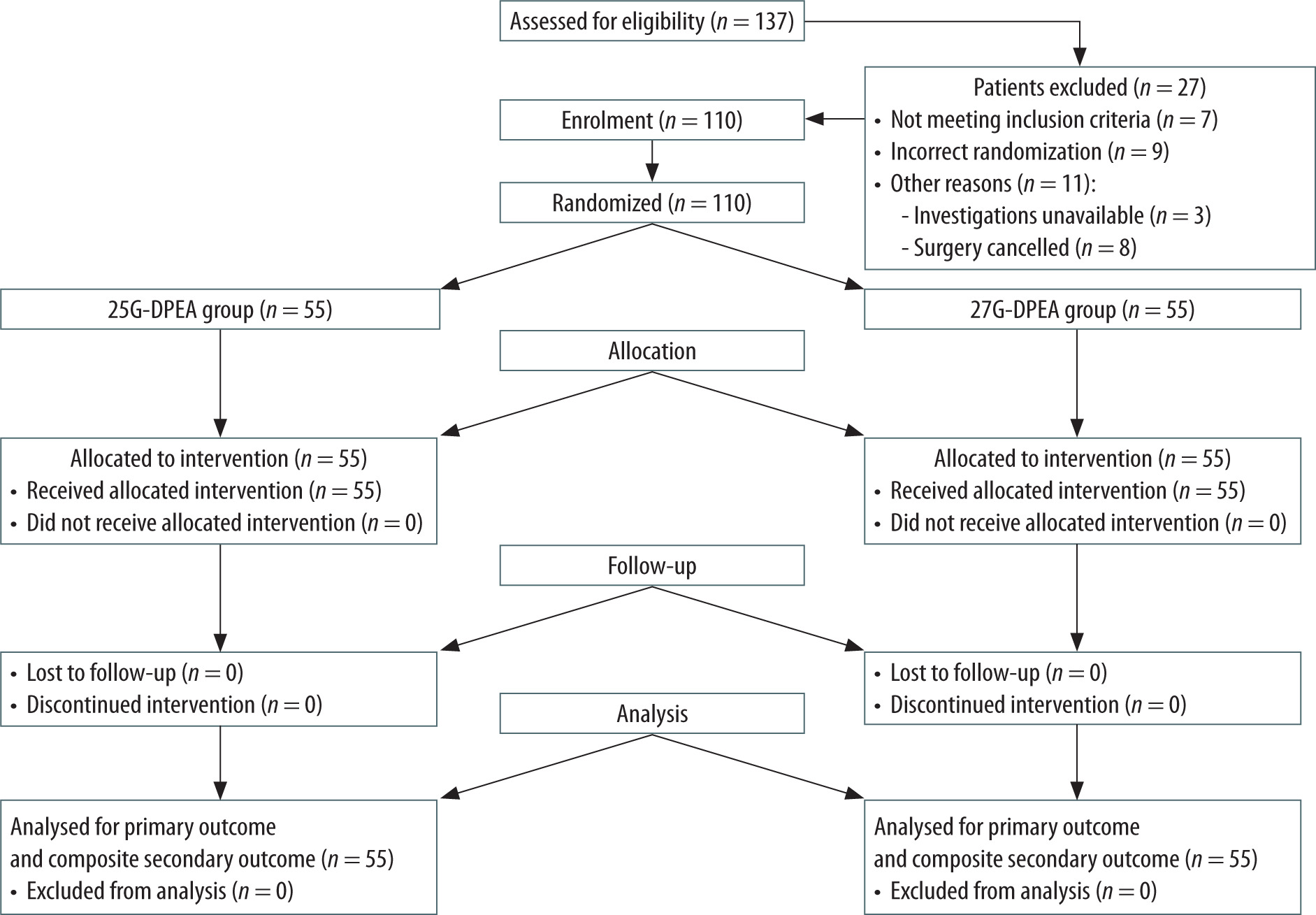
The researchers conducted a randomized, controlled, parallel comparative clinical trial in a single center (Department of Obstetrics and Gynaecology, Kasr Al-Ainy Hospital, Cairo University). The trial was double-blinded. Ethical approval of the statistical plan and complete protocol was provided by the Research Ethical Committee (REC) of Cairo University Hospitals, Cairo, Egypt. Thereafter, written informed consent was obtained from all participants before enrollment. The study was registered at https://clinicaltrials.gov/study/NCT06184425. CONSORT reporting guidelines were followed (Figure 1).
One hundred and ten parturients, ASA I and II, 20–35 years old, body mass index (BMI) < 35 kg m–2, with a single fetus of vertex presentation at 38 to 42 weeks’ gestation with planned elective CS, were equally divided into two groups for inclusion. Exclusion criteria were emergency CS, known fetal anoma lies, BMI ≥ 35 kg m–2, Hb < 10 gm%, patients with El-Ganzouri score ≥ 5, upper airway problems, hiatus hernia, obstructive sleep apnea, patient refusal, uncooperative patients, coagulation abnormalities, patients with maternal diseases or obstetric complications and severe hemodynamic instability.
Randomization
The study was designed as a double-blind, prospective, randomized controlled trial. A computer-generated 1 : 1 ratio randomization, through an online randomization program (http://www. randomizer.org), scheduled with blocks of 10, was created by a research coordinator not involved in the study, then the patients were allocated to one of two groups (DPEA group using 25G pencil-point spinal needles [25G-DPEA group] and DPEA group using 27G pencil-point spinal needles [27G-DPEA group]; each group numbered 55 patients). Allocation assignments remained concealed using sequentially numbered, opaque, sealed envelopes. After the initiation of patient enrollment and before the scheduled CS, the proceduralist opened the envelope containing the group allocation. DPEA technique was performed by the attending anesthesiologist or by residents under direct supervision of the attending anesthesiologist. The team performing the epidural technique had no other involvement in the study. The clinical team caring for the patient (obstetricians, anesthesiologists, and nurses), outcome assessors, data analyst, and study participants were blinded to randomization. The parturient was also blinded to the type of neuraxial procedure.
Anesthetic procedure
Parturients were checked and examined during the preoperative visit to determine who met the inclusion criteria and exclude others with the exclusion criteria. Approximately 1 hour before the scheduled CS, participants arrived at the preope rative room to start DPEA using either 25G or 27G Whitacre needles according to the randomization assignment. After participants arrived at the operating room, a peripheral venous access was established using an 18G intravenous cannula, and standard monitoring, including electrocardiogram (ECG), noninvasive arterial blood pressure and SPO2 monitoring, was applied; no premedication was given. The obstetrician monitored fetal heart rate (HR) before and after DPEA to rule out any abnormalities. Participants received a co-load of 500 mL of 37°C lactated Ringer’s solution infused at a rate of 5 mL kg–1 h–1 at the start of DPEA. Participants were in a sitting position and a midline approach was used while an unblinded anesthetist (who dealt with patients inside the pre-operative room) administered the DPEA technique in the preoperative room. The epidural space was located using a 17-gauge Touhy needle and the loss-of-resistance-to-saline technique. Then, a needle-through-needle technique was used to penetrate the dura using a 25-gauge or 27-gauge Whitacre needle. Once it was determined that cerebrospinal fluid was flowing freely, the spinal needle was removed. Subsequently, a 19-gauge spring-closed-tip catheter was guided cranially and implanted 5 cm into the epidural space.
To prevent post-DPEA hypotension, patients were placed supine with their left uterus displaced after DPEA insertion, and 5 L of oxygen per minute was supplied as supplemental oxygen. In order to rule out the possibility of intravascular or intrathecal catheter implantation, a test dose of 3 mL of 1.5% lidocaine with 1 : 200,000 epinephrine was administered.
Approximately 5 minutes after a negative test dose, participants received up to 20 mL of 0.0625% bupivacaine with 2 μg mL–1 fentanyl (in 5-mL increments) to establish a bilateral sensory level to pin-prick at the T10 dermatome. Then this sensory level was maintained with a continuous epidural infusion of the same solution at a rate of 12 mL per hour via an epidural pump until the participants were led into the surgery room, ensuring a constant sensory level (T10 analgesia was established by the epidural infusion via an epidural pump).
The team performing DPEA had no other involvement in the study. When patients entered the operating room at the scheduled time, the epidural pump was discontinued and a blinded anesthetist (who dealt with patients inside the operation room) verified that all participants exhibited a bilateral T10 sensory block, and the motor block was evaluated using the modified Bromage score at 5-min intervals for 30 min after completion of injection of epidural extension, where: 0 = no motor block; full flexion of knees and ankles = full movement = the patient can lift legs straight at the hip; 1 = just able to move knees; partial flexion of knees, full flexion of ankles = partial block 33% = the patient can bend knees but cannot lift legs straight; 2 = able to move feet only; inability to flex knees, partial flexion of ankles = partial block 66%; 3 = unable to move feet or knees; inability to flex knees and ankles = complete block = the patient has no movement in the hips, knees, or ankles [14]. A score of 1 or higher on the modified Bromage scale indicated the presence of motor blockage. Regular surveillance was resumed. The study’s participants, outcome assessors, data analyst, and members of the intraoperative clinical team (including obstetricians, anesthesiologists, and nurses) were all unaware of the randomization allocation process. The DPEA method remained hidden from the parturients. A co-load of 500 cc of 37°C lactated Ringer’s solution was administered intravenously over the course of 15 minutes. Intra-operatively, all patients received intravenous 2 g of cefotaxime, 4 mg of dexamethasone and 10 mg of metoclopramide if there were no contraindications.
A test dosage of 5 mL of 0.5% bupivacaine (bupivacaine 5 mg mL–1) was administered after a negative epidural aspiration was verified. If no aberrant signals were noticed after 3 minutes, a further 15 mL of 0.5% bupivacaine (bupivacaine 5 mg mL–1) was injected over 1 minute. Time zero for epidural extension anesthesia is the end of the injection of the test dose. If a T6 bilateral block could not be obtained within 10 minutes after the beginning of epidural extension anesthesia, 5 mL of epidural 0.5% bupivacaine (bupivacaine 5 mg mL–1) was administered every 5 minutes up to a total maximum cumulative dose of 30 mL. Surgery was allowed after achievement of a bilateral sensory block at T6. If no preoperative bilateral T10 block occurred or if the block failed to reach T6 bilaterally within 20 minutes after extension of epidural anesthesia, alternative neur-axial anesthesia or conversion to general anesthesia was allowed according to the clinical situation, and this patient was excluded from the study.
A 5 mg intravenous bolus of ephedrine was administered every 3 minutes until the hypotension resolved; hypotension was defined as a drop in mean arterial pressure of more than 25% from the baseline value or a drop in systolic arterial pressure below 100 mmHg. Intravenous atropine, 0.5 mg, was administered to patients with bradycardia, which was defined as a heart rate less than 60 beats per minute. Intraoperative infusion of isotonic saline 0.9% solution was administered at a rate of 1.5 mL kg–1 h–1. Colloid solution could be used to compensate for blood loss exceeding 300 mL. IV 50–100 μg naloxone was given if pruritus occurred. IV 25 mg pethi-dine was given after fetal delivery if shivering occurred. Mask oxygen inhalation or endotracheal intubation was applied in dyspneic patients, who were excluded from the study. When the sensory block level was at T6 or higher, intravenous boluses of 30 mg of ketamine or 50–100 μg of fentanyl were given to patients experiencing intraoperative discomfort (VAS ≥ 3). If the sensory block level was below T6, epidural injection of 3–5 mL of bupiva-caine 0.5% (bupivacaine 5 mg mL–1) was administered. If there was no improvement of intraoperative pain, general anesthesia was induced, and this patient was excluded from the study. Asymmetric blockade, where there was a disparity in sensory blockade of more than two dermal levels between the patient’s left and right sides, was assessed during patient examinations. Subsequent to delivery of the infant, a bolus of 5 IU of oxytocin was given by slow intravenous injection, followed if required by intravenous infusion of 30–50 IU of oxytocin in 500 mL of 0.9% saline at 30–125 mL h–1. Fetal Apgar scores were reported at 1 minute and 5 minutes. On a visual analog scale (VAS) (0 = completely dissatisfied and 10 = completely satisfied), postoperative satisfaction was assessed for both the patient and the surgeon. Furthermore, time to remove urinary catheter, time of Bromage score return to 0 and postoperative pain VAS scores (0 = no pain, 10 = worst pain imaginable) at 6 h and 24 h were assessed. Thereafter epidural injection of 10 mL of 0.125% bupivacaine (bupivacaine1.25 mg mL–1) with 5 μg mL–1 fentanyl was administered over 5 minutes, then the epidural catheter was removed before the discharge of the patients from the recovery room. Oral acetaminophen (650 mg every 6 h) and ibuprofen (600 mg every 6 h) were given for breakthrough pain if needed.
In order to check for post-dural puncture headache, nausea, vomiting, and back pain, participants were examined on the first, second, and third postoperative days.
The primary outcome was the onset time to surgical anesthesia, i.e. time from the end of the injection of the intraoperative epidural test dose to the achievement of a bilateral T6 block, so that it could mark the start of epidural extension anesthesia (time zero on the stopwatch) [15, 16]. Secondary outcomes included the quality of DPEA as described by Sharawi et al. [15]. This was a composite of the following factors: (1) failure to achieve a T10 bilateral block preoperatively (after epidural administration of 3 mL of 1.5% lidocaine with 1 : 200 000 epinephrine and up to 20 mL of a mixture of 0.0625% bupivacaine (bupivacaine 0.625 mg mL–1) with 2 μg mL–1 fentanyl), (2) failure to achieve surgical anesthesia (bilateral sensory block at T6 level) within 15 minutes of epidural extension anesthesia, (3) requirement for intraoperative analgesia, (4) requirement for repeat neuraxial procedure, or (5) conversion to general anesthesia. The rate of intraoperative analgesia was defined as the requirement for any rescue medication to control discomfort or pain during CS. Choice of medication to relieve the intraoperative pain was made according to the opinion of the anesthesiologist. All components of the composite outcome were used to assess the quality of the DPEA, and the presence of any event was considered positive for the secondary outcome. Other secondary outcomes included number of patients with cranial sensory block to T6 level and number of patients with a modified Bromage score reaching 3 at 15 min, highest achieved cranial and sacral sensory block level and highest achieved Bromage score at each time point after epidural extension, total volume of local anesthetics, incidence of vasopressor admini stration, intraoperative IV analgesic supplementation, incidence of asymmetrical block, general intraoperative data, neonatal outcome, maternal and surgeon satisfaction, in addition to adverse effects such as postoperative headache.
Sample size calculation was based on the primary outcome, which was the onset time to surgical anesthesia and was calculated from starting time of epidural extension anesthesia (time zero on the stopwatch) to when the patient could no longer feel a sharp sensation at T6 (assessed bilaterally at the midclavicular line) [15, 16]. Sample size calculation, determining the number of subjects as 100 (50 per group), was based on studies suggesting such a sample size for pilot studies with a moderate effect size, 95% confidence level, 80% power, and P < 0.05% for significance [17]. After adding 10% for dropouts, the number of patients was increased to 110 patients (55 per group).
Statistical analysis
SPSS v27 (IBM Corp., Armonk, NY, USA) was employed. Kolmogorov-Smirnov and Shapiro-Wilk tests were used to assess data normality. Normally distributed quantitative continuous data are expressed as mean and SD, while non-normally distributed quantitative data are expressed as median and range. Qualitative categorical data are expressed as percentages. Student’s t-test was used to compare normally distributed data. The Mann-Whitney or Kruskal- Wallis test was used to compare non-normally distributed data. For comparing categorical data, the c2 test or Fisher’s exact test was used. Analysis of variance (ANOVA) with repeated measures and post-hoc Bonferroni correction was used to compare hemodynamic changes over time. P < 0.05 was considered statistically significant.
RESULTS
Between January 2023 and December 2023, 137 patients were assessed and screened for eligibility. Twenty-seven patients were excluded, so that a total of 110 patients were included in the final analysis and divided equally, giving 55 patients in each group (Figure1). Table 1 presents baseline participant characteristics, indications for CS, and preoperative epidural variables.
TABLE 1
Demographic and clinical characteristics of participants
Primary outcome: onset time of surgical anesthesia
The primary outcome was median time to achieve a bilateral sensory block to T6 level; the median (IQR) time to surgical anesthesia was 9.12 (8.71–18.54) minutes in the 25G-DPEA group and 14.18 (12.43–23.56) minutes in the 27G-DPEA group (Table 2). The median (IQR) difference in the onset time of sensory block between the 2 groups was 5.06 (3.72–5.02) minutes. There was a significant difference in the time required to achieve surgical anesthesia between the two compared groups (HR: 2.3; 95% CI: 1.79–3.14%; P < 0.0001).
TABLE 2
Intraoperative data and outcomes
[i] Values are expressed as median (interquartile range). Data were compared using the Kruskal-Wallis test with post-hoc pairwise comparisons using Dunn’s test. Continuous normal variables are presented as mean ± SD using Student’s t-test. Categorical data are presented as numbers using c2 test. P > 0.05: not statistically significant. P < 0.05: (*) statistically significant.
Secondary outcomes: quality of epidural anesthesia
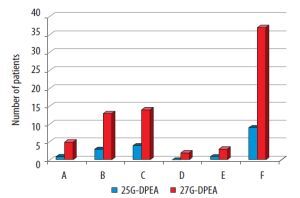
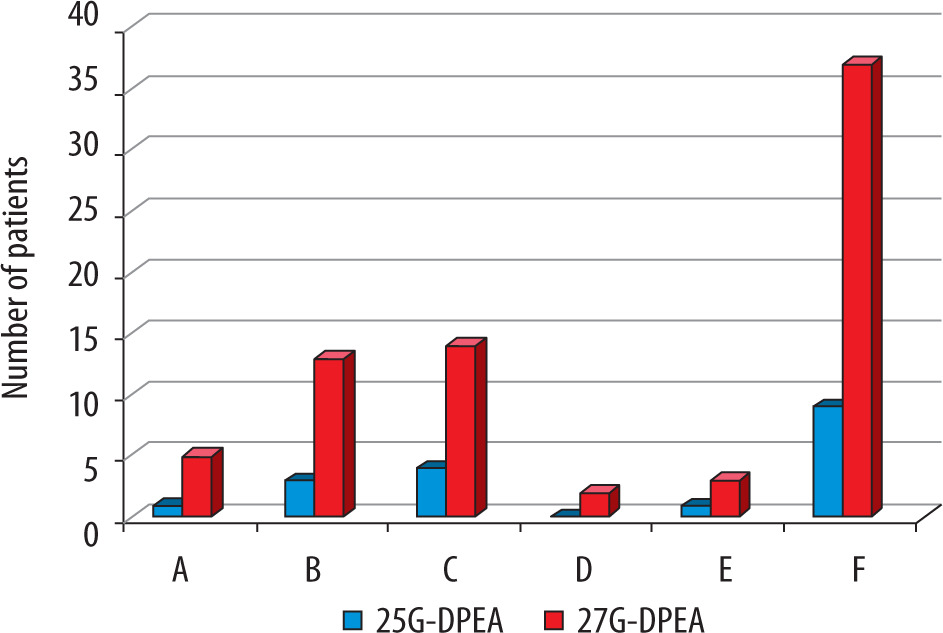
The composite secondary outcome that was used to assess the quality of the DPEA was composed of 5 components that indicated lower quality of anesthesia in the 27-DPEA group compared to the 25-DPEA group, as shown in Figure 2; the observed composite rate was 9 of 55 parturients (16.4%) in the 25-DPEA group compared to 37 of 55 parturients (67.3%) in the 27-DPEA group (odds ratio: 0.095; 95% CI: 0.04–0.24%; P < 0.0001); 1 patient in 25G-DPEA versus 5 patients in 27G-DPEA failed to achieve T10 block preoperatively, 3 patients in 25G-DPEA versus 13 patients in 27G-DPEA had onset of surgical anesthesia > 15 minutes, 1 patient in 25G-DPEA versus 3 patients in 27G-DPEA were converted to general anesthesia, 4 patients in 25G-DPEA required intraoperative analgesia versus 14 patients in 27G-DPEA. In addition, 2 patients in 27G-DPEA required repeat of the neuraxial procedure, in contrast to 25G-DPEA, where no patients repeated the neur-axial procedure.
FIGURE 2
Secondary outcome composite with its individual components for assessment of quality of dural puncture epidural anesthesia. A: Failed T10 block preoperatively. B: Onset of surgical anesthesia > 15 minutes. C: Intraoperative analgesia. D: Repeat neuraxial procedure. E: Conversion to general anesthesia. F: Secondary outcome composite
Other secondary outcomes
Table 2 shows:
The number of patients with a modified Bromage score of 2–3 when the primary outcome was achieved was 41 (75.9%) in 25G-DPEA and 12 (24%) in 27G-DPEA (95% CI: 33.31–65.43%, P < 0.0001).
On entry to the operating room, the 25G-DPEA group was presented with a significantly higher sensory block level than 27G-DPEA (66.7% vs. 40%, 95% CI: 7.52–43.33%, P = 0.007), and there was no statistically significant difference regarding the modified Bromage score (70.4% vs. 70%, 95% CI: 16.71–17.69%, P = 0.97) between the compared groups.
The number of patients with cranial sensory block to T6 level at 15 min was 51 in 25G-DPEA and 37 in 27G-DPEA (95% vs. 74%, 95% CI: 7.2–34.9%, P = 0.003). The number of patients with a modified Bromage score reaching 3 at 15 min was 47 in 25G-DPEA and 35 in 27G-DPEA (87% vs. 70%, 95% CI: 1.18–32.23%, P = 0.04).
Regarding the supplementary epidural top-ups: patients in the 27G-DPEA group required a single top-up on average, while those in the 25G-DPEA group did not require supplementary epidural top-ups (P < 0.0001), and subsequently the total dose of bupivacaine (mL) was significantly higher in 27G-DPEA than in 25G-DPEA (P < 0.0001).
Time from induction of epidural anesthesia to patient discomfort was statistically significantly shorter in 27G-DPEA than 25G-DPEA (P < 0.0001), so that 51 patients in the 25G-DPEA group versus 41 patients in 27G-DPEA group did not require intraoperative analgesia (94.6% vs. 82%, 95% CI: 0.03–25.89%, P = 0.045).
Table 3 shows:
TABLE 3
Sensory nerve and motor block levels in the two groups at each time point after epidural extension
[i] Values are expressed as median (interquartile range). The data were analyzed with linear mixed model. Ptime: the time effect within group, the differences between the two groups at each time point were tested with adjusted Bonferroni correction for multiple comparisons. P < 0.05: (*) statistically significant. Pgroup: the main effect between the 25G-DPEA group and the 27G-DPEA group over time. Pinteraction: the interaction effect of group-by-time.
The cranial and sacral sensory block levels and modified Bromage motor block scores at different time points after beginning of epidural extension.
The sensory block level on the cranial side was significantly higher at 5 min, 10 min and 15 min in 25G-DPEA than in 27G-DPEA (P < 0.05). The sensory block level on the sacral side was significantly lower in 25G-DPEA than in 27G-DPEA at each time point (P < 0.05). The modified Bromage motor block score was significantly higher in 25G-DPEA than in 27G-DPEA at each time point (P < 0.05).
Table 4 shows:
TABLE 4
Adverse events
[i] Continuous normal variables are presented as mean ± SD using Student’s t-test. Categorical data are presented as numbers and analyzed using the c2 test. P > 0.05: not statistically significant. P < 0.05: (*) statistically significant.
[ii] The patient satisfaction rating ranged from 0 (extremely dissatisfied) to 10 (extremely satisfied).
Patient satisfaction was greater in 25G-DPEA versus 27G-DPEA (P = 0.03). Surgeon satisfaction was greater in 25G-DPEA versus 27G-DPEA (P = 0.017). Moreover, there were no significant differences in terms of intra-operative fluid administration, estimated blood loss, urine output, neonatal outcomes, adverse effects (hypotension, respiratory depression, chest distress, nausea and vomiting, dizzy, chills, nasal obstruction, pruritus, high spinal, local anesthesia systemic toxicity, or asymmetrical block) and DPEA post-operative complications (until 3 days), postdural headache, back pain, motor deficit, or paraesthesia.
DISCUSSION
Dural puncture epidural anesthesia (DPEA) technique was a modification of the CSE technique. DPEA involves puncturing the dura with a pencil-point spinal needle and the local anesthetics are introduced into the epidural space via an epidural catheter instead of direct injection into the subarachnoid space [18]. It was suggested that dural perforation facilitated the subarachnoid local anesthetic infiltration [19]. According to our results, the 25G-DPEA group had a higher quality of anesthesia with superior cranial and sacral coverage in addition to a higher motor block degree than the 27G-DPEA group during elective CS because the onset to surgical anesthesia was approximately 5 minutes faster with 25G-DPEA than with 27G-DPEA, leading to a more favorable quality of anesthesia for CS. Moreover, the composite secondary outcome – a composite of failed T10 block preoperatively, onset of surgical anesthesia > 15 minutes, need to repeat neuraxial procedure, requirement of intraoperative analgesia and conver- sion to general anesthesia – indicated lower quality of anesthesia with 27G-DPEA than with 25G-DPEA. These results are consistent with a study which suggested that DPEA could benefit the parturient through improving the sacral spread and accelerating onset of epidural analgesia with a bilateral spread, compared to LEA [20]. Furthermore, a recent review proved a more rapid onset of epidural analgesia, early bilateral sacral analgesia, lower incidence of asymmetric block, and fewer maternal and fetal side effects with DPEA compared to LEA [18]. In contrast to our results, there were two systematic reviews of randomized controlled trials that compared DPEA with LEA and concluded that there was a lack of a clear evidence on either benefits or risks of DPEA and recommended more studies with different sizes of the spinal needles before making any final conclusion about DPEA [21, 22].
Regarding the size and the type of the spinal needles, it was assumed that the dural puncture made during DPEA could facilitate the drug transfer into the subarachnoid space and hasten the onset of epidural analgesia [23]. It was concluded that the passage of epidurally injected drugs into the subarachnoid space via the dural hole was directly proportional to the dural hole size [24, 25].
Although there was a controversy regarding the correlation between the spinal needle size and the effectiveness of DPEA, there are several studies supporting our results; these studies reported that 25G-DPEA was associated with faster onset of surgical anesthesia and sacral coverage, greater sacral spread, lesser requirement of epidural top-ups and lower incidence of asymmetric block, so that 25G-DPEA showed a greater benefit to the parturient [20, 26], while other clinicians used a 26G pencil-point needle and documented its effectiveness in DPEA [27]. A previous study compared 25GDPEA with 27G-DPEA for labor analgesia and found a 1.6-min shorter onset time with 25G-DPEA than with 27G-DPEA. However, the authors concluded that, although this difference was statistically significant, it was of no clinical importance [19]. Although it was shown that the 27G-DPEA did not affect the quality of epidural analgesia during labor [28], another study recorded fast onset with improved quality of labor analgesia with 27G-DPEA technique when compared to LEA technique [29]. Moreover, with so much heterogeneity in the protocols of various studies regarding the local anesthetic volume, time for completing the injection, size of the spinal needle, and variability of patient demographics in these studies, it has been difficult to assess the exact role of spinal needle size in DPEA.
According to previous studies, sacral spread occurred earlier and was more extensive with 25G-DPEA or 26G-DPEA when compared to LEA [30–32]. In addition, in vitro research showed that lidocaine flowed significantly into the subarachnoid space via 18-gauge and 24-gauge needle punctures, but not through a 27-gauge puncture [24]. It was found that 27G-DPEA did not provide improved quality of labor analgesia when compared with LEA [28]. Although a larger gauge spinal needle could play a critical role in transmeningeal flux of the local anesthetics, the choice of the spinal needle should be limited to no larger than 25G in order to minimize the incidence of postdural puncture headache and abnormally extensive blockade. Aside from the spinal needle, it was found that the transmeningeal flux of anesthetics might depend on many other factors that could affect the performance of the epidural anesthesia. These include the type and size of the epidural needle; the type and length of the epidural catheter inserted into the epidural space; choosing an appropriate level for insertion of the epidural needle was crucial to achieve the desired block area; the rate of injection and the total volume of local anesthetic; the pressure gradient between the epidural and the subarachnoid spaces, which could be altered by the volume of local anesthetic; the type of the used local anesthetic and its concentration; the position of the patient during and after epidural administration due to the effects of gravity on the distribution of the anes thetic in the epidural space, especially when patients were positioned laterally or in a head-down or head-up tilt; and the great variation in the anatomy of the epidural space. Proper attention to these factors could help optimize the quality and safety of the epidural block [21, 23, 33].
The investigators used 20 mL of 0.5% bupiva-caine for epidural extension anesthesia, which is consistent with different studies reporting that administration of various epidural dosing regimens such as 20 mL of 0.125% bupivacaine and 12 mL of 0.25% bupivacaine during 25G-DPEA technique resulted in a more rapid onset of thoracic sensory blockade and greater median cranial spread following the injection of a higher-volume and low-concentrated initial epidural bolus [19, 34].
It was documented that the hemodynamic parameters with DPEA technique became more stable than that with CSE technique and were comparable with that of LEA technique [19]. These findings are consistent with our results which recorded the limited need for vasopressors in both groups.
The two compared groups, 25G-DPEA and 27G-DPEA, did not experience any side effects such as post-dural puncture headache, respiratory depression, chills, nausea, vomiting, nasal obstruction, maternal hypotension or chest pain. Furthermore, a lack of difference in neonatal outcomes between the two groups suggested that the DPEA technique used for CS was equally harmless to both the mother and the newborn. These findings were correlated with those obtained by Gunaydin [18]. It was noted that the obstetric outcome became difficult to compare amongst the studies as the decision, especially CS, was often dependent on multiple factors such as the local hospital protocol and the experience of the attending obstetrician [35].
LIMITATIONS
This trial was performed in parturients scheduled for elective CS, not intrapartum CS. Adhesions in the epidural space may affect spread of the local anesthetic solution in the epidural space as well as its translocation into the subarachnoid space, which might increase the bias of the data.
CONCLUSIONS
25G-DPEA resulted in significantly faster onset of surgical anesthesia, higher cranial and sacral spread with higher motor block scores at each time point than 27G-DPEA. We believe these results are clinically meaningful and relevant for patients requiring emergency CS under epidural extension anesthesia.