
Dear Editor,
Intracranial hypotension (IH) is a condition characterized by a spectrum of neurological symptoms, including postural headaches and, in very rare, severe cases, coma. Severe cases are potentially life-threatening. IH is typically associated with spontaneous leakage of cerebrospinal fluid (CSF) or as a sequela to repeated lumbar puncture [1–3]. Notably, over the past decade, only two documented cases of IH resulting from trauma have been reported [4]. We would like to present a unique case in which IH was associated with a shoulder injury and resulted in a coma.
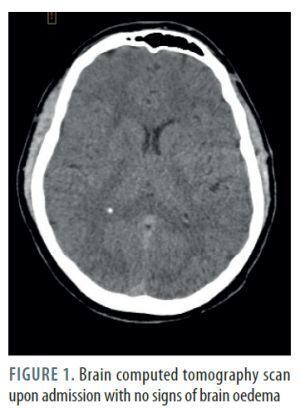
A 24-year-old male patient was admitted to a trauma centre after a motorcycle accident involving a collision with a traffic sign, resulting in a right shoulder injury. Initial evaluation by emergency services showed only paralysis of the right arm; the patient was fully conscious. Upon admission, a whole-body computed tomography (CT) scan was performed, revealing a single fracture of the right collarbone, with no signs of brain injury (Figure 1). Two hours later, the patient fell into a coma, necessitating intubation, sedation, and transfer to the intensive care unit (ICU). A subsequent brain CT scan showed diffuse brain oedema (Figure 2). Intracranial pressure (ICP) was measured at –5 mmHg in the drainage position with the upper body elevated to 30° using a multimodal intracranial probe. The patient remained sedated and ventilated for 48 hours, sustaining stable low ICP levels between –5 and 2 mmHg. Upon cessation of sedation, the patient showed a gradual improvement in consciousness, which was consistent with the changes in ICP levels. Interestingly, higher ICP levels were associated with a better state of consciousness.
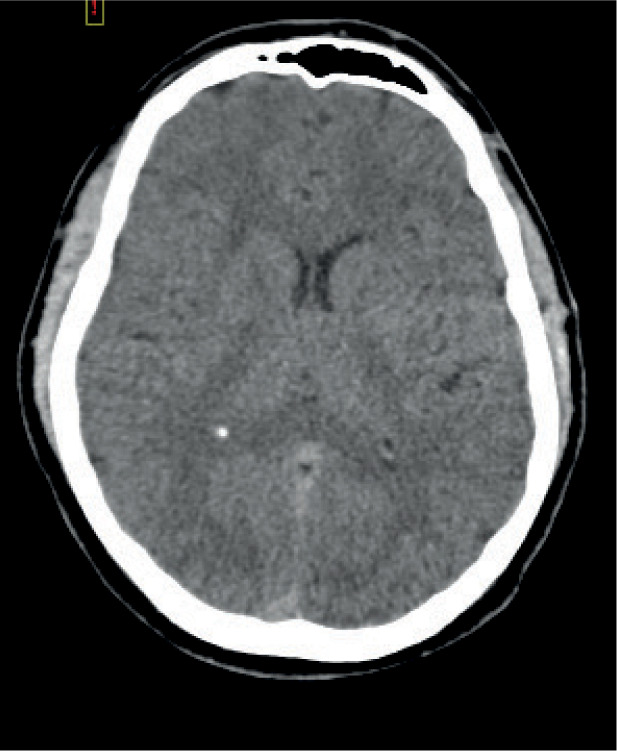
FIGURE 2
Brain computed tomography scan after intubating the patient in a coma with signs of diffuse brain oedema

Due to the observed correlation between improved consciousness and elevated ICP, concerns arose regarding CSF overdrainage. CT perimyelography was performed, revealing an unexpected discovery of CSF leakage through the injured right brachial plexus.
The patient was positioned in a neutral position. The ICP stabilized spontaneously at around 3 mmHg on the 4th day of admission. The patient regained full consciousness and was extubated on day the 5th day and discharged from the ICU on the 6th day. The patient underwent brachial plexus reconstruction three months later. Presently, the patient shows paresis of the right arm with a Neurological Impairment Scale (NIS) score of 2.
IH is rarely associated with trauma. Our case demonstrates the importance of being aware of this association, even in the absence of head or spinal trauma. Normally, IH causes recurring postural headache, but coma can rarely be a sole symptom. Treatment of the cerebrospinal leak depends on the underlying cause and the size of the leak. Usually, a small leak can resolve spontaneously, while a larger leak may need surgical treatment, as in our case. The most common conservative approach incorporates bed rest, caffeine intake restriction and increased oral fluid intake. Blood patch and block of sphenopalatine ganglion are two othercommon interventions to consider treating IH, with likely success when IH is a sequela to repeated lumbar punctures. For treating cerebrospinal leak from the spine or plexus, surgical repair is a frequently used approach [5–7].
There are several key lessons to learn from this case. Firstly, diagnosing IH is challenging due to the absence of pathognomonic signs on standard CT scans, so additional tests such as perimyelography are essential [8]. Secondly, a negative or very low ICP should prompt consideration of potential IH due to CSF leakage as a possible cause of coma. Lastly, it is crucial to move a patient with known or suspected CSF leakage from the standard semirecum-bent position to the supine position.
Written informed consent was obtained from all subjects.