
Knee pain is common among individuals around the age of 55 and older. It is often caused by osteo- arthritis or trauma, with the most common injury leading to chronic knee pain being anterior cruciate ligament (ACL) injury. Chronic knee pain tends to intensify with movement, especially on jumping or walking, and existing inflammation within the joint can worsen the pain [1]. In severe cases of osteoar- thritis of the knee (gonarthrosis), knee arthroplasty (knee replacement) serves as an effective surgical intervention for knee osteoarthritis. During this sur- gery, the affected joint is replaced with a prosthesis that functions similarly to a natural joint [2]. However, nearly 20% of patients undergoing knee arthroplas- ty do not fully recover and continue to experience chronic knee pain along with impaired joint function. As many as half of these patients might require revi- sion surgery due to persistent pain or infection [3].
Surgical injury triggers an inflammatory re- sponse initially caused by local mediators, which can also have systemic effects. Such inflammation not only leads to increased postoperative pain but can also result in such complications as delirium and a longer recovery period [4]. Furthermore, sleep dis- ruption due to severe pain can contribute to mental problems and worsen outcomes [5].
Adequate perioperative pain management is considered a top research priority for patients un- dergoing knee replacement surgery, since it plays a crucial role in facilitating early mobilization and re- habilitation. A comprehensive recovery program for knee surgery patients was described in The Lancet by Price et al. [3]. One important aspect of this pro- gram is effective analgesia, including techniques such as regional blocks.
Peripheral nerve blocks (PNBs) serve as an effec- tive and safer alternative to traditional opioid anal- gesia in knee surgery. PNBs involve the use of local anesthetics [6] and can address concerns around the use of opioids, such as addiction risks and other safety issues [7]. The advantages of PNB include not only fewer side effects but also faster patient reco- very [8]. The conventional PNBs used in knee sur- gery include femoral nerve block (FNB) and sciatic nerve block (SNB). Recently there has been a grow- ing interest in using adductor canal block (ACB) [7]. The International Consensus on Anesthesia-Related Outcomes after Surgery (ICAROS) recommends the use of PNBs in total knee arthroplasty to mini- mize postoperative complications [9].
However, to prolong the effect of PNBs, which generally last a few hours, adjuvants such as dexa- methasone (DEX) may be required [10, 11]. Perineu- ral DEX added to a PNB demonstrated decreased rescue analgesia requirements and pain intensity after upper limb surgery [8]. The precise mecha- nisms by which DEX controls pain are not fully un- derstood. It probably has both local and systemic effects. Locally it acts as a vasoconstrictor, which can reduce the absorption rate of anesthetics [8, 12]. Systemically, it suppresses the release of inflam- matory mediators and pain signals by modulating the cyclooxygenase and lipoxygenase pathways [4], as well as affecting C-fibers and nerve cells [8]. These anti-inflammatory effects along with allevia- tion of nausea and vomiting [13] may contribute to improved patient recovery and longer peripheral block duration [14, 15]. Additionally, some guide- lines recommend using steroid injections for knee osteoarthritis treatment. Intra-articular injections were associated with lower pain intensity in such patients [16].
Previous systematic reviews have examined mixed intravenous and perineural routes of DEX administration in total knee reconstruction [17] or perineural DEX in upper limb surgery [8]. Some systematic reviews have studied the effects of DEX in other lower limb procedures, such as hip arthro- plasties [11, 18]. However, there is currently no re- cent review specifically focusing on the analgesic effects of perineural DEX in knee surgery patients.
This systematic review aims to evaluate the analgesic effects of perineural DEX as an adjuvant to regional peripheral block in knee surgery.
METHODS
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [19]. The protocol was registered in Open Science Framework and is publicly available at https://doi.org/10.17605/OSF.IO/AQRZ2.
Search strategy
We searched PubMed and the Cochrane Library for the relevant literature published before Septem- ber 11, 2024. We used the following search query: ((“knee surgery”) OR (“total knee replacement”)) AND ((“regional anesthesia”) OR (“dexamethasone”) OR (“perineural dexamethasone”)) + randomized controlled trial (PubMed) / trial (Cochrane Library) + English language (please see the supplementary file). We screened the titles and the abstracts against the following inclusion and exclusion criteria:
Exclusion criteria
population: wrong surgery type, no PNB,
intervention: epidural, oral, intravenous DEX,
comparator: active comparator,
study types: ongoing, observational, animal, and in vitro studies, secondary analyses, and editor correspondences. These types of studies gene- rally have a higher risk of bias than RCTs.
After selecting eligible studies, duplicates were removed.
Outcomes
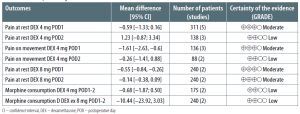
The primary outcomes of our meta-analysis are postoperative pain intensity scores at rest and with movement (numerical rating scale (NRS) or visual analogue scale (VAS, 0–10)) for postoperative days (POD) 1 and 2. The secondary outcome is postope- rative opioid consumption, converted to morphine equivalents (mg), for the first two POD.
Data extraction and statistical methods
AA extracted data from eligible studies and re- corded the citation, country, study design, types of surgery, age and number of participants, com- parator, dose and concentration of DEX, peripheral block used, and study conclusions in Table 1. The data from each study were screened against the outcomes of interest to be eligible for the evidence synthesis. Outcome data were extracted to an Excel table and analyzed using the Review Manager (RevMan) com- puter program, Version 5.4 (The Cochrane Collabora- tion, 2020). We double-checked the data extracted.
For some studies, we estimated the missing data values of the sample mean and sample standard deviation using existing methods [20, 21]. Hetero- geneity was estimated by the I2 statistic. Subgroup analysis was used to explore the sources of het- erogeneity. In the case of high heterogeneity, we explored it by subgroup analysis based on the DEX regimen. We used a random-effects meta-analysis for synthesis of evidence. To express continuous outcomes, we calculated the mean difference (MD) and 95% confidence interval (CI) using an inverse variance method. The sensitivity analysis was per- formed by repeating the analysis with each individ- ual study removed. The outcomes were shown in forest plots and summarized in a summary of find- ings table. A reduction in pain of 2 or more points on a VAS scale of 10 was considered to be clinically meaningful [22].
TABLE 1
Characteristics of included studies
[i] 1S – first study, 2S – second study, ACB – adductor canal block, ACLR – anterior cruciate ligament reconstruction, AKS – arthroscopic knee surgery, CFNB – continuous femoral nerve block, FNB – femoral nerve block, ID – intravenous dexamethasone, PD – perineural dexamethasone, PNB – peripheral nerve blockade, QNB – quadruple nerve block, RCT – randomized controlled trial, SNB – sciatic nerve block, SSNB – subsartorial saphenous nerve blockade, TKA – total knee arthroplasty, TKR – total knee replacement, UKA – unicompartmental knee arthroplasty
Risk of bias assessment and the certainty of evidence
Each RCT was classified as having a low, unclear, or high risk of bias in the following areas: randomi- zation, allocation concealment, blinding of par- ticipants, staff, and investigators, missing data, and selective reporting of outcomes. In the category of “other” bias, we assessed the conflict of interests in the included studies [23]. KT summarized the risk of bias using RevMan. We did not exclude any stud- ies based on our assessments.
We assessed the certainty of evidence using the Grading of Recommendations Assessment, De- velopment and Evaluation (GRADE) approach [24]. We assessed five outcomes: pain at rest, pain with movement and morphine consumption. Our evalu- ation considered factors such as risk of bias, impreci- sion, inconsistency, and indirectness. Each outcome was assigned a level of certainty: “low,” “moderate,” or “high.” We presented our assessments in the sum- mary of findings. For meta-analyses involving more than ten RCTs, we planned to assess publication bias using a funnel plot.
RESULTS
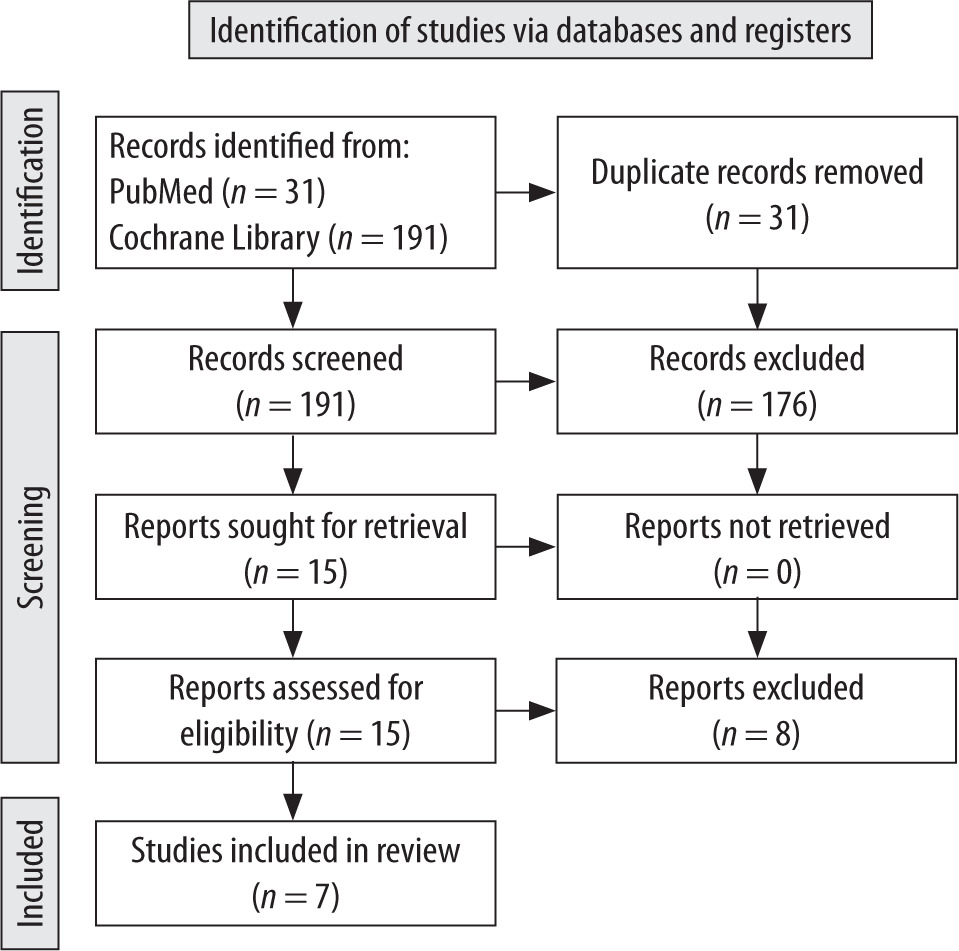
The initial search yielded 160 articles, 153 of which were excluded. The reasons for exclusion are described in Figure 1. Seven RCTs with 551 patients were included in the meta-analysis [25–31] (Table 1). The studies were focused on total knee replace- ment, total knee arthroplasty, and ACL reconstruc- tion. The doses of DEX ranged from 1 to 8 mg. The regional blocks included sciatic nerve block, single-shot nerve block, FNB, perineural nerve block, and ACB. The age of participants varied from children to seniors. While most of the studies fo- cused on adult populations, Aoyama et al. [25] and Veneziano et al. [30] investigated the effects of DEX in children, adolescents, and young adults.
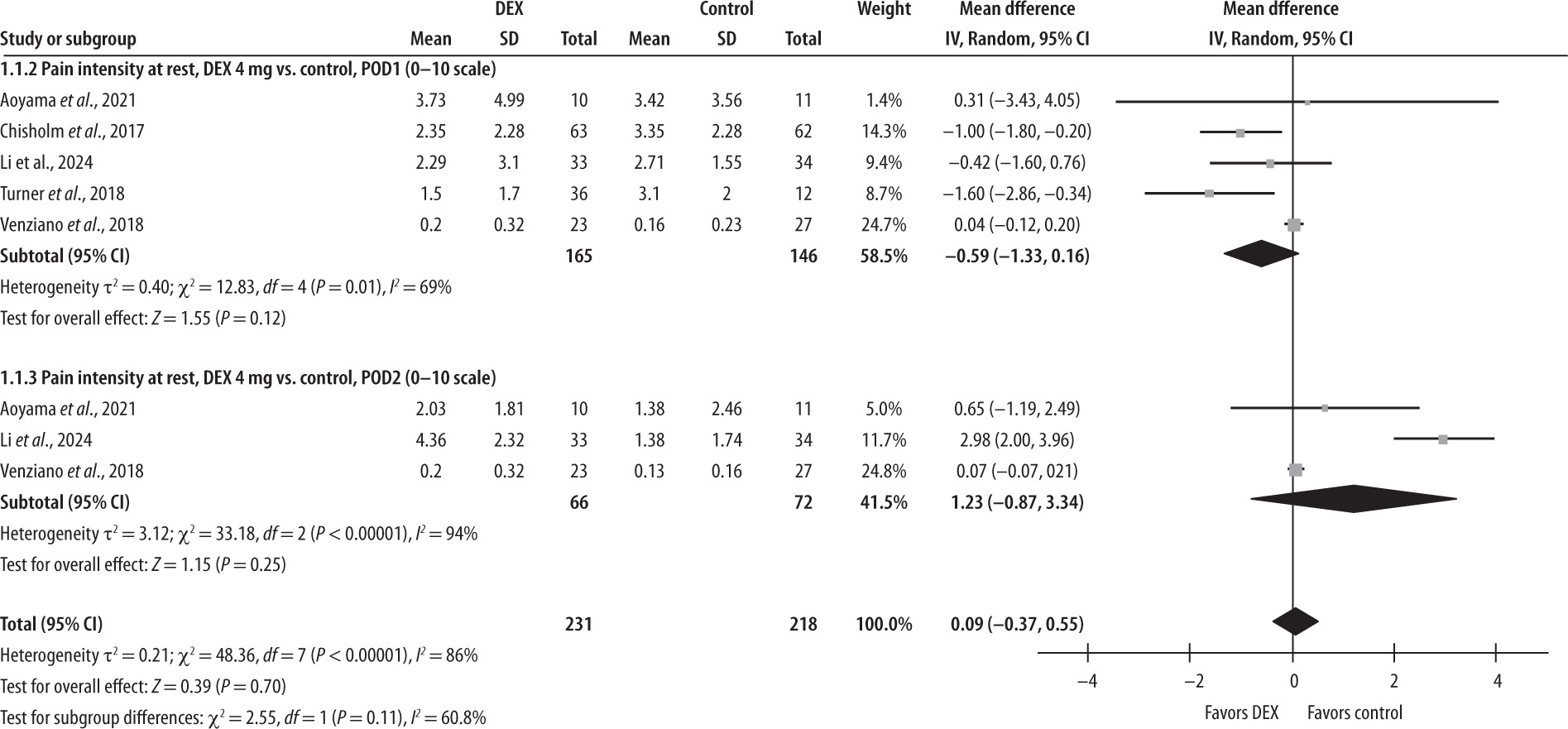
Postoperative pain intensity score at rest measured on POD1 and POD2 for DEX 4 mg vs. control (NRS/VAS, 0–10)
The forest plot in Figure 2 presents the compari- son of the DEX 4 mg group with the control group on POD1 and POD2. Five studies (DEX = 165, con- trols = 146) report the results for pain scores at rest on POD1. The model does not favor either group (MD with 95% CI is –0.59 [–1.33; 0.16]; P = 0.12). There is moderate heterogeneity among the in- cluded studies (I2 = 69%). Three studies (DEX = 66, controls = 72) reported pain scores at rest on POD2. On the second POD the model did not favor either group (MD = 1.23 [–0.87; 3.34], P = 0.25); the hetero- geneity among the included studies was consider- able (I2 = 94%). Overall, the model does not favor either group (MD with 95% CI is 0.09 [–0.37; 0.55]; P = 0.7).The sensitivity analysis indicates that the model favors the DEX 4 mg group on POD1 when the study by Venziano et al. is excluded [30].
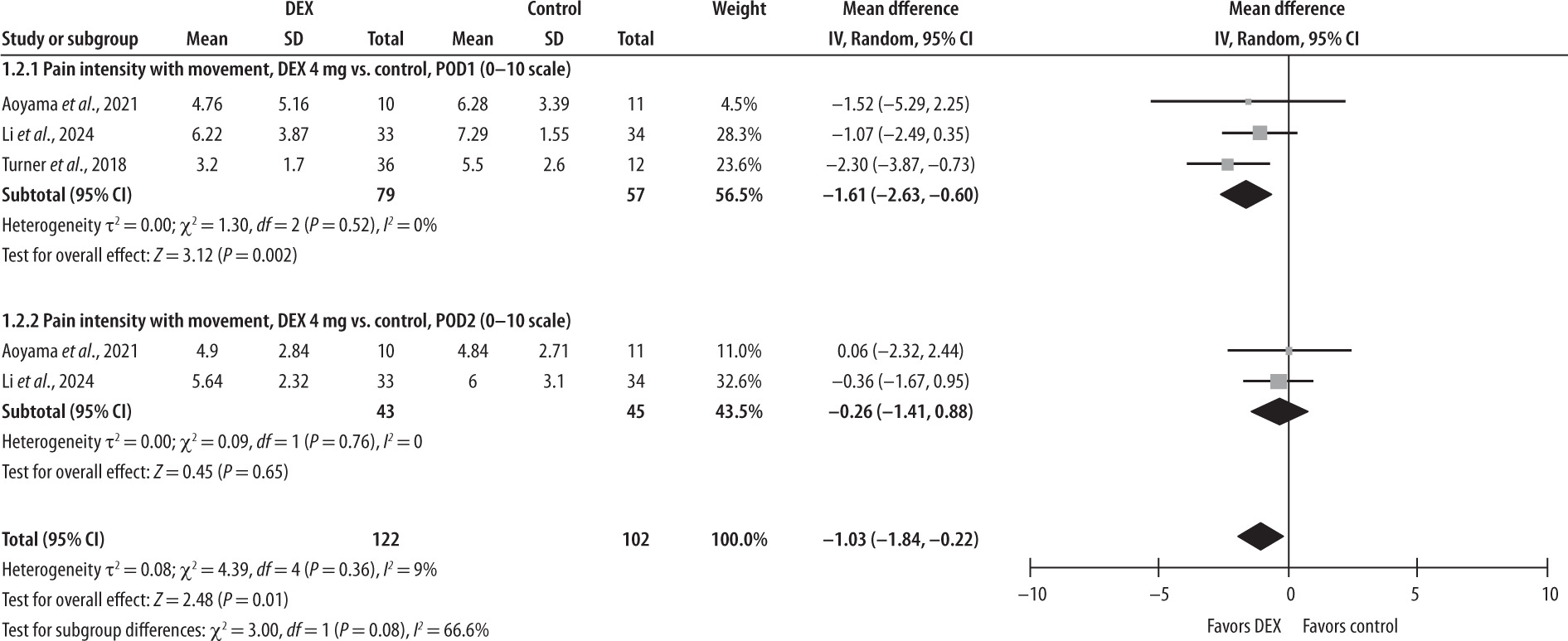
Postoperative pain intensity score with movement measured on POD1 and POD2 for DEX 4 mg vs. control (NRS/VAS, 0–10)
The forest plot in Figure 3 below presents the com- parison of pain intensity with movement in the DEX 4 mg group versus the control group on POD1 and POD2. Three studies (DEX = 79, controls = 57) re- port pain scores on movement in the first 24 h after the surgery. The model favors the DEX group over the control group (MD with 95% CI is –1.61 [–2.63, –0.60], P = 0.002, I2 = 0%). Only two studies (DEX = 43, controls = 45) reported the results of pain intensity with movement on POD2. On the second day after surgery the model did not favor the DEX group (MD with 95% CI is –0.26 [–1.41, 0.88], P = 0.65), with no heterogeneity observed between studies (I2 = 0%). Overall, the model favors the DEX group in terms of the pain intensity with movement, showing a sig- nificant effect (–1.03 [–1.84, -0.22], P = 0.01). The re- sults are sensitive to the exclusion of a study by Turner et al. [28], in which case the model does not favor either group.
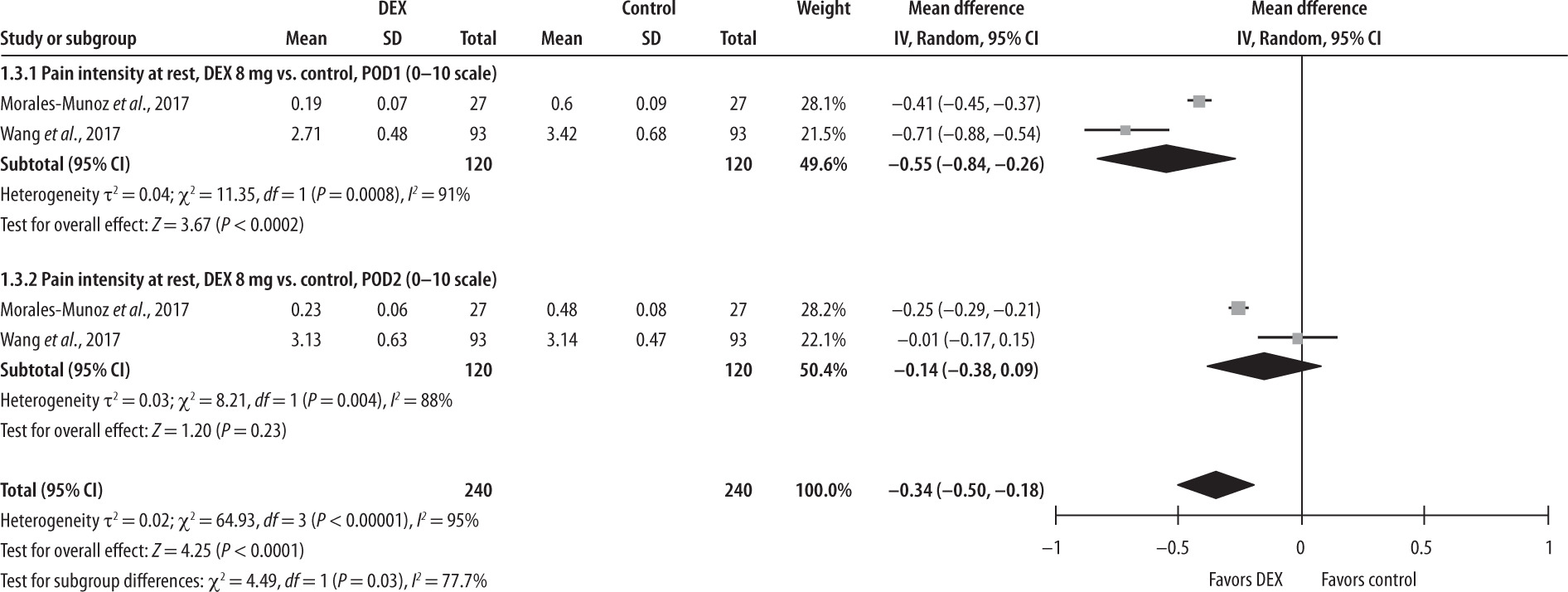
Postoperative pain intensity score at rest measured on POD1 and POD2 for DEX 8 mg vs. control (NRS/VAS, 0–10)
The forest plot in Figure 4 illustrates the compari- son of postoperative pain intensity at rest between the DEX 8 mg and control groups on POD1 and POD2. Only two studies were included in this comparison (DEX = 120, controls = 120). On POD1 the mean difference was –0.55 [95% CI: –0.84, –0.26], indicating a statistically significant lower pain inten- sity at rest in the DEX group compared to the control group, with considerable heterogeneity, I2 = 91%. On POD2 the mean difference was –0.14 [95% CI: –0.38, 0.09], indicating no significant difference between the groups, while the heterogeneity re- mained considerable, I2 = 88%. The model would favor the DEX 8 mg group over the control if a study by Wang et al. [29] were excluded. The overall re- sult of the model favors the DEX 8 mg group over the control group, with MD of –0.34 [–0.50, –0.18], P < 0.0001, and considerable heterogeneity, I2 = 95%. This indicates better pain reduction management with use of DEX 8 mg.
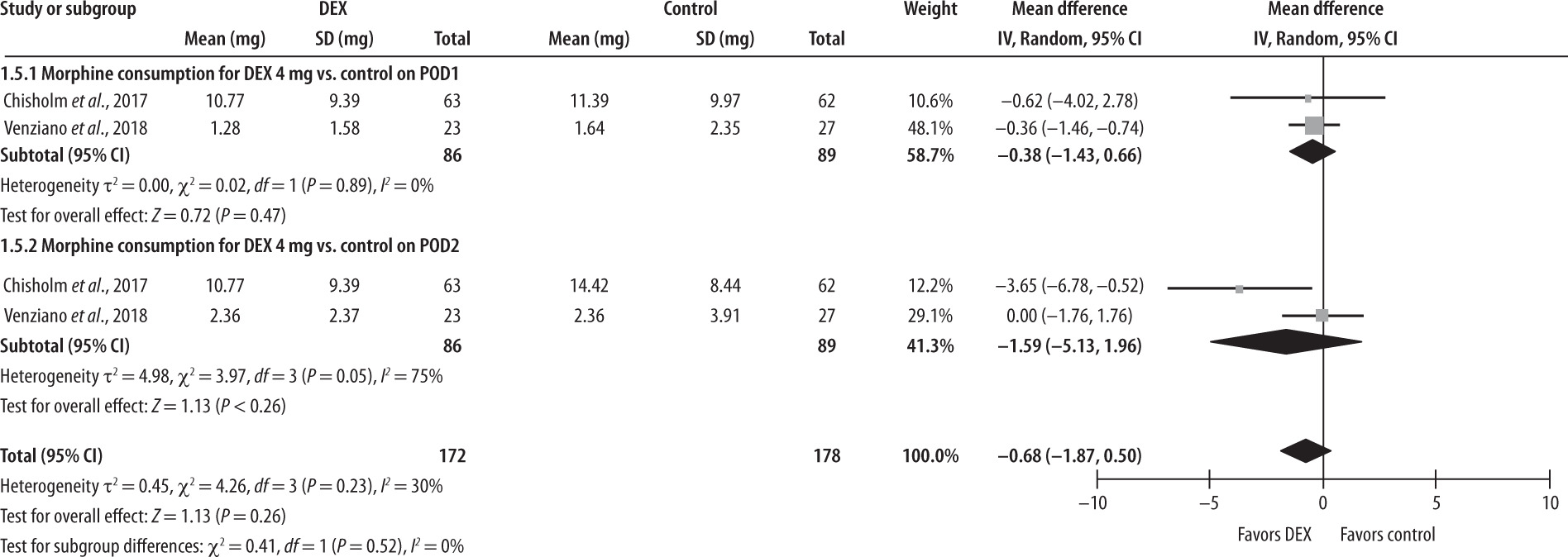
Morphine consumption for DEX 4 mg vs. control
Two studies report the outcome of morphine consumption on POD1 and POD2 (DEX = 86, con- trols = 89), as shown in Figure 5. The forest plot shows that the model does not favor either group; MD with 95% CI is –0.68 [–1.87; 0.5], P = 0.26. There was low heterogeneity (I2 = 30%).
Morphine consumption for DEX 8 mg vs. control
Two studies (DEX = 120, control = 120) reported morphine use in those who received a dose of DEX of 8 mg. The overall effect of the model (Figure 6) does not favor the DEX 8 mg group over the con- trol group (MD with 95% CI is –10.44 [–23.92, 3.03], P = 0.13, I2 = 90%). The sensitivity analysis shows that the result is sensitive to the exclusion of either study, in which case the model favors the DEX 8 mg group. Again, given the limited number of included studies, the results should be interpreted with caution.

Risk of bias
All the studies had a low risk of bias (Table 2). All the studies described adequate randomization and allocation concealment techniques. All the studies were double-blind, and outcome measurements were also performed by blinded study team mem- bers. The missing data were addressed, and all the primary outcomes were reported in each study.
TABLE 2
Cochrane risk of bias
The certainty of evidence was “low” or “moder- ate”. This is presented in the summary of findings (Table 3). Perineural DEX did not improve postopera- tive pain at rest. There are mode rate and low levels of evidence for POD1 and POD2, respectively, due to inconsistency and imprecision. Administration of DEX 4 mg significantly reduced pain on move- ment on POD1, supported by mode rate evidence. No differences were found in pain alleviation on movement on POD2, though the level of certainty is low. As for morphine consumption, there were no differences between the intervention group and controls for both the DEX 4 mg and DEX 8 mg groups. However, our confidence regarding these re- sults is low due to imprecision and inconsistency. We did not assess publication bias due to the scarcity of studies (less than ten).
TABLE 3
Summary of findings
DISCUSSION
This meta-analysis involved seven RCTs and a total of 551 patients. Its primary focus was evalu- ating the effects of DEX as an adjuvant to regional peripheral blocks in knee surgery. The key outcomes considered were pain intensity and opioid require- ments within two POD. These outcomes were as- sessed separately for DEX doses of 4 mg and 8 mg. Almost all the trials, except for one [25], had low or unclear risks of bias.
The findings did not favor the use of DEX at any dose in terms of pain intensity at rest and morphine consumption on POD1. However, administration of 4 mg of DEX showed a reduction in pain with movement by 1.61 points (on a scale out of 10) on POD1. The certainty regarding pain intensity with movement is moderate, given that the result is based only on two studies. There were slight im- provements in pain in those who received the 8 mg dose of DEX.
There are several explanations for such results. One study suggested that many patients suffering from chronic knee pain often rely on opioids before surgery. This can lead to the development of opioid tolerance and opioid-induced hyperalgesia [32]. Ad- ditionally, pain catastrophizing – where patients ex- cessively focus on and exaggerate their pain – may reduce the perceived analgesic effects of DEX. Finally, there might be differences in the effects of different PNBs [6]. Among the various types of PNBs, Kumar et al. [32] suggest the ACB as the preferred choice, as it was associated with reduced length of hospital stay. In contrast, FNB and sciatic nerve block have been observed to negatively affect immediate post- operative knee function, which in turn can extend the recovery period. Our meta-analysis demonstrates somewhat better analgesic effects of perineural DEX in ACB compared to FNB and SNB, according to the sensitivity analyses. However, a Cochrane sys- tematic review of 25 RCTs and 1688 patients did not find any evidence supporting the superiority of ACBs, over sham or FNB [33].
The applicability of these results is relatively broad, extending across various demographic and clinical characteristics. We included studies focused on different age groups, from children and adoles- cents to adults. The included studies were conducted in different geographical locations, thus covering variations in health systems, postoperative care prac- tices, and patient populations across different regions. In terms of surgical and intervention contexts, our results include the most common orthopedic proce- dures, while the diverse regional blocks reflect the va- riety of anesthesia practices. Almost all the studies reported the primary outcome, namely, pain at rest. However, one of the studies lacked blinding of out- come assessors, which could affect the results.
We have found two systematic reviews that as- sess perineural DEX in knee surgery. One system- atic review [17] was focused only on total knee arthroplasty, and out of eight studies, only two evaluated perineural DEX. A Cochrane systematic review [8] included upper and lower limb opera- tions, with only two studies on lower limbs. Both systematic reviews concluded lower pain scores and opioid use within the first POD in the DEX group. The perineural DEX group experienced lower pain levels than the control group 12 hours after sur- gery, with a mean reduction of 2.08 on a 10-point scale. However, there was no clinically significant difference in pain intensity between the groups 24 and 48 hours postoperatively. The perineural DEX group required fewer opioids than the placebo group 24 hours after surgery, with a mean difference of 19.25 mg [8].
Two more systematic reviews studied perineural DEX in other types of surgery. One systematic review of four RCTs focused on the use of the DEX in knee and hip arthroplasties. The authors concluded that it reduced pain and opioid use during the first two days after surgery [18]. Another meta-analysis of nine RCTs also found decreased morphine use, with a mean difference of 8.5 mg [11]. It did not find any benefits regarding postoperative pain intensity. The mean dif- ference did not reach one point out of ten for the out- comes of early (several hours postoperatively) and late (after 24 hours) pain.
The results of these systematic reviews are some- what controversial, probably due to the heteroge- neity of the included studies, e.g. differences in DEX administration and types of surgery. More studies, focusing specifically on perineural DEX in knee sur- gery, are needed to draw more solid conclusions.
Regarding our limitations, the most important one is the modest number of the included trials and low number of participants for each outcome as a re- sult. This affected our level of certainty in evidence. For more definitive conclusions, we need more stud- ies evaluating perineural DEX in knee surgery, par- ticularly assessing postoperative pain on movement. The limited number of trials did not allow us to as- sess publication bias. However, as we included only articles written in English, there could be a consider- able bias in selection of studies. Another limitation of our meta-analysis is the lack of safety assessment of perineural DEX in knee surgery patients. Gluco- corticoids are notorious for causing a range of ad-verse events, the most common of which are infec- tions, delayed wound healing, hyperglycemia, and psychological issues [34].
Implications for further research
Future research should address the adverse events caused by perineural DEX and effects on peri- pheral block duration. Long-term patient-reported outcomes, including quality of life, would also be of interest. Different PNB and the effects of peri- neural DEX in each should be compared to choose the block with the most benefits in knee surgery. The effects of perineural DEX should be compared with the effects of convenient intravenous adminis- tration, already recommended in guidelines for hip surgery [35].
CONCLUSIONS
In this meta-analysis of seven RCTs involving 551 patients, we assessed the analgesic effects of peri- neural DEX as an adjuvant to regional peripheral blocks in knee surgery.
The 4 mg dose of DEX did not significantly re- duce pain at rest on the first POD, but showed a ben- efit in reducing pain during movement, suggest- ing improved postoperative mobility. In contrast, the 8 mg dose provided more effective pain man- agement at rest, indicating its potential for better overall pain management. In terms of morphine con- sumption, neither dose of DEX demonstrated a re- duction in morphine requirements. In knee surgery patients, the use of a higher dose (8 mg vs. 4 mg) of perineural DEX may reduce pain, while a lower dose (under 4 mg DEX) may reduce pain on move- ment. Despite the positive findings, the evidence is limited by the relatively small number of participants included in the analysis.