
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) are procedures with an intermediate risk of post-operative complications, for which the risk of myocardial infarction, cardiovascular death, and stroke, associated with the surgical procedure is 1–5% [1]. In 2022 almost 38 thousand TKA and 65 thousand THA procedures were performed in Poland, and these numbers are expected to increase in following years [2].
Optimal collaboration between the anaesthetic and orthopaedic teams is crucial to improve the quality of medical care, minimise complications and reduce hospitalisation time. Several elements of anaesthetic management with a potential to improve patients’ outcomes have been identified, including optimising preoperative patient education, anaesthetic technique, as well as a transfusion strategy in combination with an opioid-sparing multimodal analgesic approach and early mobilization [3].
Currently, in Poland there is no unified standard of perioperative care for patients undergoing total joint replacement (TJR). Thus, we conducted a survey to identify the patterns of perioperative management of anaesthetists and orthopaedic surgeons and to compare them with existing global recommendations. Our group has previously published a report concerning preoperative care, while in the current study we focus on the intraoperative and postoperative anaesthetic management [4].
METHODS
This was a survey-based study aimed at determining the perioperative anaesthetic management (during anaesthesia and in the postoperative period) in patients undergoing TJR in Poland. The survey was sent to all health care institutions in Poland performing elective TJR procedures in adult patients. A list of health care institutions was obtained from the National Health Fund (in Polish: Narodowy Fundusz Zdrowia – NFZ) data thanks to collaboration with the National Centre for Quality Assessment in Healthcare (in Polish: Centrum Monitorowania Jakości w Ochronie Zdrowia – CMJ). The questionnaire was carried out in two rounds: 17 May – 30 July 2021 and 3 August – 24 August 2021. The study was promoted through websites, social media channels and personal contacts. This paper discusses the results and issues of the survey concerning anaesthesia, analgesic treatment and measurement of myocar-dial injury markers (cardiac troponin) in patients at high risk of cardiovascular complications. The study was approved by the Bioethics Committee of the Jagiellonian University in Cracow – Decision No. 1072. 6120.259.2020 of 24 September 2020.
Survey development
The questionnaire was created after prior analysis of the available literature identifying key elements of anaesthetic management. The questionnaire contained 24 questions, some of which were single-choice and some multiple-choice, which was taken into account in the statistical analysis. The questionnaire was addressed to both medical specialists and medical doctors in specialty training. Any number of anaesthetists from each health care institution could take part in the survey. The questionnaire was created in collaboration with the National Consultant in the field of Anaesthesiology and Intensive Care. In order to reach as many anaesthetists as possible, the form was made available online using the Lime-Survey application (version 3.26.1+210427) [5].
Survey validation
Once the initial version of the survey was created, personal professional contacts were used to provide feedback. Minor modifications were made to the final version (appendix in the supplement). The methodology was described in detail in our previous publication [4].
Statistical analysis
This is a descriptive analysis encompassing types of anaesthesia, adjuvant anaesthetics and postoperative pain control in patients undergoing TJR procedures. Categorical variables are presented as counts with percentages. This was a complete case analysis. Due to the lack of data on the characteristics of 20 respondents, the denominator may vary across analyses in the manuscript. All statistical analyses were performed using R version 4.0.3.
RESULTS
We received responses from 258 anaesthetists out of 112 health care institutions in Poland. Details on the survey participants are summarised in Table 1.
TABLE 1
Characteristics of respondents (n = 238, 20/258 participants did not answer questions on group characteristics)
For anaesthesia in TKA, 86.0% of respondents would use the subarachnoid block (SAB), 11.6% combined spinal-epidural (CSE) and 2.3% general anaesthesia. For THA, 88.0% of anaesthetists use SAB, 7.0% CSE block, and 5.0% use general anaesthesia.
Additional peripheral nerve block for TKA surgery is used by 69.4% of respondents, and 30.6% report not using it routinely. Femoral nerve block (FNB) is the most commonly performed procedure (46.5%), followed by the adductor canal block (ACB) in 33.3% of cases, and sciatic nerve block (SNB) in 12.8%. Infiltration between the popliteal artery and capsule of the knee (iPACK) is used by 8.9% and tibial nerve block (TNB) by 0.4% of respondents. Differences in choosing the type of peripheral blockade based on professional experience are shown in Figure 1. Data on periprocedural analgesia in TJR are summarised in Table 2.
FIGURE 1
Type of peripheral nerve block for total knee arthroplasty, depending on seniority (multiple-choice answers). iPACK – infiltration between the popliteal artery and capsule of the knee
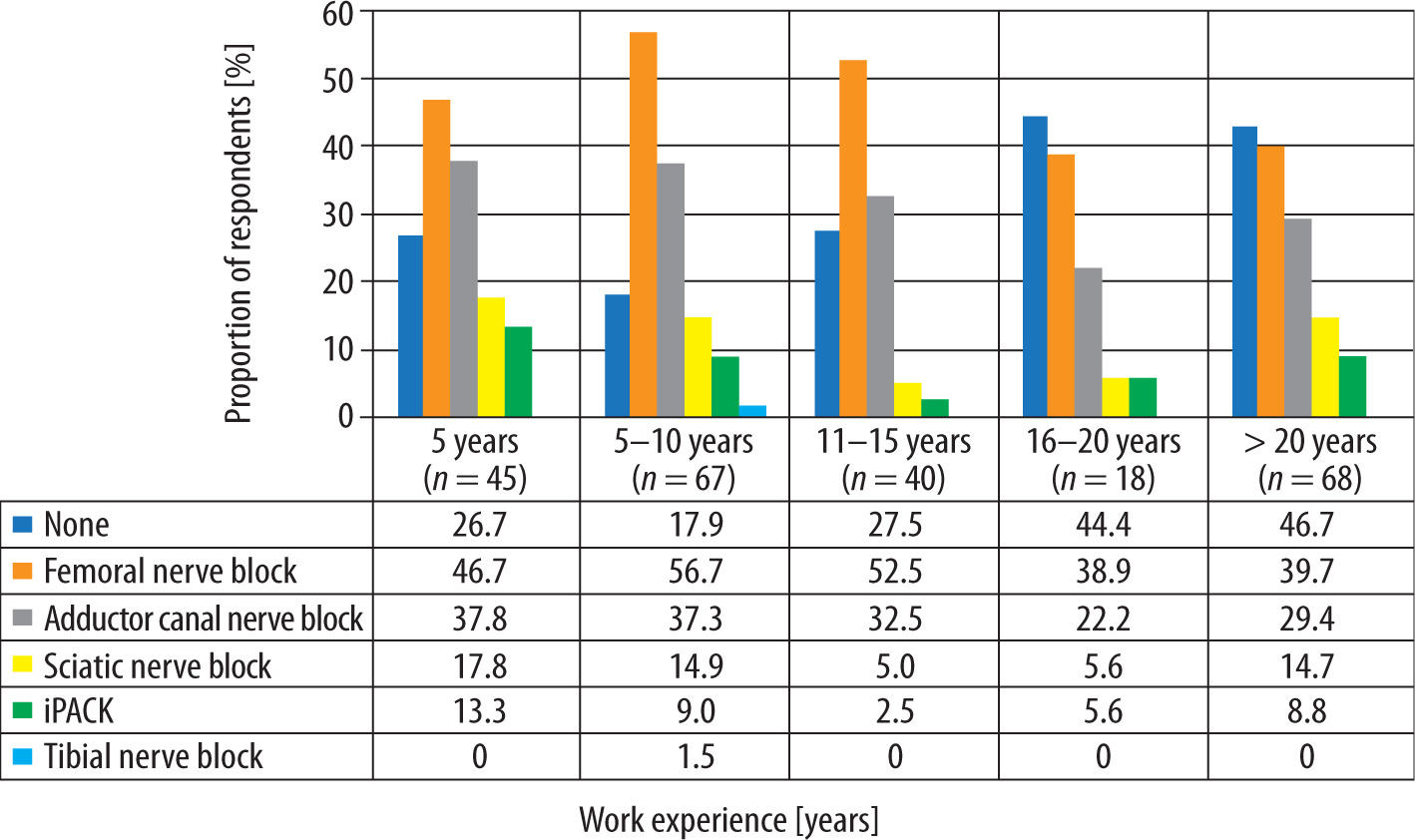
TABLE 2
Periprocedural analgesia in total joint replacement (multiple-choice answers)
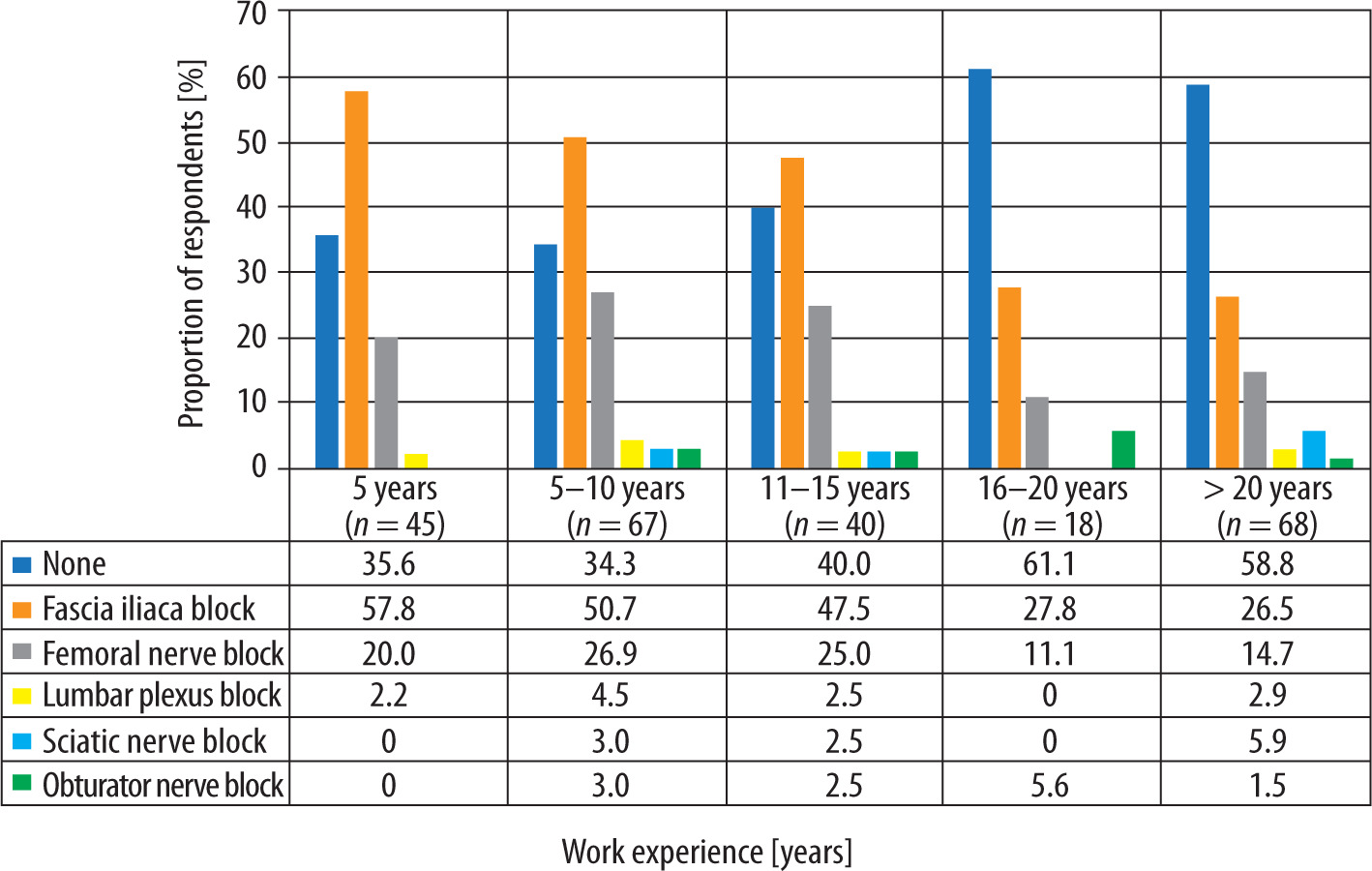
For THA procedures, 44.6% of anaesthetists report that they routinely do not perform any peripheral nerve block. The most commonly performed procedure is the fascia iliaca compartment block (FICB), performed in 42.6% of cases, followed by FNB in 21.3% of cases. SNB is used by 3.1% of respondents, lumbar plexus block (LPB) by 2.7% and obturator nerve block (ONB) by 2.3% of anaesthetists. Differences in choosing the type of peripheral blockade for total hip surgery stratified by professional experience are shown in Figure 2.
FIGURE 2
Type of plexus and peripheral nerve blocks for total hip arthroplasty, depending on seniority (multiple-choice answers)
When asked about the use of intrathecal opioids, 96 (37.2%) anaesthetists responded that they always use opioids, and 64 (24.8%) said they mostly do. Pre-emptive analgesia for TJR procedures is routinely performed by 155 (60.1%) respondents, while it is never carried out by 31 (12.0%) of them. Table 3 shows the analgesics preferred by anaesthetists for multimodal postoperative pain management for TJR.
TABLE 3
Drugs preferred in multimodal analgesia for total joint replacement procedure
A total of 196 (77.2%) anaesthetists do not routinely perform troponin testing in the group at high risk of cardiovascular complications, 40 (15.7%) leave it to the orthopaedists to decide, while 9 (3.5%) perform the determination in the first three days after surgery.
DISCUSSION
In this survey-based study we described perioperative practices used in TJR procedures in Poland. We found that the vast majority of anaesthetists use SAB. Peripheral nerve blocks are less frequently performed for THA procedures for analgesia compared to TKA procedures, regardless of the type of anaesthesia. Local infiltration analgesia (LIA) is performed more often for TKA than for THA. For postoperative pain management, almost all anaesthetists use systemic drugs, regardless of the type of anaesthesia, and more than half use pre-emptive analgesia. The most common systemic drugs of choice are paracetamol, metamizole and opioids. Only a small group of respondents (3.5%) routinely order a cardiac troponin test in patients at high risk of cardiovascular complications in the immediate post-TJR period.
Type of anaesthesia
Numerous studies have been conducted over the years in an attempt to determine the role and safety of anaesthesia in TJR. The scientific data are inconclusive. A consensus issued in 2020 by the Enhanced Recovery After Surgery Society (ERAS) indicates the equivalence of general anaesthesia and SAB [3]. Similar recommendations, endorsed by the European Society of Regional Anaesthesia and Pain Therapy (ESRA), were presented by the procedure specific postoperative pain management group (PROSPECT). This group, formed by surgeons and anaesthesiologists, focuses on improving the management of postoperative pain. PROSPECT demonstrated a reduction in pain in the postoperative period after THA procedures under SAB, compared to general anaesthesia. However, it was emphasised that the current scientific evidence is not sufficient to select one of the techniques as a gold standard [6]. Conversely, the International Consensus on Anaesthesia-Related Outcomes after Surgery Group (ICAROS), in recommendations based on a systematic review and meta-analysis published in 2019, unequivocally identifies SAB as more beneficial, due to reduced complications and lower mortality [7]. The authors of the consensus pointed out that SAB should be the preferred technique, even though it is difficult to make a reliable comparison the technique, as general anaesthesia has changed over the years [7].
The benefits of long-acting intrathecal opioids have been demonstrated in several studies [8]. However, neither ERAS nor the PROSPECT group recommends their routine use because of the high risk of possible side effects: respiratory depression, postoperative nausea and vomiting, and skin pruritus [3, 9]. PROSPECT recommendations allow the use of intrathecal morphine in hospitalised patients when both LIA and ACB are not feasible [9].
In Poland, the vast majority of anaesthetists prefer SAB for TJR. In the absence of conclusive evidence, given the benefits of better postoperative pain control following SAB, this practice seems to be appropriate. According to our results, more than half of Polish anaesthetists use intrathecal opioids, which necessitates longer monitoring of these patients in the postoperative period. Considering available evidence, it seems that, to minimise the risk of com-plications after intrathecal opioids, other methods of analgesic treatment, e.g. regional blocks, should be considered more often. Attention is also drawn to the high number of performed CSEs, despite possible complications, muscle weakness and delayed rehabilitation. According to ERAS and PROSPECT recommendations, epidural technique should not be performed because of side effects [3, 6, 9].
Post-operative pain management
Adequate pain control after TJR procedures is critical for ensuring patient comfort, early mobilisation, rehabilitation and shortening the length of stay (LOS) [6, 9]. Therefore, analgesic treatment should be multidirectional (multimodal), including peripheral nerve blocks, LIA, and intrathecal opioids, in combination with systemic drugs, and planned in advance in an individualised manner [10, 11]. This is particularly relevant for TKA procedures, which are associated with significant postoperative pain [9].
The PROSPECT group has published recommendations for postoperative pain management in patients undergoing TKA (2022) [9] and THA (2021) [6]. The preoperative and intraoperative pharmacological management recommended for TJR is paracetamol, NSAID or cyclooxygenase-2 (COX-2) specific inhibitor, and dexamethasone [6, 9]. Out of the peripheral nerve blocks, ACB performed preoperatively and peri-articular LIA performed intra-operatively are recommended for TKA (a combination of these two techniques is preferred) [9]. However, for THA, a single-shot FICB or LIA is suggested [6]. FICB performed above the inguinal ligament shows greater efficacy [12]. For postoperative pain management in TJR procedures, the continuation of paracetamol and NSAID or COX-2 specific inhibitors is recommended. Opioids should be reserved as rescue analgesics [6, 9]. The ERAS group recommends the use of LIA for TKA procedures, as opposed to THA procedures. Importantly, routine use of peripheral nerve blocks for TKA is not recommended due to the limiting effect on the motor function of the lower limb [3].
We found that more than 50% of surveyed anaesthetists perform peripheral nerve blocks in TKA procedures, and the majority of these are FNB and SNB, which potentially impair lower limb motor function the most. If operators do not perform LIA in TKA, iPACK is recommended. Only about 15% of orthopaedists in Poland perform LIA for TJR. We believe that it may be related to concerns about possible toxic effects of drugs around the operated joint or an increased risk of infection. However, the available studies have not confirmed these concerns. In addition, LIA has no effect on motor function and significantly reduces the need for opioid medication [3, 9].
For THA procedures, almost half of the anaesthetists report that they do not perform any regional block, limiting analgesic treatment solely to systemic drugs. The most commonly performed blocks are FICB and FNB.
In the group of Polish anaesthetists, the number of regional blocks performed in TJR decreases as their professional experience increases.
Systemic analgesics
Expert groups unanimously recommend the use of systemic analgesia. The contraindications should be considered on a patient-by-patient basis [3, 6, 9].
The PROSPECT group and ERAS society do not refer to the use of metamizole (dipyrone). In some countries the drug is not registered for treatment due to possible agranulocytosis. It appears to be a good alternative to NSAID or COX-2 specific inhibitor groups when there is a risk of gastrointestinal bleeding or renal dysfunction [13, 14].
Other drugs such as ketamine, gabapentinoids, and lidocaine are not routinely recommended. In the case of ketamine, efficacy in reducing opioid consumption has been proven, but reliable dosing data are lacking [6, 9]. Gabapentinoids are not recommended because of the risk of adverse effects: delirium, and somnolence, especially in the elderly [6, 9]. In the case of lidocaine, ERAS and PROSPECT recommendations have not mentioned this drug, probably because the efficacy in TJR has not been proven [3, 6, 9].
Magnesium, so far neglected in recommendations, also deserves attention. There is evidence of a reduction in pain not only in the postoperative period [15–17], but also at a distant time after surgery (even after one year) in a group of patients who received an intravenous infusion [16].
The study showed that the systemic drugs most commonly used by Polish anaesthetists in TJR procedures are: paracetamol, metamizole, opioids and NSAIDs. Metamizole is used far more frequently than NSAID/COX-2 inhibitors, presumably out of fear of haemorrhagic complications. Only a small group of respondents use systemic glucocorticoids (GCs), which have a proven track record in pain management and also show multidirectional benefits. With favourable evidence for magnesium, its more frequent use should be considered. Postoperatively, anaesthetists routinely turn to opioids in up to 80% of cases. Opioid overuse in clinical practice urgently necessitates change in the planning of perioperative analgesic treatment.
Cardiac troponin test
In 2022, new guidelines from the European Society of Cardiology (ESC) [18] were published, which changed the recommendation for routine perioperative troponins screening before intermediate and high-risk non-cardiac surgery. Routine performance of these tests offers the possibility of early recognition of significant cardiovascular complications in the perioperative period.
However, these guidelines have not yet been implemented in clinical practice. In Poland, only 3.5% of anaesthetists routinely measure troponin levels in the first three days after surgery.
Weakness
Despite intensive effort to achieve a maximal response rate, our analysis does not perfectly represent the population of Polish anaesthetists involved in care of patients undergoing TJR.
Strength
The questionnaire addressed various issues of intraoperative and postoperative anaesthetic care. With the help of the National Health Fund and the National Centre for Quality Assessment in Healthcare, we were able to reach all health care institutions in Poland performing TJR. We believe that the results represent current practice among Polish anaesthetists in caring for TJR patients.
CONCLUSIONS
Based on the survey and analysis of available guidelines and global recommendations, elements of intraoperative and postoperative anaesthetic management were identified, the modification of which will improve the safety and quality of TJR procedures performed.
The following conclusions were formulated:
the preferred type of anaesthesia in TJR is SAB,
CSE in primary TJR should not be performed, because of side effects,
in TKA procedures, the recommended management is LIA with ACB and systemic drugs; the frequency of performing FNB or SNB should be limited due to the impact on lower limb motor function,
in THA procedures the recommended management is LIA or FICB and systemic drugs,
operators should be encouraged to perform LIA, especially in TKA,
regional blocks are performed too rarely, especially by anaesthetists with longer experience,
cautious use of opioids in postoperative pain management should be recommended,
improved analgesic effects can be seen by increasing the number of regional blocks performed, increasing the number of NSAID/COX-2 inhibitor drugs ordered, GCs given intraoperatively, and intraoperative intravenous magnesium infusions,
the use of pre-emptive analgesia reduces the risk of persistent postoperative pain; better and earlier planning of analgesic treatment should be individualised,
in patients at risk of cardiovascular complications, troponin levels should be measured routinely before surgery and for 48 h after TJR.
The results of the current study support the need to prepare standardised perioperative management guidelines for TJR.