
Prostate cancer is one of the most common malignant diseases of men. It contributes to almost 15% of all cancers detected in men [1]. A radical prostatectomy is the treatment of choice, despite the fact that there are many other therapies. Prostatectomy affords a more than 10-year life expectancy [2]. In addition, laparoscopic surgery is associated with a significant reduction in postoperative pain and opioid consumption, lower morbidity, faster recovery, and a shorter hospital stay [3]. Nevertheless, although laparoscopic prostatectomy is minimally invasive, postoperative pain is still present [4].
Well-being in the postoperative period mainly depends on the particular analgesic treatment, which influences postoperative recovery. Current recommendations indicate that pain-relieving treatment should be multimodal. The treatment should include regional analgesia, non-opioid agents, and opioids. These treatments must ensure satisfactory pain control in the postoperative period.
Opioids have many side effects that could complicate the postoperative period. Opioids may increase health care costs (e.g., nausea, vomiting, and ileus) [5]. Opioids are well known for their immuno-suppressive effects, especially in patients with cancer, potentially increasing the risk of infection and cancer recurrence [6]. After laparoscopic prostatectomy, regional anesthesia techniques should be used to diminish pain in the postoperative period and thereby to reduce opioid consumption during recovery [7, 8].
The quadratus lumborum block (QLB) was first described by Rafael Blanco in 2007. It was later categorized into approaches QLB 1, 2, and 3, with another modification being the intramuscular QLB. These approaches are distinguished by the location of the tip of the needle and the position of the local anesthetic injection [9]. A considerable amount of data [10, 11] supports the effectiveness of QLB in reducing pain in the postoperative period and in reducing opioid consumption after many different types of operations.
Erector spinae plane (ESP) block is a relatively new interfascial block used for postoperative pain and chronic neuropathic pain relief in the thoracoabdominal region. The primary indication for the ESP block was treatment of chronic pain. However, the ESP block has advantages in the postoperative periods that follow many thoracic and abdominal operations [12, 13]. The main target of ESP block is the dorsal and ventral rami of the thoracic and abdominal spinal nerves; blockade at these sites diminishes pain after surgery.
To the best of our knowledge, there is no published comparison of the efficacy of ultrasound-guided bilateral ESP block versus bilateral QLB after laparoscopic prostatectomy. Thus, we used the Numeric Rating Scale (NRS) to measure postoperative pain and total opioid consumption in the first 24 hours after laparoscopic prostatectomy for patients who received the ultrasound-guided bilateral ESP block and patients who received the bilateral QLB.
METHODS
The Bioethics Committee of the Jagiellonian University in Cracow, Poland approved this study and the human subject protocol on March 23, 2022 (No. 1072.6120.32.2022). All methods adhered to the principles outlined in the 2013 Declaration of Helsinki. The study was registered at ClinicalTrials.gov (NCT05446727) on July 3, 2022, and the first patient was enrolled on July 5, 2022. Written informed consent was obtained from all subjects. This study was a single-center, prospective, randomized controlled trial involving patients who underwent laparoscopic radical prostatectomy at the University Hospital in Cracow from May 2022 to December 2023. The registered trial was designed to include patients undergoing various abdominal procedures.
The present manuscript reports a pre-specified subgroup analysis restricted to male patients undergoing laparoscopic radical prostatectomy. Patients were stratified into groups according to the type of surgical procedure and the underlying disease prior to enrollment in the study. Information regarding the groups is available in the ClinicalTrials registry. All study participants provided written informed consent to participate voluntarily.
Inclusion and exclusion criteria
Men over 18 years of age with a body mass index (BMI) of less than 40 kg m–2, who underwent laparoscopic radical prostatectomy within the study period, were included in the study and classified as ASA I–III.
The exclusion criteria were the following:
patients who refused to participate in the study,
patients with contraindications to blocks, such as infection at the site of needle insertion, empyema, tumor occupying the thoracic paravertebral space, coagulopathy, bleeding disorders, or therapeutic anticoagulation,
patients unable to use a patient-controlled analgesia pump because of comprehension barriers,
patients with a known allergy to local anesthetics,
patients with chronic pain syndromes,
patients with chronic opioid use.
Before laparoscopic radical prostatectomy, patients were randomized and assigned to one of two equal groups: Group I received an ultrasound-guided ESP block with 30 mL of 0.35% ropivacaine on each side and Group II received an ultrasound-guided QLB1 with 30 mL of 0.35% ropivacaine on both right and left sides. Both groups received their blocks before undergoing laparoscopic prostatectomy.
Randomization was performed using a computer-generated sequence prepared in Microsoft Excel 2016 with a block randomization procedure to ensure balanced group sizes throughout the study. The allocation list was prepared in advance and made available to the attending anesthesiologist immediately prior to induction of anesthesia, in order to perform the assigned block. No formal allocation concealment protocol was applied. Patients and anesthesiologists were therefore aware of the block performed, which could have introduced a risk of performance bias. However, surgeons and postoperative care nurses, who were responsible for outcome assessment, remained blinded to the intervention. Pain intensity was assessed using a standardized NRS protocol with consistent verbal instructions prior to each measurement. Statistical analysis was conducted by an independent statistician blinded to group allocation.
Protocol modification
The original study protocol specified the placement of catheters for compartment blocks; however, due to the unavailability of appropriate equipment, this procedure could not be implemented. For logistical reasons, the regional anesthesia technique (type of QLB) was modified. Furthermore, owing to the specific formulation of the local anesthetic preparation supplied by the institutional pharmacy, the concentration was adjusted from 0.375% ropivacaine to 0.35% ropivacaine. The postoperative observation period was also reduced from the initially planned duration to 24 hours. All protocol amendments were prospectively registered and updated at ClinicalTrials.gov. All participants enrolled in the study were managed in accordance with the revised methodology.
ESP block technique
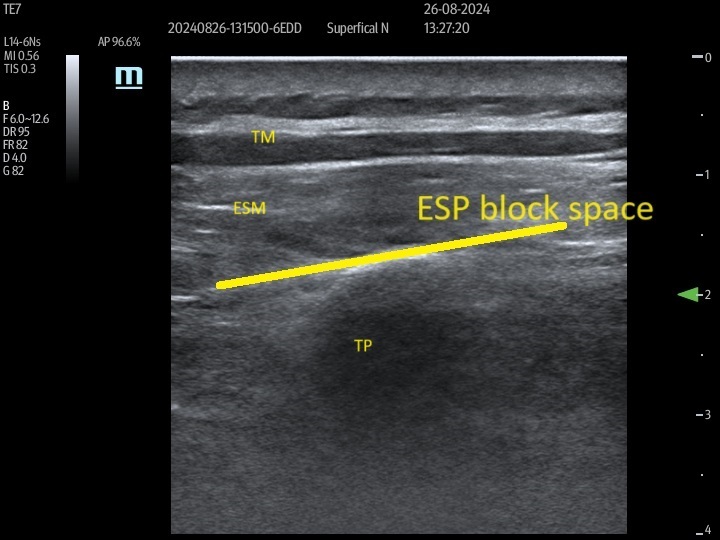
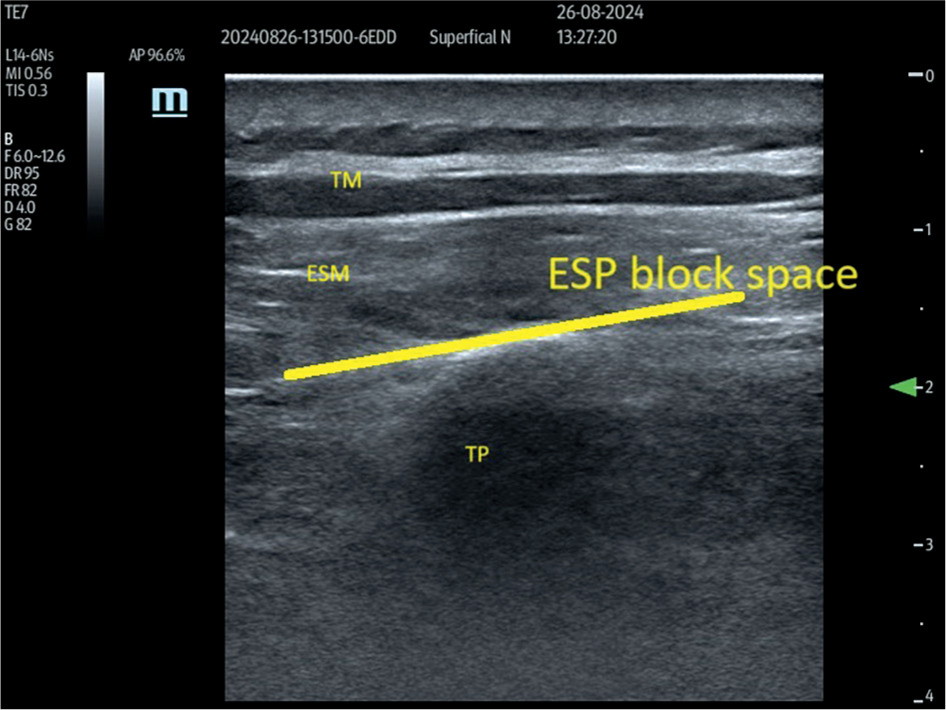
The ESP block was performed with the patient in a sitting position. After skin disinfection, a linear high-frequency (L14–6NS) ultrasound probe (Mindray, UMT-400, Mindray Building, Keji 12th Road South, High-Tech Industrial Park, Nanshan, Shenzhen, People’s Republic of China), covered with a sterile sheath, was positioned sagittally 1–2 cm lateral to the midline at the level of the ninth thoracic vertebra (T9). The T9 level was earlier identified by palpating the spinous process of the seventh cervical vertebra and counting down nine intervertebral spaces. After identifying the erector spinae muscle (ESM) and transverse process, a 21-gauge needle (Echoplex+ REF 6194.853 85 mm) was inserted deep into the ESM in a cranio-caudal direction, using an in-plane technique (Figure 1). The needle was advanced, ensuring that it crossed all muscle layers until it contacted the transverse process. Correct needle placement was confirmed by administering 0.5–1 mL of local anesthetic. After ensuring negative aspiration for blood, 30 ml of 0.35% ropivacaine was injected slowly deep into the ESM. This procedure was performed bilaterally on each patient.
QLB technique
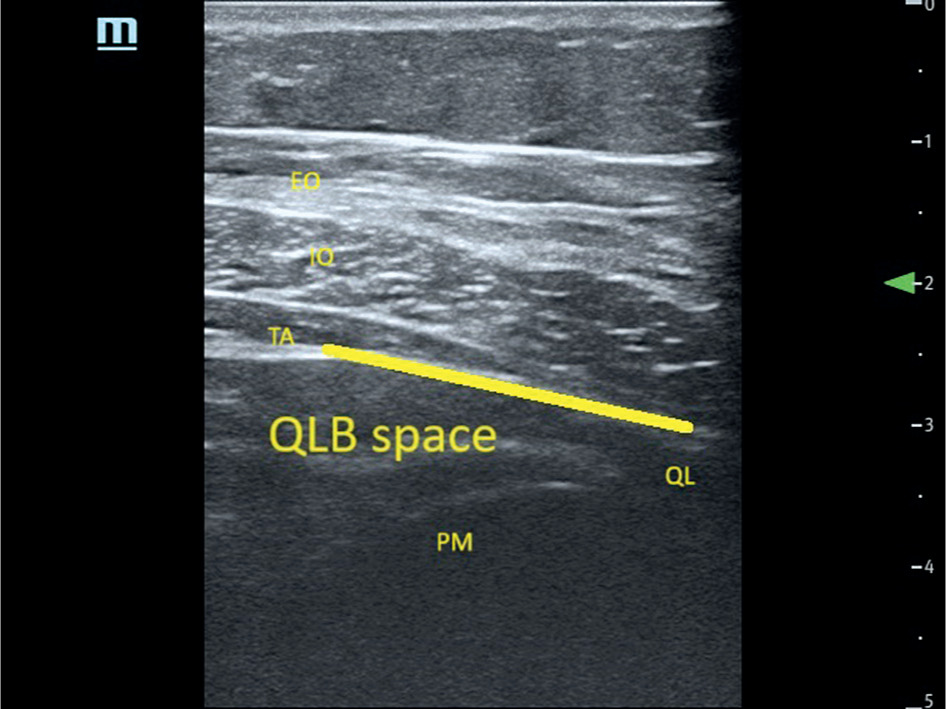
Patients were placed in the lateral decubitus position. After skin disinfection, a linear high-frequency (L14–6NS) ultrasound probe (Mindray, UMT-400 Mindray Building, Nanshan, Shenzhen, People’s Republic of China) guarded with a sterile cover was set above the iliac crest and shifted cranially until the three abdominal wall muscles were distinguished. Then, it was moved medially until the latissimus dorsi and quadratus lumborum muscles (QLM) were shown within identical short-axis views. A 21-gauge needle (Echoplex+ REF 6194.853, 85 mm) was inserted from the edge of the probe using an in-plane technique and advanced into the fascia over the QLM. After ensuring negative aspiration for blood, 30 mL of 0.35% ropivacaine was injected slowly into the fascial interspace between the QLM and internal oblique muscles (Figure 2). An experienced anesthesiologist performed this procedure bilaterally on each patient.
Definitions of studied groups
The ESP group was composed of patients who had the bilateral ESP block, and the QLB group consisted of patients who had the bilateral QLB.
FIGURE 1
Erector spinae plane (ESP) block block as seen on ultra-sound examination. Para sagittal ultrasound view at the T9 level in a slightly more medial plane prior to ESP block showing trapezius muscle and erector spinae muscle. The line shows the target site of the block. TM – trapezius muscle, ESM – erector spinae muscle, TP – transverse process
Induction and maintenance of anaesthesia
Standard monitoring during the procedure included arterial oxygen saturation, ECG, and noninvasive arterial blood pressure. Premedication was not used. The standard anesthesia consisted of propofol (1.5–2 mg kg–1 body weight IV) for induction and an infusion of remifentanil using a plasma target-controlled infusion with a calculated plasma level of 1–6 ng mL–1. Rocuronium (0.6 mg kg–1 body weight IV) was administered prior to intubation. Rocuronium was used to provide neuromuscular blockade throughout the operation, and the total dosage was guided by the train-of-four (TOF) index to maintain muscle relaxation. Anesthesia was maintained with desflurane (MAC 1–1.5). In all groups, desflurane end-tidal concentrations were titrated according to the real-time electroencephalography monitor to achieve a bispectral index value between 40 and 60. Mechanical ventilation was delivered with a tidal volume of 6–8 mL kg–1 ideal body weight. The end-tidal carbon dioxide concentration was monitored and kept within the 35–45 mmHg range with modification of the respiratory rate. Postoperative nausea and vomiting (PONV) prophylaxis was achieved with intravenous dexamethasone (0.1 mg kg–1 IV) at induction and intravenous ondansetron (0.1 mg kg–1 IV) 30 minutes before the end of surgery.
FIGURE 2
Ultrasound image of the approach to quadratus lumborum block (QLB). The line shows spaces where local anesthetic spread from the posterior layer of the thoracolumbar fascia on the quadratus lumborum (QL) muscle. TA – transversus abdominis muscle, IO – internal oblique muscle, EO – external oblique muscle, PM – psoas major muscle
Postoperative analgesia
Before surgery, all patients received a combination of intravenous analgesics: magnesium sulphate 2 g, paracetamol 1g, and metamizole 2.5 g. This regimen was repeated every 6 hours for paracetamol and every12 hours for metamizole. Additionally, all patients received 2 mg of intravenous oxycodone 15 minutes before the end of surgery. Prior to surgery, all patients were instructed on the use of the patient-controlled analgesia (PCA) pump (B Braun Perfusor Space, B Braun Melsungen AG, 34209 Melsungen, Germany). The intravenous PCA pump delivered a bolus of 2 mg of oxycodone only on demand, with a 10-minute lockout time. Patients were instructed to use the pump if the NRS score (NRS 0–10/10) was ≥ 4.
Primary endpoint
As the primary outcome parameter, we evaluated cumulative oxycodone consumption within the first postoperative 24 hours.
Secondary endpoints
Secondary outcome parameters were the following: (1) NRS, (2) incidence of PONV during the first 24 postoperative hours, (3) dosage of remifentanil during the operation, (4) estimated blood loss and operation time, (5) volumes of fluids given intraoperatively, and (6) time to patient awakening.
Data analysis
We conducted a pilot study to determine the sample size needed for adequate statistical power. For the first 10 patients, randomized to the ESP and QLB groups, we measured oxycodone consumption between groups in the 24-hour period following the operation. We found a mean oxycodone consumption of 29 mg with a standard deviation of 14.00 mg in the ESP group and 38 mg with a standard deviation of 18.28 mg in the QLB group. We used these data to calculate that 104 patients were required (52 in the QLB group and 52 in the ESP group) to achieve the desired statistical power (power of 0.8 with an α error of 5%). Power analysis was calculated using Open Source Epidemiologic Statistics for Public Health. Our sample size calculation was based on a small pilot study and targeted detection of a 9 mg difference in oxycodone consumption between groups. Smaller, yet potentially clinically meaningful differences could have been missed, introducing a risk of type II error. Therefore, our findings should be interpreted with caution, and larger trials are needed to confirm these results.
Quantitative variables were summarized using descriptive statistics, such as mean, standard deviation, median, quartiles, and minimum and maximum values. Qualitative variables were presented as absolute frequencies and percentages for all possible values of these variables. Qualitative values were compared between the two groups using the χ2 test (with Yates’s correction for 2 × 2 tables) or Fisher’s exact test when the assumptions for the χ2 test regarding the so-called expected numbers were not met. The comparison of the values of quantitative variables between the two groups was performed using the Mann-Whitney U test. Correlations between quantitative variables were analyzed using Spearman’s rank correlation coefficient. A one-way analysis of the influence of quantitative characteristics on a dichotomous variable, e.g., taking only two possible values, occurrence or absence of extensive bleeding, was performed using logistic regression. The significance level of 0.05 was adopted for the analysis, so that all P-values below 0.05 indicated significant relations. The analysis was performed in R, version 4.3.2 [14].
RESULTS
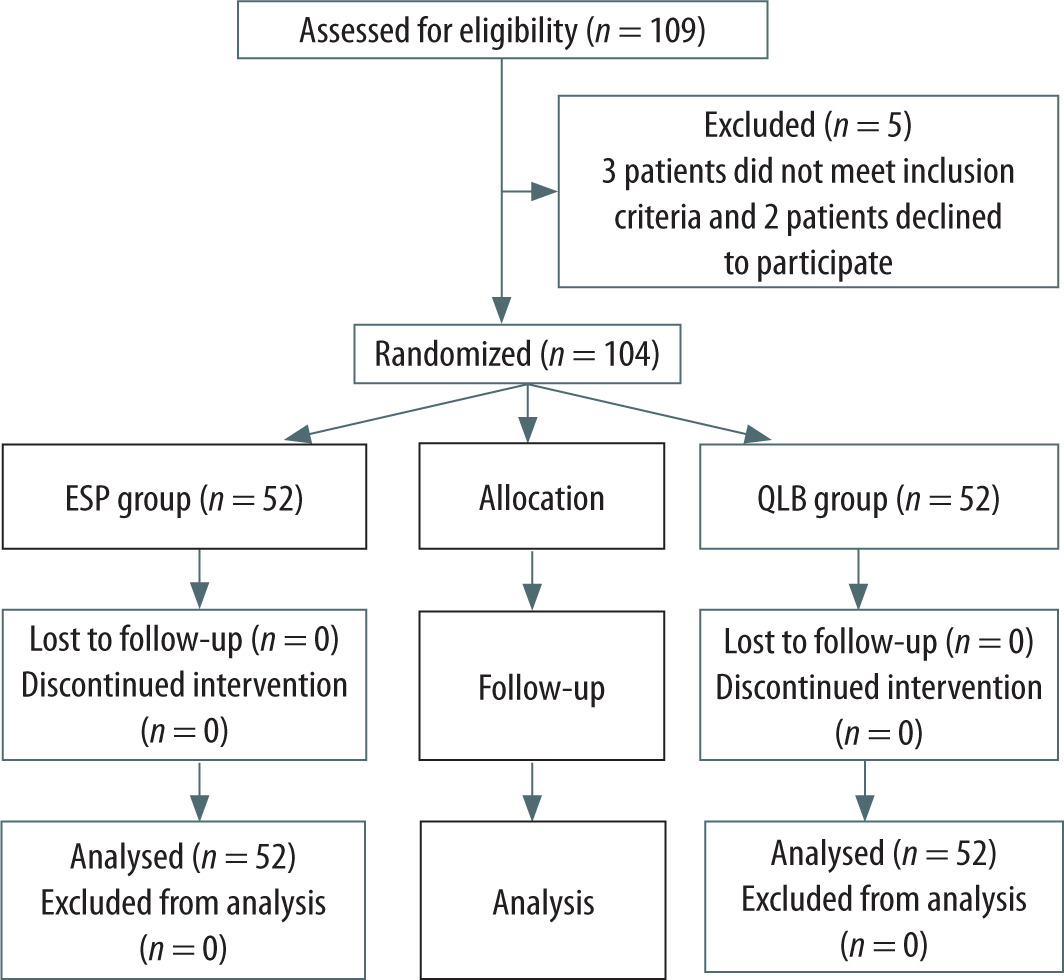
Between May 2022 and December 2023, 109 participants underwent laparoscopic radical prostatectomy under general anesthesia. Three patients did not meet the inclusion criteria, and two patients declined to participate (Figure 3). After providing informed consent, 104 patients were enrolled and randomized. There were 52 patients in the ESP group and 52 in the QLB group. The demographic and anesthesia-related characteristics of the groups were similar (Table 1).
Mean dose of oxycodone, number of requested boluses, mean time of surgery, estimated blood loss, and mean dose of remifentanil are presented in Table 2. For our primary outcome of 24-hour opioid consumption, the difference between groups with its 95% CI, for the ESP group was 17.32–27.56 mg and for the QLB group 22.04–31.07 mg. The MannWhitney U test was used to compare oxycodone consumption between groups.
Pain was evaluated using the NRS at 1, 2, 6, 12, and 24 hours after surgery (Table 3 and Figure 4).
Regarding secondary outcomes, no significant differences were found between groups in the incidence of PONV. Intraoperative opioid requirements (Table 2) were comparable in both groups. Similarly, recovery parameters such as time to extubation, duration of PACU stay, and length of hospital stay did not differ significantly between ESP and QLB groups. These findings suggest that both blocks could provide a broadly similar perioperative profile beyond postoperative analgesia.
Two ESP group patients and three patients in the QLB group experienced PONV. There was no statistically significant difference between the groups (P = 1).
We considered prolonged awakening as an emergence from anesthesia time longer than 10 minutes after the end of the procedure. Only two patients in the QLB group experienced prolonged emergence, but this difference was not statistically significant (P = 0.496).
No complications, such as hypotension, arrhythmia, or allergic reaction, were observed during the intraor postoperative periods of any patient. Neither block-related complications nor side effects of local anesthetics were observed postoperatively.
DISCUSSION
The main aim of the current study was to measure and compare the efficacy of the analgesic action in the perioperative period between the QLB or ESP block in patients undergoing laparoscopic prostatectomy under general anesthesia. We hypothesized that the application of plane blocks after abdominal surgery may reduce pain in the postoperative period. To the best of our knowledge, this study is the first randomized, prospective investigation comparing the ESP block with the QLB for postoperative analgesia in laparoscopic prostatectomy. There were no block-related complications such as perforation, hematoma, infection, or significant hemodynamic instability.
Our main finding was that both the ESP block and QLB provided similar and satisfactory analgesia in the early postoperative stage. There was no difference in opioid consumption between the two groups during the postoperative period. Additionally, we did not find differences in NRS scores regardless of the type of block. Our findings suggest that, although both blocks are safe, they may not provide sufficient stand-alone analgesia for laparoscopic prostatectomy, highlighting the need for adjunctive analgesic strategies. Similarly, intraoperative remifentanil consumption did not significantly differ between the groups.
Lemoene et al. [3] focused on pain management following surgery for prostate cancer and recommended a multimodal approach, particularly with regional analgesia. The investigators suggested the transversus abdominis plane (TAP) block as the first choice regional technique for laparoscopic prostatectomy. However, the QLB may also be indicated because it reduces intraoperative medication and has a role in postoperative multimodal analgesia. The needle tip was localized at the ante rolateral border of the QLM at its junction with the transversalis fascia, and the local anesthetic was injected.
TABLE 1
Demographic and anesthesia-related characteristics
| Factor | ESP group (n = 52) | QLB group (n = 52) |
|---|---|---|
| Age (years) | 65 ± 7 | 66 ± 6 |
| Body mass (kg) | 85 ± 11 | 85 ± 14 |
| Height (m) | 1.78 ± 5 | 1.75 ± 5 |
| BMI (kg m–2) | 27 ± 3 | 28 ± 4 |
| ASA | II – 39; III – 13 | II – 40; III – 12 |
TABLE 2
Mean dosage of oxycodone, number of requested boluses, mean time of surgery, estimated blood loss and mean dosage of remifentanil
TABLE 3
NRS scores at 1, 2, 6, 12, and 24 hours after surgery and total score. NRS (Numeric Rating Scale)
Thus, the QLB can provide effective postoperative analgesia after abdominal surgery. Evidence suggests possible improved visceral pain coverage [15]. Furthermore, the block is safe, because the needle tip is positioned far away from abdominal organs and large blood vessels.
There are data supporting the beneficial effects of TAP regional anesthesia, but there are no direct comparisons between the TAP block and the QLB. The TAP block became popular because it is easy to put in place [16]. Gao et al. [17] reported that, compared with the TAP block, the QLB is more effective in decreasing opioid consumption in the postoperative period. Hu et al. [18] compared pain levels of patients after radical prostatectomy with or without the QLB. In the postoperative period, at 2, 4, 6, and 12 hours, patients in the QLB group had lower NRS scores than patients in the group without the block. Hu et al. [18] did not demonstrate a correlation in the amount of remifentanil administered between the two groups during the operation. Nevertheless, the cumulative dose of sufentanil was notably lower in the QLB group than for patients without the block. Moreover, patients without the block had higher nausea scores. In our study, there was no significant difference between the groups in remifentanil consumption during the operation. Wang et al. [19] examined pain and opioid consumption after transurethral resection of the prostate. The group of patients with the QLB had lower sufentanil consumption. Furthermore, there was a reduction in the VAS scores at 1, 4, 8, 12, and 24 hours in the QLB group after surgery, as well as a shorter hospital stay compared with patients without the block.
Jin et al. [20] reported diminished opioid consumption in the postoperative period after caesarean delivery and renal surgery. These data suggested a positive effect of the QLB on pain scores and time to rescue analgesia; nevertheless, there was significant heterogeneity, and the quality of the evidence was low [20].
The effectiveness of the ESP block was confirmed after robotic-assisted radical prostatectomy [21]. The ESP block ensured lower NRS scores, compared with intravenous infusion of analgesic drugs. Moreover, recovery time from postoperative ileus was significantly shorter in the ESP group compared with the group that received intravenous analgesia. Buo nanno et al. [21] also noted that the ESP block reduced the need for supplemental total dosage of sufentanil and end-tidal volatile anesthetic concentrations, thereby ensuring hemodynamic stability.
Also, the ESP block group had lower discomfort due to tenesmus. Conversely, the effect of the ESP block differed markedly in open radical prostatectomy. Dost et al. [22] reported similar results in NRS scores for patients undergoing open radical prostatectomy, whether they had the ESP block or a placebo, except during the first hour, when pain was lower in the ESP group. The difference may be due to the various surgical approaches; open surgery provokes more pain than robotic-assisted surgery.
In our study, we compared two blocks: ESP and QLB. We did not find any difference in pain and opioid consumption between these groups of patients. Aygun et al. [23] were the first to compare the QLB and the ESP block. They included 80 patients after cholecystectomy, and the results did not show a statistically significant difference in morphine consumption at the 1st, 6th, 12th, and 18th hours after the operation. Numeric Rating Scale scores were lower in the ESP group at the first hour (P < 0.001); however, NRS scores were similar at 6, 12, 18, and 24 hours after the operation. In our data, there was no statistically significant difference in the NRS scores after surgery. The main difference between our study and that of Aygun et al. [23] was the localization of the drug injected for the QLB. We preferred the QLB1, whereby the local anesthetic was deposited on the anterolateral QL muscle, between the deep and middle layers of the thoracolumbar fascia. Aygun et al. [23] used the QLB2 modification, whereby the local anesthetic was placed on the posterolateral QL muscle, between the superficial and middle layers of the thoracolumbar fascia.
Baran et al. [24] compared the QLB and the ESP block for women after hysterectomy. Ninety-one patients were included in three groups: ESP block, anterior QLB, and control. In the ESP and QLB groups, VAS scores at 2, 6, and 12 hours postoperatively were significantly lower than scores in the control group. However, there was no statistically significant difference between the ESP and QLB groups. The opioid consumption in the QLB and ESP groups was also significantly lower than in the control group. There was a lower occurrence of postoperative nausea and vomiting in the QLB and ESP groups than in the control group, although there was no significant difference between the ESP and QLB groups. In our study, we did not find significant differences in postoperative nausea between the studied groups.
Fakhry et al. [25] compared the QLB and ESP block in patients after laparoscopic resection of colorectal cancer. They found that the time required to perform the technique was remarkably shorter in the ESP group. There were no significant differences in the VAS scores between the groups at 30 min, 6 h, and 24 h at rest after surgery. Nevertheless, the VAS scores significantly differed at 1, 3, and 12 hours after surgery between the groups (the ESP group had lower values than the QLB group). There was no significant difference in the VAS scores during the movement between the study groups.
In a meta-analysis, Qin et al. [26] found that 24 h postoperative IV morphine-equivalent consumption was lower for patients receiving ESP than for patients receiving the QLB (MD –2.307 mg; 95% CI: –4.577 to –0.038; P = 0.046; and I2 = 96.5%), although the reduction did not reach a clinically meaningful difference.
Liheng et al. [27] performed a meta-analysis to compare ESP block and TAP block in patients after abdominal surgery. They reported that the ESP block provided good analgesic efficacy, similar to the efficacy of the TAP block.
The TAP block is easy to perform, and it is proven to significantly lower pain and opioid consumption after surgery. However, TAP does not block visceral pain because of the localization of the local anesthetic [28]. In theory, the ESP block should influence both somatic and visceral analgesia compared with the TAP block.
Onay et al. [29] compared the QLB2 with the ESP block in patients after undergoing open nephrectomy. They included 40 patients and found results similar to our findings for NRS scores and opioid consumption. Notably, we included twice as many patients while observing similar findings.
In addition to the primary outcomes, we analyzed secondary endpoints including PONV, intraoperative opioid use, and recovery-related variables. No statistically significant differences were observed between the ESP and QLB. These results are consistent with previous reports suggesting that both blocks can provide stable perioperative conditions without major differences in recovery parameters. However, given the limited sample size, the study may not have been adequately powered to detect small differences in these secondary outcomes.
LIMITATIONS
The main limitation of this study was the lack of a control group. We designed this study as a simple randomized controlled trial. Given that many studies showed that blocks reduce opioid consumption and NRS scores, we decided to omit the control group. Additionally, the local anesthetic dosage differed across various studies. None of our patients presented with systemic local anesthetic toxicity. However, further studies are needed to establish ideal concentrations and volumes of local anesthetic solutions.
Another limitation is that patients and anesthesiologists were not blinded to group allocation, which could have introduced performance and detection bias. The randomization procedure also did not include allocation concealment. Although surgeons, postoperative nurses, and the statistician remained blinded, the possibility of bias cannot be completely excluded.
A further limitation concerns the follow-up period. In the original trial registration, the primary endpoint was planned for 48 hours after surgery. In the present analysis, we restricted the observation period to 24 hours. This change was motivated by the typical recovery trajectory after laparoscopic radical prostatectomy, where patients are mobilized early and often discharged within 24–36 hours. Therefore, the 24-hour endpoint better reflects the relevant clinical practice setting. However, we acknowledge that this decision may have limited our ability to detect later differences in analgesic efficacy between groups. Future studies with extended follow-up (48–72 hours) are warranted to fully assess delayed onset pain and the duration of block effectiveness.
CONCLUSIONS
Our results showed no statistically significant difference between the ESP and QLB in postoperative oxycodone consumption and pain scores within 24 hours after surgery. While these findings suggest that both blocks may provide comparable levels of analgesia in this context, we emphasize that our study was not designed or powered as an equivalence or non-inferiority trial. Therefore, absence of a significant difference should not be interpreted as proof of equivalence. Rather, our findings indicate that within the limitations of this study, the ESP and the QLB yielded broadly comparable clinical outcomes.