
Supraglottic airway devices (SGAs) are routinely used in general anesthesia and emergency medicine [1, 2]. Introduced in the 1980s as a less invasive alternative to endotracheal intubation, the laryngeal mask (LM) remains the most commonly used SGA [3, 4]. The primary advantages of SGAs are that they require less expertise to insert and are associated with reduced airway trauma and fewer complications compared with tracheal intubation [1, 5]. SGAs are also important tools in difficult airway management and are currently recommended in various guidelines for rescue ventilation after failed intubation [1, 6, 7].
Given that airway management is a potentially life-saving procedure, healthcare professionals working in acute care medicine should be taught in its basic principles. Previous reports have shown that inexperienced healthcare professionals can be taught to use a LM more easily than to perform tracheal intubation [2, 8]. It is generally accepted that novice operators should be trained on simulators before performing airway interventions on patients. Consequently, LMs have been widely evaluated in simulation settings, comparing success rates and time to ventilation among non-specialists such as paramedics, medical students, non-anesthesiologists, and medical assistants [5, 9, 10].
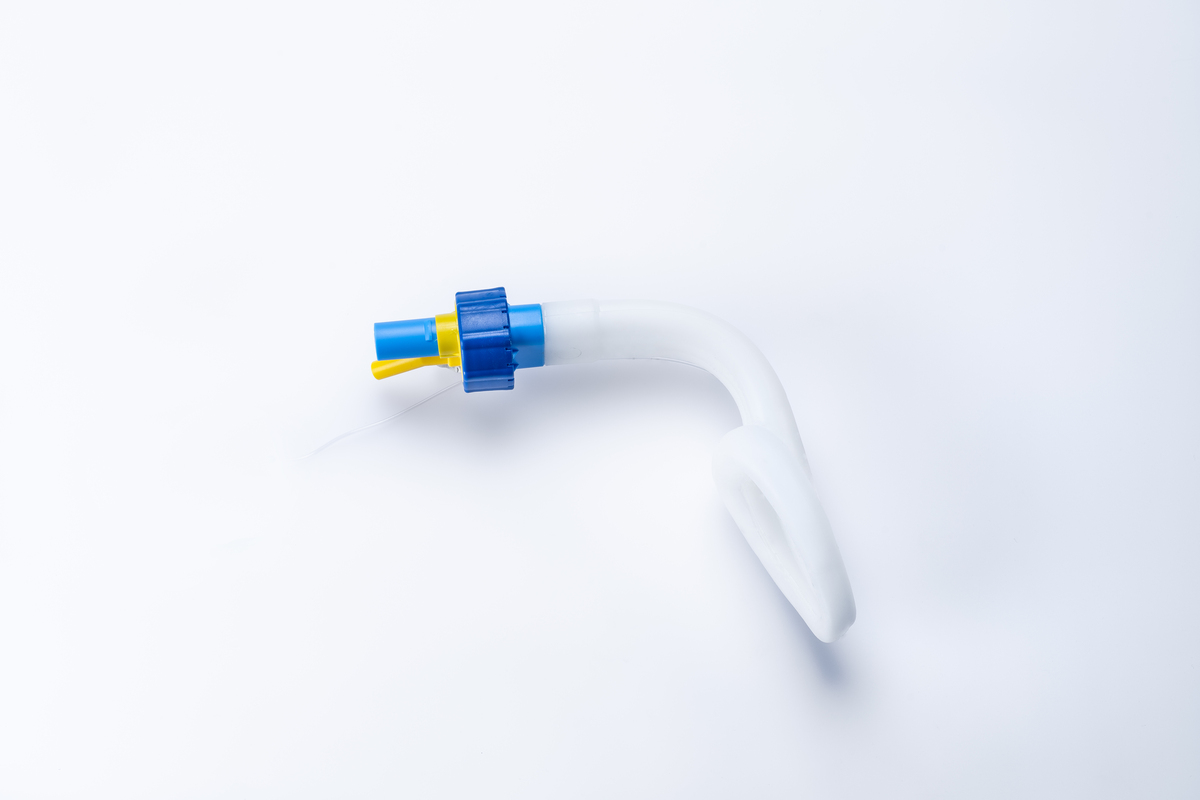
A wide variety of SGAs and LMs is now available. The recently introduced Singularity Air secondgeneration LM (Singularity AG, Maur/Zurich, Switzerland; Figure 1) features an adjustable shaft angle, controlled by a dial, allowing the device to be bent after insertion. This flexibility is hypothesized to improve sealing of the LM airway. To date, evaluations of the Singularity Air have been carried out primarily in controlled laboratory settings involving trained personnel, or as observational, non-controlled studies [11, 12].
This study’s aim was to compare the in-vitro performance of the Singularity Air LM with two established devices: (a) the first-generation LM Unique (LMA, Teleflex, Athlone, Ireland), inserted by inexperienced users, and (b) the well-studied secondgeneration LM Ambu AuraGain (Ambu, Bad Nauheim, Germany), inserted by trained airway management personnel. The primary endpoint was the time to successful ventilation.
METHODS
Setting and participants
This randomized, controlled comparative study was conducted from January to March 2025 at a Swiss acute care hospital performing approximately 9,000 anesthetics annually. The local Ethics Committee of Eastern Switzerland determined that the study was exempt from formal approval (EKOS 24/028, 22.02.2024). No formal sample size calculation was conducted, as the study was exploratory and aimed to provide initial performance data under standardized conditions. Figure 2 shows the CONSORT flow diagram for the study design.

Study Part A included 20 medical personnel without anesthesia training and with no prior experience in LM insertion (physicians and nurses from the emergency department or intensive care unit). Study Part B included 20 anesthesia staff trained in airway management and experienced in LM insertion (> 50 applications in patients). All participants were volunteers responding to a volunteer recruitment request circulated through the hospital’s internal communication channels.
Study devices and intervention
Using a pre-generated list of randomized numbers, participants were allocated to one type of LM according to their study part. Participants in Study Part A were assigned to either the Singularity Air or the first-generation Unique LM. In Study Part B, participants were assigned to the Singularity Air or the second-generation AuraGain LM. All devices were size 4.
Prior to beginning insertion attempts, participants in Study Part A individually viewed an approximately 5-minute instructional video on LM insertion, which had been selected by the investigators from publicly available online materials. Participants could ask questions after watching the video. Each participant performed five consecutive insertions with the same device. Prior to each insertion, bagmask ventilation was performed. LM insertion was carried out independently by the participant, without assistance from a second person (e.g., for mouth opening or the Esmarch maneuver). If the insertion was unsuccessful, participants were allowed to modify the insertion technique, such as 180° rotation, increased bending in Singularity Air shaft, or digital guidance with a finger. After successful LM insertion, the cuff was inflated using a hand-operated cuff manometer (Cuff manometer; VBM, Sulz am Neckar, Germany) to a pressure of 60 cmH2O, and bag–LM ventilation was initiated.
Before use, the cuffs of all LMs were nearly deflated using a syringe, and both the inner and outer surfaces were lubricated with silicon spray (Silikospray; Rüsch, Kernen, Germany). The shaft of the Singularity Air was slightly bent and the cuff prepared according to the manufacturer’s instructions. The LMs were replaced after every five participants. All attempts at airway management were performed on a Laerdal Airway Trainer torso (Laerdal Medical, Stavanger, Norway).
Variables and measurements
LM insertion was defined as successful if bagLM ventilation produced visible chest movement of the mannequin within 60 seconds. The study’s primary endpoint was the time from cessation of bagmask ventilation to the first successful manual ventilation through the LM. One of two investigators (D.N., A.D.) observed each set of five attempts and measured the time using a stopwatch. After each set of five attempts, participants rated the difficulty of the task on a scale from 0 (very easy) to 10 (extremely complex and difficult).
Statistical methods
Normality of continuous variables was assessed using the Shapiro-Wilk test. Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate. Cate gorical data are reported as frequencies and percentages. For non-normally distributed data, the Mann-Whitney U-test was performed. P < 0.05 was considered statistically significant. All analyses were conducted in Stata (version 15; StataCorp, College Station, TX).
RESULTS
Study Part A – Medical personnel without anesthesia training
The overall success rate for LM insertion was 100% (n = 100; five attempts by 20 participants) for both masks. During the first attempt, the median time to successful ventilation was 13.5 seconds (IQR 11–16) for the LM Unique and 17 seconds (IQR 10–22) for the Singularity Air (P = 0.5959). These times decreased to 8 seconds (IQR 6–9) for the LM Unique (P = 0.0049), and 7.5 seconds (IQR 5–10) for the Singularity Air (P = 0.005). The inter-device comparison at the fifth attempt was not significantly different (P = 0.7073). Participants rated the median level of difficulty of insertion as 2 (IQR 1–3) for both the LM Unique and the Singularity Air (P = 0.5882).
Study Part B – Anesthesia staff trained in airway management
The success rate for LM insertion was 99% (n = 100; five attempts by 20 participants). One attempt with the Singularity Air was unsuccessful due to a leakage in the mannequin lung model, so that successful ventilation could not be confirmed. At the first attempt, the median time to successful ventilation was 13 seconds (IQR 11–17) for the LM AuraGain and 12 seconds (IQR 10–14) for the Singularity Air (P = 0.4859). These times decreased to 8 seconds (IQR 7–9) for the LM AuraGain (P = 0.005) and 7.5 seconds (6–8) for the Singularity Air (P = 0.009). The intermask comparison at the fifth attempt showed no significant difference (P = 0.2437). Participants rated the median difficulty of insertion as 0 (IQR 0–1) for the LM AuraGain and 1 (IQR 0–2) for the Singularity Air (P = 0.3712).
Singularity air
When comparing Study Parts A and B for the Singularity Air only, the success rate for LM insertion was 99% (n = 100). As mentioned above, one attempt in the anesthesiology trained group failed due to a problem with the mannequin. The median time to successful ventilation for the first attempt was 17 seconds (IQR 10–22) in the non-anesthesia trained group and 12 seconds (IQR 10–14) seconds for the anesthesiology trained group (P = 0.2870). By the fifth attempt, these times decreased to 7.5 (IQR 5–10) seconds and 7.5 (IQR 6–8) seconds, respectively (P = 0.6740). There was no statistically significant difference in the perceived difficulty of insertion (median 2 [IQR 1–3] for the non-anesthesiology group versus 1 [IQR 0–2] for the anesthesia-trained group; P = 0.2770).
However, the non-anesthesiology participants demonstrated a greater improvement across the five attempts, with a median reduction of 9 seconds compared with 5 seconds in the anesthesia-trained group (P = 0.1518). This 4-second greater improvement indicates a steeper learning curve among participants without prior airway management training.
DISCUSSION
In this randomized in-vitro study, the performance of the Singularity Air LM was compared between medical personnel with and without airway management training. Both groups achieved high overall success rates and comparable times to successful ventilation, indicating that the device can be effectively used even by operators without prior anesthesia experience. While no statistically significant differences were observed in insertion time or perceived difficulty between the groups, participants without airway management training showed a greater reduction in time to successful ventilation across repeated attempts.
LM airways are probably the most widely used SGAs. Because they are less invasive and easier to teach, LMs serve not only as an alternative to endotracheal intubation in elective general anesthesia but also as a potentially life-saving backup device in difficult airway situations [1, 2]. They are particularly valuable for personnel with limited experience in airway management, such as paramedics or military medical staff [1, 13].
Second-generation LMs allow for the insertion of gastric probes and may also facilitate tracheal intubation through the device. The Singularity Air is a second-generation LM that was recently introduced but has not yet been widely evaluated. In a randomized crossover mannequin study (Laerdal Airway Management Trainer; Laerdal Medical, Stavanger, Norway), Gasteiger et al. [11] compared insertion times for the Singularity Air to the Ambu AuraGain when used by anesthetists experienced in more than 100 SGA insertions. They found a mean insertion time of 24 seconds for the Singularity Air as compared to 20 seconds for the Ambu AuraGain (P < 0.001), both longer than in our study. Furthermore, their overall insertion rate (92%) for the Singularity Air was lower than ours. The reasons for these discrepancies remain unclear but may relate to differences in study design such as repeated interventions in our study, creating a learning effect. Furthermore, their definition of insertion time may differ from ours, and their masks were lubricated with gel only on the back surface, whereas in our study both the outer and inner surfaces were lubricated with silicone spray, possibly facilitating insertion. In addition, differences in mannequin type and airway geometry could have influenced the results.
Our insertion time data for the AuraGain are simi lar to those reported by Wong et al. [14] in actual patients (11 ± 3 seconds) but shorter than those described by Kriege et al. [15] (30 seconds [18–41]) and Svendsen et al. [16] (54 ± 26 seconds). In general, insertion times and success rates tend to be more favorable in mannequins than in patients, as mannequins lack physiological responses and anatomical variability [9]. This difference likely explains why LMAs can be inserted within seconds in static models but often require 20 seconds or more in clinical settings. The Singularity Air is relatively rigid due to the mechanism to bend its shaft after having been inserted. This rigidity, combined with the lubrication on both surfaces, may aid insertion once the optimal angle is identified.
Insertion of LMs by untrained personnel is mainly promoted for emergency situations such as cardiopulmonary resuscitation or military medicine, where it offers a practical alternative to tracheal intubation and bag mask ventilation [1, 13]. Several simulation studies have shown that novice users can achieve performance comparable to trained personnel, likely reflecting the relative simplicity of the insertion procedure [5, 10, 17]. In clinical practice, however, the task involves more complexity, including sufficient anesthesia depth and ventilation adjustments. First-generation LMs may be easier to insert, which was the reason we chose to use two different comparator devices. In our study, the non-anesthesia trained participants showed a greater improvement between the first and fifth insertion attempts (9 vs. 5 seconds, P = 0.1518), suggesting a steeper learning curve among less experienced operators. This difference did not reach statistical significance, possibly due to the limited sample size.
One strength of this randomized, controlled comparison involving both anesthesia-trained and non-trained medical personnel is that it enabled assessment of the influence of operator experience on the performance of a new second-generation LM. The standardized in-vitro design ensured that all participants performed under identical, reproducible conditions, while repeated insertions provided insight into the learning effect and handling characteristics of the Singularity Air.
However, several limitations should be acknowledged. The in-vitro setting cannot fully replicate the anatomical variability, airway secretions, or stress conditions encountered in clinical practice. The use of a mannequin therefore limits the generalizability of the findings to real-world airway management. Additionally, the sample size was relatively small, and performance was assessed over only five insertions, which may underestimate or overestimate the learning effect with continued practice. Furthermore, lubrication of the inner and outer surfaces of the LM may have simplified insertion compared with clinical conditions. Finally, participants were aware that they were being observed, which may have influenced their performance.
CONCLUSIONS
In this exploratory mannequin study, the Singularity Air LM achieved a high success rate and comparable time to ventilation between acute care medical personnel with and without airway management training. These preliminary findings suggest that prior airway experience may have only a minor influence on device performance under standardized conditions.