
Due to advanced age and numerous comorbidities, neck of femur (NOF) fracture is a common, incapacitating injury among older adults and is frequently linked to significant morbidity and mortality [1]. Because insufficient analgesia can result in delirium, longer hospital stays, and a delayed recovery, effective pain management and optimal patient satisfaction are essential elements of perioperative management in patients with fractured NOFs [2].
Since spinal anesthesia (SA) has a better hemodynamic profile and fewer pulmonary complications than general anesthesia, it is commonly used for the surgical repair of the NOF [3]. The positioning of patients for the administration of SA is frequently complicated by preoperative pain. This could make it less effective and make patients uncomfortable [4].
Numerous prespinal analgesic techniques have been developed to improve SA efficacy and ease patient positioning [5]. Although it mainly affects the anterior aspect of the thigh and knee, the femoral nerve block (FNB) has long been considered an effective method of providing analgesia for femoral fractures [6].
By focusing on the articular branches innervating the anterior hip capsule, the pericapsular nerve group (PENG) block has recently become a viable alternative for treating hip fracture pain [7].
Additionally, because they are convenient and readily available in the perioperative setting, simple pharmacological measures such as preoperative intravenous (IV) fentanyl administration are still widely used, even though they might not offer the same degree of analgesic efficacy and patient satisfaction as nerve blocks [8].
There is a relative lack of comparative data focusing on their effects on patient satisfaction and SA ease in NOF surgery, despite the benefits of each approach being reported. We predicted that, in comparison to IV fentanyl, the PENG block would result in better SA quality and patient satisfaction.
This study’s main goal was to evaluate the effectiveness of prespinal analgesic techniques – the FNB, PENG block, and IV fentanyl – in facilitating the performance of SA for procedures involving fractured NOF. It focused on pain reduction during positioning, ease of spinal administration, and immediate procedural outcomes, such as patient positioning comfort, time to readiness for surgery, and technical ease of SA placement. Opioid usage and postoperative analgesia were regarded as secondary outcomes.
MATERIAL AND METHODS
In this prospective, randomized, double-blind study, 210 patients of both sexes who were 60 years of age or older were chosen to concentrate on elderly patients who were most affected by NOF fracture and were most likely to benefit from the intervention. These patients had physical statuses cate gorized as II or III by the American Society of Anesthesiology, and they were undergoing internal fixation of NOF with SA. This study was approved by the ethical committee of Aswan University Hospitals (IRB: Aswu 918/5/24), and written informed consent was obtained from all subjects participating in the trial. Clinicaltrials.gov registered the trial before any patients were enrolled (ID: NCT06537323). The study was carried out between July 2024 and January 2025.
Individuals who were known to be allergic to the study drug were excluded from participation. All participants underwent laboratory testing and clinical examination and their medical history was taken before the surgery. They were also taught how to accurately report their pain levels by using the visual analog scale (VAS) to measure pain.
Blinding and randomization
Computer-generated codes (https://www.randomizer.org/) were used in a randomized allocation procedure to guarantee the study’s integrity, and each participant’s code was kept blind by keeping it in opaque, sealed envelopes. A 1 : 1 : 1 randomization process was used to divide the participants into three groups.
Group A received 20 mL of 0.25% bupivacaine along with ultrasound-guided FNB.
Group B was administered the same volume and concentration of bupivacaine through ultrasound-guided PENG. Given its proven ability to provide sufficient analgesia for femoral and PENG blocks while reducing the risk of motor blockade and systemic toxicity, 20 mL of 0.25% bupivacaine was selected for nerve blocks [6, 7].
Group C: 10 to 15 minutes before SA, they received 1 µg kg–1 IV fentanyl. Because of its quick onset and brief duration, 1 µg kg–1 IV fentanyl was chosen as the dose that would be most effective for preoperative analgesia. The literature provides strong support for this dosage as an effective way to manage pain in older patients while lowering the risk of sedation and respiratory depression.
To preserve allocation concealment, identical occlusive dressings were placed either over the block site (Groups A and B) or the IV cannula site (Group C) to ensure a similar appearance. The study was observer-blinded: patients in the control group did not receive a sham block, but the anesthesiologists performing SA and all outcome assessors remained unaware of group allocation. Two separate teams performed the prespinal analgesic techniques and SA, while data analysts were also blinded to group assignments to minimize bias and maintain study validity.
Under ultrasound guidance (ACUSON NX3, Siemens, Germany), both PENG and FNB were given 10–15 minutes before SA, which was carried out with patients seated, using a 25G Quincke needle and 2.5 mL of 0.5% hyperbaric bupivacaine at the L3–L4 or L4–L5 interspace. Before the drug injection, the flow of cerebrospinal fluid (CSF) was verified. Following SA, patients were immediately placed in a supine position.
Femoral nerve block
The femoral vessels were visualized by placing a high-frequency transducer (6–12 MHz) transversely at the inguinal crease. In relation to the femoral nerve, the femoral artery and vein were situated medially at the level of the inguinal ligament. If more than one artery was found, such as the superficial and deep femoral arteries, the probe was positioned closer until only the common femoral artery and its associated vein were visible. In most cases, the femoral nerve was visible as an oval or bright (hyperechoic) wedge that was directly lateral to the femoral vessels. The femoral nerve was located next to the iliopsoas muscle group, superficially, and below the fascia lata and fascia iliaca. Before the block needle (SonoPlex, STIM 20G, Germany) was inserted into the tissue, a lidocaine wheal was applied. The needle tip was then advanced toward the femoral nerve beneath the fascia iliaca. An in-plane or out-of-plane technique was used, depending on the clinician’s preference. To make sure the needle was outside of a blood vessel and avoid intravascular injection, negative aspiration for blood was carried out. The local anesthetic’s spread around the nerve was verified using ultrasound guidance. Extremely high injection pressures or nerve enlargement, which might have suggested an intraneural injection, were avoided [9].
Pericapsular nerve group (PENG)
Above the anterior inferior iliac spine (AIIS), a low-frequency (2–5 MHz) curvilinear transducer was positioned horizontally. To locate the femoral artery, ilio-pubic eminence, and pubic ramus, the probe was lowered. After that, the probe was turned approximately 45o either clockwise or counterclockwise to align with the pubic ramus. A 20G, 10 cm long, echogenic needle (SonoPlex, STIM 20G, Germany) was inserted laterally to medially within the musculofascial plane between the pubic ramus and the psoas tendon using the in-plane technique. The distribution of the anesthetics under the iliopsoas muscle confirmed the precise needle position.
Senior anesthesiologists with more than three years of experience and more than fifty blocks of each type administered all regional blocks.
Data collection and outcome measures
The Ease of Spinal Anesthesia (EOSA) Score [10] is a tool used to evaluate the difficulty of SA administration. It combines objective data with subjective ratings from the anesthesiologist conducting the procedure. The EOSA Score is a 5to 25-point system used to evaluate the difficulty of administering SA, although there have been few specific validation studies for it. Higher scores suggest a more difficult process, while lower scores indicate a simpler one. Patient positioning, the palpability of anatomical landmarks, the number of attempts at needle passes, the degree of needle redirection, and the time until CSF appearance are the five main factors that determine the score. A structured me thod for assessing and forecasting possible difficulties in SA is provided by the rating system, which rates each parameter from 1 (easiest) to 5 (most difficult). An easy procedure is indicated by a total score of 5 to 10, a moderately difficult procedure by a score of 11 to 15, a difficult procedure by a score of 16 to 20, and a very high difficulty or failure by a score of 21 to 25.
Before the administration of SA, at 10, 20, 30, 60, 90, and 120 minutes, and at the end of the procedure, hemodynamic parameters, such as heart rate (HR) and mean arterial blood pressure (MAP), were measured.
At baseline, during patient positioning, immediately after SA puncture, 6, 12, and 24 hours after surgery, and 30 days later, VAS scores were evaluated. It was determined how much nalbuphine was used overall in the first 24 hours. 0.1 mg kg–1 of nalbuphine was given if the VAS score was higher than 4. From the conclusion of surgery to the first request for more pain relief, the time to first rescue analgesia was calculated.
Hypotension, nausea, vomiting, respiratory depression, pruritus, urinary retention, motor weakness, systemic toxicity from local anesthetics, and block-related side effects were among the many complications that were carefully recorded. 10 mg of ephedrine was used to treat hypotension, which was defined as a drop in MAP of more than 20% from baseline or MAP < 65 mmHg. Ondansetron was administered intravenously at a dose of 0.1 mg kg–1 to treat postoperative nausea and vomiting (PONV). Additional issues were noted, including respiratory depression, pruritus, urinary retention, motor weakness, and any adverse effects related to the block.
The days from surgery to discharge were used to calculate the length of hospital stay. The 30-day post-surgery readmission and mortality rates were also tracked.
Within 24 hours and 30 days after surgery, patient satisfaction was assessed using a 5-point Likert scale, with 1 denoting extreme dissatisfaction, 2 unhappiness, 3 neutrality, 4 satisfaction, and 5 extreme satisfaction [11].
Time to the first request for analgesia, nalbuphine consumption within the first 24 hours, postoperative pain scores, intraoperative hemodynamic stability, duration of the spinal block, patient satisfaction, the incidence of complications, time to surgical readiness, and length of hospital stay were the study’s secondary outcomes. The research’s primary outcome was the EOSA score.
Sample size calculation
The sample size was determined using G*Power version 3.1.9.2 from the University of Kiel, Germany. A preliminary pilot study involving 10 participants in each group revealed that the mean (± SD) EOSA scores were 8.2 ± 0.78 for Group A, 8.7 ± 0.82 for Group B, and 8.1 ± 1.1 for Group C. Based on an effect size of 0.291, a 95% confidence level, 95% study power, an equal group ratio of 1 : 1 : 1, and adding 8 participants per group to account for potential dropouts, the total sample size was calculated. Consequently, 70 patients were recruited for each group.
Statistical analysis
All statistical analyses were conducted using SPSS software, version 27 (IBM Corp., Armonk, NY, USA). Data normality was evaluated using the ShapiroWilks test and visualized with histograms. For normal quantitative variables, results were expressed as means ± standard deviations and analyzed using ANOVA followed by Tukey’s post hoc test. Quantitative non-normal data were presented as medians and interquartile ranges and examined with the Kruskal-Wallis test and Bonferroni post hoc tests. Qualitative variables were reported as frequencies and percentages and analyzed using the χ2 test. Additionally, the method of repeated measures ANOVA was used to assess differences between groups over time.
RESULTS
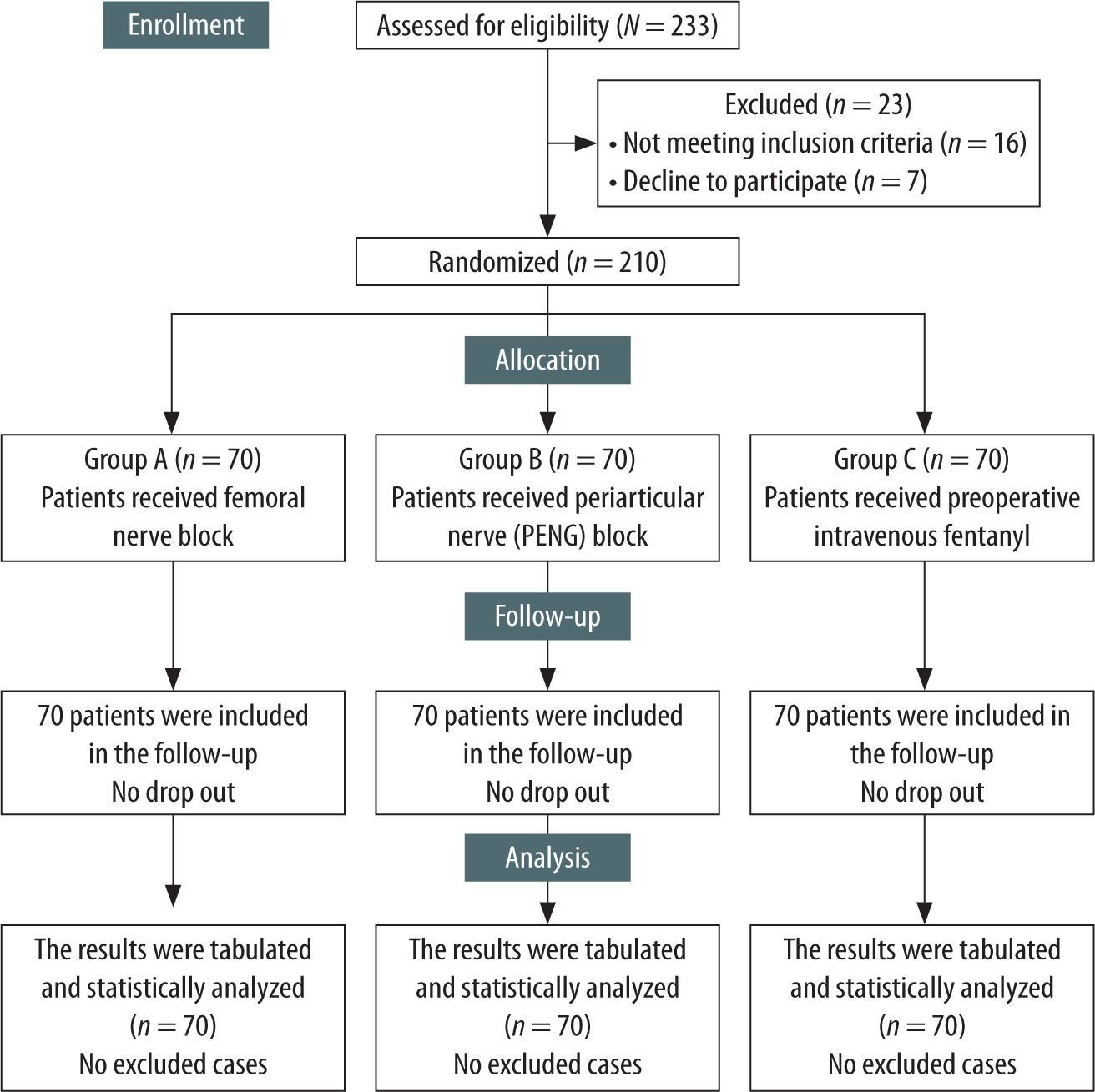
A total of 233 patients had their eligibility evaluated (Figure 1). 210 patients were randomly assigned to one of three groups: FNB (Group A), PENG (Group B), or IV fentanyl (Group C) after 23 patients were eliminated (16 did not meet inclusion criteria, and 7 chose not to participate).
Age, sex, weight, height, body mass index (BMI), ASA physical status, and length of surgery were comparable across the three groups (Table 1).
TABLE 1
Demographic data and duration of surgery of the studied groups
The PENG group had the lowest median EOSA score, at 7 (IQR 7–8), while the FNB group had 8 (IQR 7–9) and the IV fentanyl group had 9 (IQR 9–10) (P < 0.001). Significant differences between all groups were validated by post hoc Bonferroni-adjusted pairwise comparisons (Table 2).
TABLE 2
Ease of Spinal Anesthesia (EOSA) score, time of first rescue analgesia (h), total nalbuphine consumption (mg), visual analog scale (VAS)
At several perioperative timepoints, VAS scores were evaluated. The three groups’ VAS scores were similar at the time of block administration (P = 0.076). The PENG group had significantly lower VAS scores during patient positioning for SA than both the FNB and IV fentanyl groups (P < 0.001), while the fentanyl group had the highest pain scores and the FNB group had intermediate scores. Likewise, patients in the PENG group reported the lowest pain at the time of spinal puncture, followed by those in the FNB group, while the fentanyl group reported the most pain (P < 0.001).
At 6 and 12 hours after surgery, the PENG group still had the lowest VAS scores, followed by the FNB group with intermediate scores and the fentanyl group with the highest pain scores (P < 0.001 for both time points). Nonetheless, there were no significant differences in the groups’ VAS scores at 24 and 30 days after surgery (P = 0.134 and P = 0.22, respectively). The absolute difference (~0.5 minutes) in readiness time was statistically significant (P = 0.046), but it was probably not clinically significant.
The PENG group had the longest time to first rescue analgesia (8.8 ± 2.03 hours, 95% CI: 8.3–9.3), which was significantly longer than the IV fentanyl group (4.2 ± 0.7 hours, 95% CI: 4.0–4.4) and the FNB group (5.9 ± 1.5 hours, 95% CI: 5.5–6.4) (P < 0.001). According to pairwise comparisons, the mean difference between PENG and fentanyl (95% CI: 3.98–5.19) and FNB (95% CI: 2.3–3.5) was 2.91 hours.
In the first 24 hours, the PENG group needed the least amount of nalbuphine (10.3 ± 4.01 mg), while the FNB group (13.8 ± 4.63 mg) and the IV fentanyl group (18.4 ± 5.51 mg) needed the most (P < 0.001). The average consumption difference was –7.01 mg (PENG vs. fentanyl; 95% CI: –8.87 to –5.16) and –3.5 mg (PENG vs. FNB; 95% CI: –5.38 to –1.63).
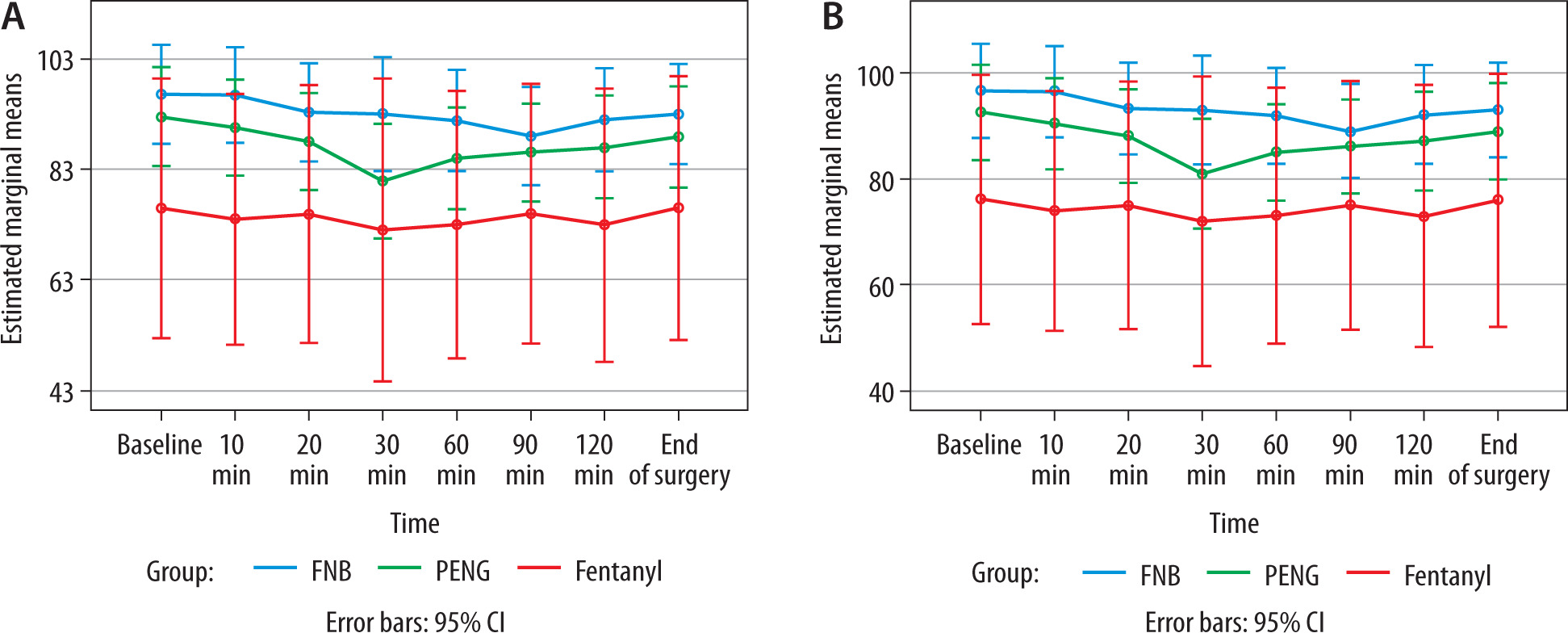
Over time, the groups’ MAP and HR were largely similar. At various intraoperative timepoints, however, the IV fentanyl group showed statistically significantly lower MAP and HR values (Figure 2).
There was no significant difference in the incidence of bradycardia, hypotension, postoperative nausea and vomiting (PONV), or other documented complications between the groups (Table 3).
TABLE 3
Complications, readmission, mortality, and patient satisfaction of the studied groups
There were no reports of pruritus, respiratory depression, motor weakness, systemic toxicity from local anesthetics, hematomas, or infections.
The duration of hospitalization was comparable for the FNB, PENG, and fentanyl groups, at 4.96 ± 1.48 days, 4.51 ± 1.32 days, and 4.90 ± 1.72 days, respectively (P = 0.176).
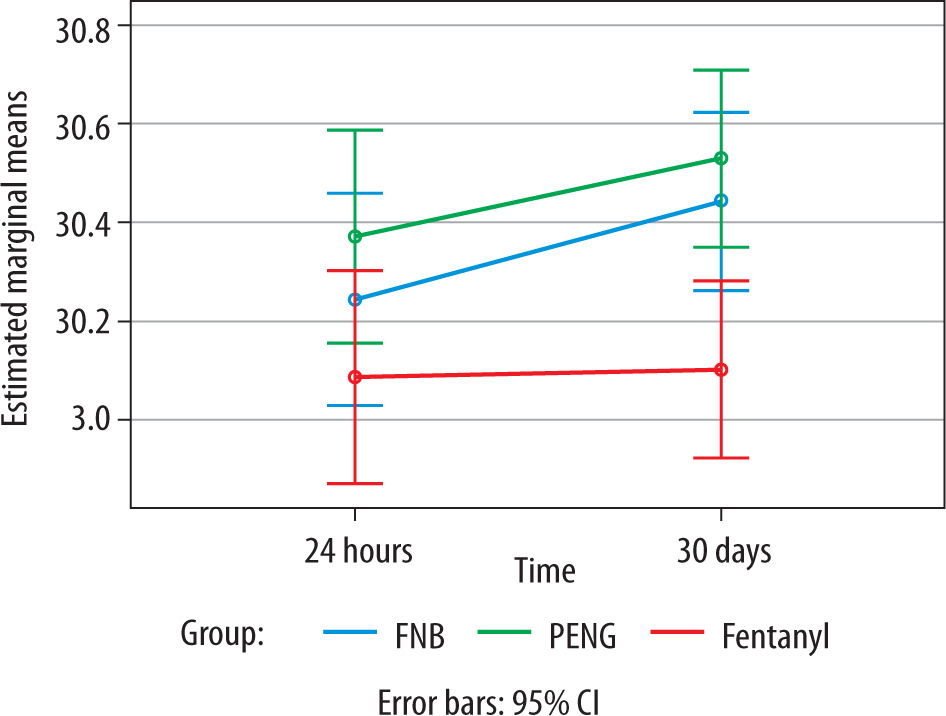
At 24 hours after surgery, the PENG group’s satisfaction scores were marginally higher than those of the FNB and fentanyl groups, although the differences were not statistically significant (P = 0.212). While there was no statistically significant difference between the PENG and FNB groups at 30 days, the PENG group’s satisfaction scores were significantly higher than those of the fentanyl group (P = 0.002) (Figure 3).
DISCUSSION
NOF fracture patients frequently have excruciating preoperative pain that makes it difficult to position them correctly for SA. An increased number of needle passes, agitation, and trouble aligning anatomical landmarks can result from such pain. These factors not only prolong the procedure but also increase the risk of complications and unsuccessful SA. Consequently, reducing pain during patient positioning is essential for increasing overall patient comfort as well as procedural ease [12, 13].
Certain nerves implicated in hip pain are targeted by regional analgesic techniques. IV fentanyl provides systemic pain relief, whereas FNB and PENG block are intended to provide localized analgesia. The EOSA scores were significantly lower for both FNB and PENG blocks than for IV fentanyl in our study, suggesting simpler patient positioning and less procedural difficulty. The PENG block in particular produced the lowest EOSA scores, most likely as a result of its targeted blockade of the articular branches innervating the anterior hip capsule. This directly lowers positioning pain and facilitates a smoother spinal puncture [3, 7].
Our results, which demonstrate that the PENG block facilitates SA more effectively than FNB and IV fentanyl, are consistent with earlier research. When compared to alternative analgesic techniques, Alshawadfy et al. [14] found that the PENG block greatly decreased positioning pain and enhanced procedural ease. The benefit of this technique was further supported by Alrefaey and Abouelela’s findings that patients undergoing the PENG block had fewer needle redirections and a shorter time to CSF appearance [15]. Our findings were further supported by a comparative trial conducted by Lin et al. [16], which showed lower EOSA scores with the PENG block.
We measured VAS scores in addition to EOSA scores at various intervals during the administration of the block, during patient positioning, and immediately after SA. Our findings showed that although the groups’ VAS scores were comparable at the block stage, there were notable variations in positioning and the way SA was administered. Interestingly, during the spinal procedure and positioning, the PENG group reported the lowest VAS scores. Lower intra-procedural pain is associated with an easier spinal technique, as evidenced by the strong correlation between this pain reduction and the observed lower EOSA scores. The significance of targeted regional blocks over systemic opioids in promoting procedural success is highlighted by these dynamic pain assessments [17, 18].
Although facilitating SA was our main goal, the PENG block also showed advantages in secondary outcomes. When compared to patients receiving FNB or IV fentanyl, patients in the PENG group had a longer time to first rescue analgesia, lower cumulative opioid consumption, and lower pain scores at 6 and 12 hours postoperatively. These findings support the view that good prespinal analgesia improves early postoperative pain management in addition to the technical aspects of SA. Long-term satisfaction and pain scores at 24 and 30 days, however, were comparable across groups, indicating that the advantages of these methods are greatest during the first few days following surgery [15, 18].
In spite of its efficacy, the PENG block’s patient satisfaction ratings at 24 and 30 days after surgery were similar to those of the FNB. Individual pain thresholds, perioperative anxiety, and surgical technique variations may be the reason for the lack of significant differences between PENG and FNB, even though both regional techniques showed superior long-term satisfaction compared to IV fenta nyl. Furthermore, our findings support those of Jadon et al. [17], who reported that FNB, compared with IV fentanyl, enhances patient comfort and satisfaction during SA positioning.
In contrast to our findings, Abd El-Rahman et al. [18] found that PENG and FNB were equally effective in postoperative pain management. The disparities could be the result of different study procedures, such as different local anesthetic concentrations, nerve block methods, or control group opioid dosages. Though they used a higher IV fentanyl dose (2 µg kg–1), Musallam et al. [19] did not include PENG block in their comparison of IV fentanyl and FNB, which may have contributed to their failure to find any discernible differences between the two.
PENG blocks’ effectiveness in this study raises the possibility of their wider use in other procedures that call for efficient perioperative analgesia, such as total hip replacements, pelvic fracture repairs, or lower limb operations. Multimodal analgesia strategies that aim to improve recovery and minimize complications are well aligned with the technique’s anatomical specificity and capacity to decrease opioid consumption. However, greater access to ultrasound guidance and anesthesiologist training might be necessary for widespread adoption.
LIMITATIONS
EOSA is not a widely standardized score, but it was developed based on prior literature assessing procedural difficulty, positioning, and patient cooperation patient positioning. However, its reliability and generalizability require further validation in larger, multicenter trials to establish its role as a standardized tool. Between-group satisfaction needs a larger sample size to become significant. This study’s single-center design limits the generalizability of findings to other settings with diverse patient populations or resources. Potential selection bias may have arisen from the exclusion of patients with significant comorbidities. Additionally, the short follow-up period restricts the assessment of long-term outcomes, such as chronic pain management and functional recovery.
CONCLUSIONS
For patients with a fractured femoral neck, the PENG block proved to be more effective than the FNB and IV fentanyl in promoting SA. The PENG block has a clear clinical advantage by lowering positioning pain considerably, making the procedure easier, and improving early postoperative analgesia with few side effects. These results confirm that the PENG block is a preferred prespinal analgesic technique that may be considered a preferred option used in hip fracture surgery to maximize anesthesia quality, enhance recovery pathways, and improve patient outcomes. To confirm its wider applicability across a variety of surgical populations, more multicenter trials are necessary.