
The PREVENT-MINS trial was a multicenter randomized controlled study, designed to determine whether perioperative heart-rate reduction with ivabradine could prevent myocardial injury after non-cardiac surgery (MINS) in high-risk adults [1]. In this trial, more than 2,100 patients aged ≥ 45 years undergoing major noncardiac procedures were randomized to receive ivabradine or placebo, with MINS as a primary endpoint, adjudicated using high- sensitivity troponin assays [2]. In intention to treat analysis, ivabradine resulted in a modest perioperative decrease in heart rate, however, it did not reduce the incidence of MINS or major cardiovascular complications at 30 days [3]. PREVENT-MINS trial findings highlight the substantial and persistent burden of MINS and point to the need for improved strategies to identify patients at risk – particularly through the use of cardiac biomarkers.
Preoperative N-terminal pro-B-type natriuretic peptide (NT-proBNP) is a strong predictor of peri-operative cardiovascular events, showing a clear stepwise relationship with 30-day vascular outcomes in the VISION cohort [4]. Its inclusion improves risk discrimination beyond the Revised Cardiac Risk Index (RCRI) [5, 6], and major guidelines now recommend routine preoperative NT-proBNP (or BNP) testing in at-risk patients [7]. NT-proBNP has thus become a central element of perioperative risk stratification [8, 9].
Despite strong evidence supporting prognostic value at baseline [10], the clinical significance of postoperative significance of postoperative changes in NT-proBNP remains poorly understood. Unlike troponin-defined MINS, natriuretic peptide dynamics around the time of surgery have been studied only sparingly, and their independent contribution to short-term outcomes remains unclear. Moreover, whether targeted hemodynamic interventions – such as heart-rate reduction with ivabradine can influence these postoperative trajectories is unknown.
The aim of the present study was to perform a per-protocol analysis of the PREVENT-MINS trial and to determine whether ivabradine affects postoperative NT-proBNP concentrations in high-risk patients undergoing major noncardiac surgery.
METHODS
Overview of the PREVENT-MINS parent trial
The PREVENT-MINS trial (NCT05279651) was an investigator-initiated, randomized, placebo-controlled superiority study conducted across 26 hospitals in Poland [11]. Its primary objective was to determine whether perioperative ivabradine, compared with placebo, reduced the incidence of MINS. The full study design and protocol have been published previously [1]. All participating centers obtained approval from local institutional review boards and bioethics committees, and all participants provided written informed consent in accordance with national regulations and the Declaration of Helsinki.
Patient selection and recruitment
Full eligibility criteria are presented in the original protocol. In brief, participants were eligible if they were ≥ 45 years old, scheduled for noncardiac surgery requiring at least one postoperative overnight stay, and at elevated cardiovascular risk. Elevated risk was defined by a history of coronary artery disease, peripheral arterial disease, or stroke; planned major vascular surgery; or the presence of at least three predefined clinical risk factors. Key exclusion criteria included cardiac conduction abnormalities, ivabradine use within the previous month, and hemodynamic parameters that precluded study drug administration.
Screening occurred in preoperative clinics or upon hospital admission. Trained study personnel confirmed eligibility, obtained informed consent, and collected baseline demographic, clinical, and medication data. Following the second pre-specified interim analysis, the independent Data Monitoring Committee recommended early termination of the trial for futility.
Randomization and blinding
Randomization was performed after eligibility verification. Participants were assigned to treatment groups via an interactive web-based system employing random permuted blocks, with stratification by center. Participants, treating clinicians, trial personnel, and outcome adjudicators remained blinded to treatment allocation. Emergency unblinding was permitted solely for safety reasons.
Trial intervention
Eligible participants received oral ivabradine 5 mg or a matching placebo at least one hour before surgery. A second 5-mg dose was administered ≥ 12 hours later if hemodynamic criteria continued to be met. From postoperative day 1 through day 7 (or until discharge, whichever occurred first), the study drug was administered twice daily.
Data collection and follow-up
During hospitalization, study personnel prospectively recorded vital signs, perioperative management details, study medication administration, and laboratory results, including high-sensitivity troponin and NT-proBNP measurements. Clinical outcomes were determined by review of medical records and standardized follow-up at 30 days and 1 year after surgery, conducted in person or by telephone according to trial procedures. Case report forms were submitted via dedicated electronic data-capture software (BioStat).
Methods for the PREVENT-MINS NT-proBNP substudy
Study design
This study is a post-hoc, per-protocol secondary analysis evaluating perioperative NT-proBNP changes within the PREVENT-MINS trial. No procedures beyond those defined in the parent study protocol were implemented.
Substudy population
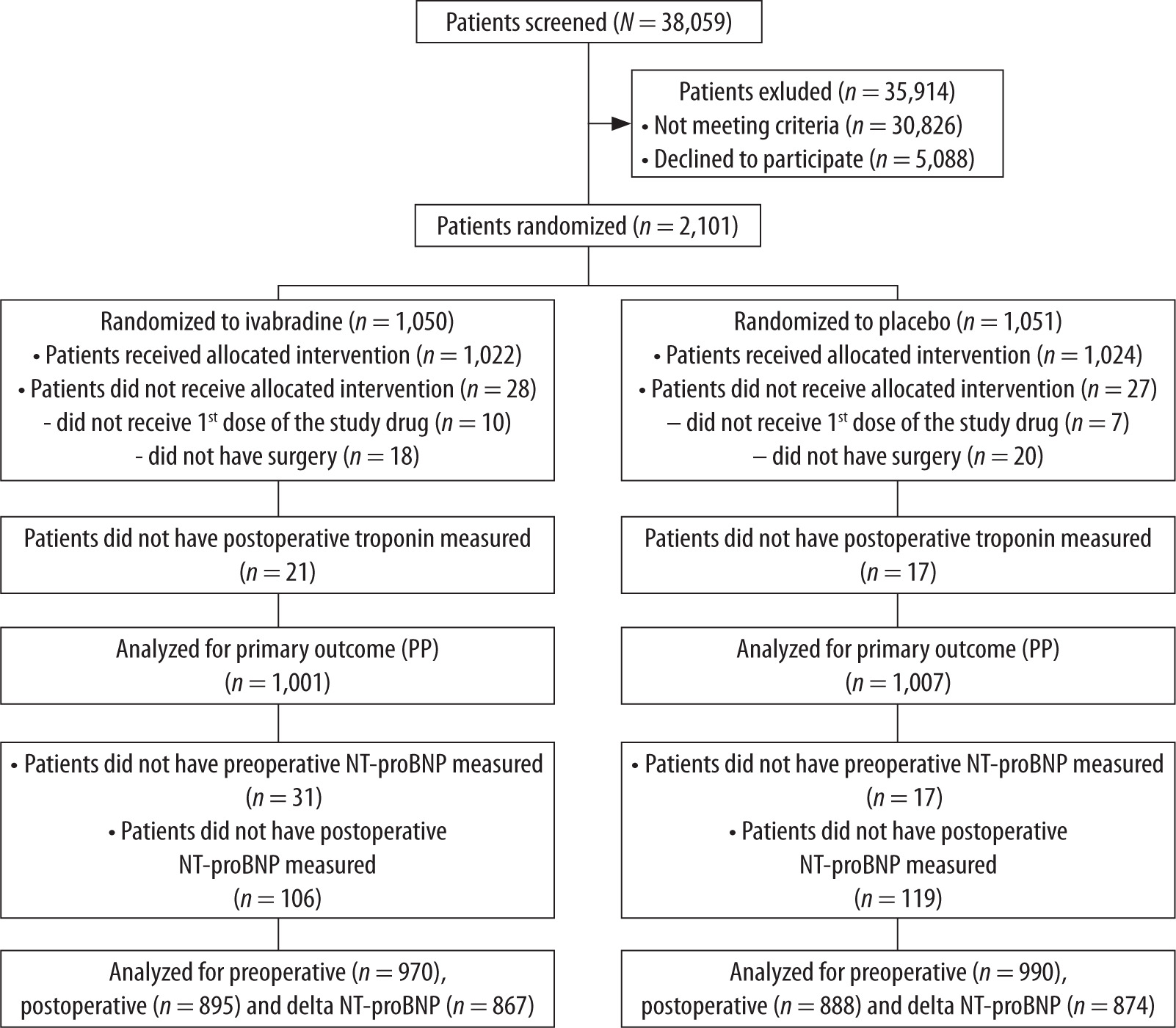
The substudy included all PREVENT-MINS participants who met per-protocol criteria. Patients were eligible if they: 1) were randomized in the PREVENT-MINS trial; 2) received at least one dose of the assigned study drug; 3) underwent the index noncardiac surgery; and 4) had both preoperative and postoperative high-sensitivity cardiac troponin measurements. Of the 2,101 randomized participants, 2,008 met these criteria and were included in the per-protocol cohort (1,001 assigned to ivabradine and 1,007 to placebo), as depicted in the study flow diagram (Figure 1).
Biochemical measurements
Preoperative NT-proBNP concentrations were measured within 24 hours before surgery using hospital assays calibrated according to manufacturer specifications. Local laboratories applied assay-specific reference ranges and standard quality-control procedures. Protocolised postoperative NT-proBNP measurements were obtained on the second postoperative day (approximately 48 hours after surgery) using the same assay platforms. In patients with more than one postoperative measurement, the peak postoperative NT-proBNP value was used for the analyses. Delta NT-proBNP was defined as the difference between peak postoperative and preoperative NT-proBNP values.
Preoperative NT-proBNP measurements were missing for 31 patients in the ivabradine group and 17 in the placebo group, and postoperative NT-proBNP values were unavailable for 106 and 119 patients, respectively. These patients were excluded from the NT-proBNP analyses accordingly and delta NT-proBNP was calculated exclusively for participants with both pre- and postoperative NT-proBNP measurements.
High-sensitivity cardiac troponin was measured preoperatively and on postoperative days 1–3 according to the PREVENT-MINS protocol.
Substudy outcomes
The main substudy outcome was postoperative NT-proBNP and delta NT-proBNP in the per-protocol cohort, analyzed according to randomized treatment assignment. Additional outcomes, evaluated in the per-protocol population, included the primary endpoint of the parent trial (MINS occurring intraoperatively or within 30 days), key secondary outcomes, and safety endpoints.
To assess robustness with respect to baseline differences in coronary artery disease (CAD) in the NT-pro-BNP analysis, a post hoc exploratory sensitivity analysis was performed after excluding patients with documented CAD. Definitions of MINS and myocardial infarction followed those of the main PREVENT-MINS trial, relying on standardized high-sensitivity troponin thresholds and adjudication of non-ischemic causes.
Statistical analysis
No separate sample-size calculation was performed for this analysis; all eligible per-protocol participants from PREVENT-MINS were included. Analyses were conducted in the per-protocol population while preserving randomized treatment allocation. Continuous variables are reported as medians with interquartile ranges, and categorical variables as counts and percentages. Between-group comparisons employed the Mann-Whitney test for continuous variables and the χ2 test for categorical variables.
Continuous secondary outcomes (including days alive and at home, health-related quality-of-life scores, intraoperative mean arterial pressure, intra-operative heart rate) were analyzed in the per-protocol cohort using linear regression, generating mean differences with corresponding 95% confidence intervals (95% CI).
We performed an analysis of covariance (ANCOVA) to evaluate the association between ivabradine treatment and peak NT-proBNP levels. Because NTproBNP often exhibits a right-skewed distribution, both baseline and peak NT-proBNP values were naturally logarithmically- transformed prior to analysis [12]. The ANCOVA model included log-transformed peak postoperative NT-proBNP as the dependent variable, ivabradine use as the main factor, and log-transformed preoperative NT-proBNP as a covariate. Additional covariates were age, sex, body mass index (BMI), history of congestive heart failure, history of coronary artery disease, and an interaction term, if an interaction between covariates was detected. Assumptions of homogeneity of variances were tested using Levene’s test. Estimated marginal means and Bonferroni-adjusted pairwise comparisons were used to quantify adjusted group differences. Residual normality was assessed using the Shapiro-Wilk test. Finally, marginal means of log-peak postoperative NT-proBNP for the ivabradine and placebo groups were back-transformed and percentage difference between groups was calculated.
All P-values are two-sided, with a P-value of less than 0.05 considered to indicate statistical significance. MedCalc Statistical Software (MedCalc Software Ltd, Ostend, Belgium).
RESULTS
Per protocol results
Among the 2,101 patients included in the intention-to-treat analysis, 2,008 (95.6%) adhered to the study protocol and were included in the per-protocol analysis. Among these, 1,001 received ivabradine and 1,007 received placebo (Figure 1).
Baseline demographic characteristics, type of noncardiac surgeries and anesthesia, and preoperative medications were well balanced between the groups (Table 1). Noticable distinctions were observed in the history of CAD which was more common in ivabradine group [268 (26.8%) vs. 223 (22.1%) patients; P = 0.016] and history of hypertension, which was less common in the ivabradine group [911 (91%) vs. 941 (93.4%) patients; P = 0.04].
The primary outcome, MINS occurred in 177 of 1,001 patients (17.7%) receiving ivabradine and in 158 of 1,007 patients (15.7%) receiving placebo (RR, 1.13; 95% CI: 0.93–1.37; P = 0.23). Among patients with MINS, 7 out of 177 in the ivabradine group and 9 out of 158 in the placebo group fulfilled the criteria for myocardial infarction (Table 2).
NT-pro-BNP results
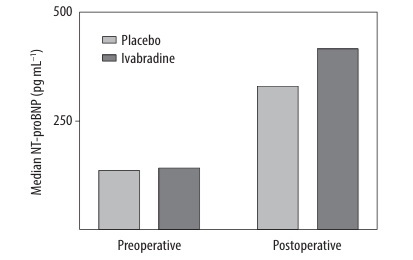
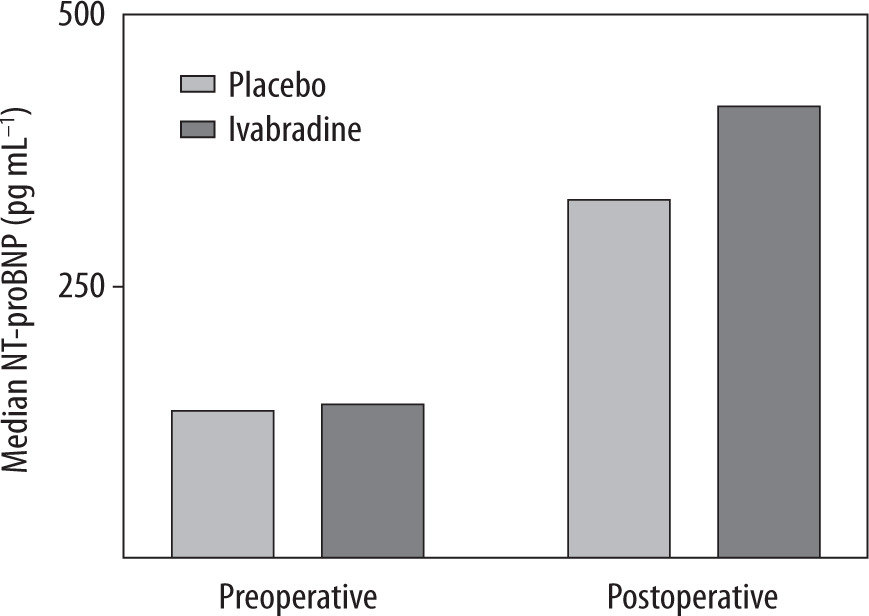
The overall preoperative NT-pro-BNP value was 139.6 pg mL–1 (IQR, 68.0 to 267.0) with no differences between ivabradine and placebo group. Patients who received ivabradine had significantly higher median postoperative NT-pro-BNP (418.0 vs. 333.5 pg mL–1; P < 0.001; Figure 2) and higher median delta NT-proBNP (215.1 vs. 154.0 pg mL–1; P < 0.001) than patients who received placebo (Table 3).
TABLE 1
Baseline characteristics, type of surgery, anesthesia, and perioperative medications (per-protocol)
[i] *Meeting this eligibility criterion involved meeting at least three of the nine risk criteria listed here.
†Major surgery was defined as undergoing intraperitoneal, intrathoracic, retroperitoneal, or major orthopaedic procedure.
‡Values represent the median pool troponin concentration across all assays.
ACEI – angiotensin-converting enzyme inhibitors, ARB – angiotensin receptor blockers, BMI – body mass index, IQR – interquartile range
TABLE 2
Effects of Ivabradine on the primary, secondary and safety outcomes at 30 days (per-protocol)
[i] *PMI defined by the 2022 European Society of Cardiology (ESC) guidelines on cardiovascular assessment and management of patients undergoing non-cardiac surgery.
†Health-related quality of life calculated as an index of EuroQoL 5-Dimension tool.
‡Presented as the mean difference (95% CI).
MINS – myocardial injury after noncardiac surgery
FIGURE 2
Median plasma N-terminal pro-B-type natriuretic peptide (NT-proBNP) concentrations (pg mL–1) in patients receiving ivabradine or placebo. Measurements were obtained preoperatively and postoperatively
In the ANCOVA analysis ivabradine treatment had a significant independent effect (F = 10.1, P = 0.002), with adjusted marginal means indicating higher log-transformed peak postoperative NTpro-BNP values in the ivabradine group (6.25 ± 0.09 vs. 5.65 ± 0.09; P = 0.0015). The adjusted mean difference on the log scale (Δ = 0.59 ± 0.19) corresponds to an approximate 82% increase in NT-proBNP among patients receiving ivabradine (95% CI: ~26–164).
A sensitivity analysis was performed after excluding 491 patients with known CAD. In this analysis, patients receiving ivabradine continued to show higher delta NT-proBNP compared with those receiving placebo (213.0 pg mL–1 [IQR, 52.6–495.0] vs. 148.0 pg mL–1 [IQR, 33.08–408.9]; P < 0.001).
DISCUSSION
In this per-protocol analysis, ivabradine did not reduce the incidence of MINS compared with placebo in patients undergoing noncardiac surgery. The direction and magnitude of the primary, secondary, and safety outcomes were consistent with those observed in the recently reported ITT analysis [2]. Notably, randomization to ivabradine was associated with greater postoperative NT-proBNP release.
Overall, the PREVENT-MINS trial demonstrated high protocol adherence, with only 4.5% of patients (n = 93) deviating from the study protocol. Most exclusions from the per-protocol population involved patients who received the study drug but ultimately did not undergo surgery (n = 38, largely due to logistical reasons) or who lacked postoperative troponin measurements (n = 38, generally due to random operational factors). Consequently, the per-protocol approach did not meaningfully alter the ITT findings.
TABLE 3
Effects of ivabradine on cardiac biomarkers (per-protocol)
TABLE 4
Analysis of covariance (ANCOVA) – adjusted effects of ivabradine for log-peak postoperative NT-proBNP
[i] F-values were calculated as the ratio of the mean square for each effect to the residual mean square. The ANCOVA model included treatment (ivabradine = 1; placebo = 0), five covariates, and a treatment × log (preoperative NT-proBNP) interaction term to account for effect modification and to satisfy the assumption of homogeneity of regression slopes. The residual represents unexplained variance after adjustment for all model predictors. Homogeneity of variances was confirmed using Levene’s test (P = 0.5).
BMI – body mass index, df – degrees of freedom, NT-proBNP – N-terminal pro-B-type natriuretic peptide
Patients receiving ivabradine showed a greater postoperative increase in NT-proBNP levels compared with placebo. This effect was consistent across both univariate and adjusted models that accounted for established determinants of NT-proBNP variability. This indicates that ivabradine use is an independent factor associated with increased perioperative NT-proBNP release (82% relative increase in peak postoperative NT-proBNP). Additionally, sensitivity analyses showed that this effect was not due to differences in CAD between groups, as the increase in delta NT-proBNP remained significant even after excluding patients with CAD.
Surgery represents an acute physiological stressor, triggering adaptive responses that maintain homeostasis, including heart rate – mediated augmentation of cardiac output when metabolic demand rises. Hypothetically, ivabradine’s negative chronotropic activity may limit the heart’s ability to increase output in response to such stress. One could therefore argue that ivabradine may impair normal perioperative cardiovascular adaptation, potentially resulting in insufficient heart rate responses to intra-operative stressors such as hypotension. In the present study, patients allocated to ivabradine indeed exhibited higher rates of bradycardia requiring intervention and a trend toward more episodes of hypo-tension necessitating vasopressor support.
A blunted chronotropic response could also alter the duration of diastolic and systolic phases and disrupt ventricular filling dynamics, thereby imposing additional myocardial stress and promoting NT-proBNP release. Similar observations were reported by Davis et al. [13], who examined short-term b-blocker effects on NT-proBNP levels in patients with stable heart failure. Nevertheless, these proposed mechanisms remain speculative. In fact, most studies conducted in nonoperative populations suggest the opposite effect, demonstrating that ivabradine is associated with reductions in NT-proBNP levels [14–16]. It is therefore plausible that ivabradine administered in the perioperative setting does not confer the same biomarker-related benefits observed outside the surgical context.
This multicenter study benefits from a large and diverse surgical patient population and was conducted according to rigorous randomized controlled trial methodology with high protocol adherence. The main limitation is the incomplete availability of perioperative NT-proBNP measurements; complete paired samples (pre- and postoperative) were obtained in 82.8% of enrolled patients.
CONCLUSIONS
In the per-protocol analysis of the PREVENT-MINS trial, ivabradine did not reduce the incidence of MINS compared with placebo, consistent with the previously reported intention-to-treat results. Among patients assigned to ivabradine, greater postoperative NT-proBNP release was observed, suggesting a potential effect of the study drug on cardiac stress markers despite its lack of impact on MINS incidence.