
Compartment syndrome (CS) occurs when there is an increase in pressure within a confined space, which affects the function of the organs within it [1]. The underlying pathophysiology of all forms of CS involves a decrease in blood flow to the intra-compartmental organs due to the increase in interstitial pressure that exceeds the capillary pressure, leading to vascular collapse, tissue hypoxia and ischemia, which clinically manifests as multiorgan dysfunction [2, 3].
Thoracic compartment syndrome (TCS) can develop in a wide variety of surgical pathologies, especially in cardiac surgery, chest trauma, and common medical conditions in intensive care, which leads to increased morbidity and mortality in critically ill patients [1]. Despite this, no clear definition is available, which limits its diagnosis and timely treatment.
This study reviews the existing scientific literature on the clinical presentation, pathophysiology, and causes of TCS to propose a definition and facilitate future research.
METHODS
This study was approved by the Ethics Committee of Fundación Clínica Shaio, Bogotá, Colombia (DIB code DIB 24-15) and was exempt from informed consent requirements, as no confidential patient or institutional information was involved.
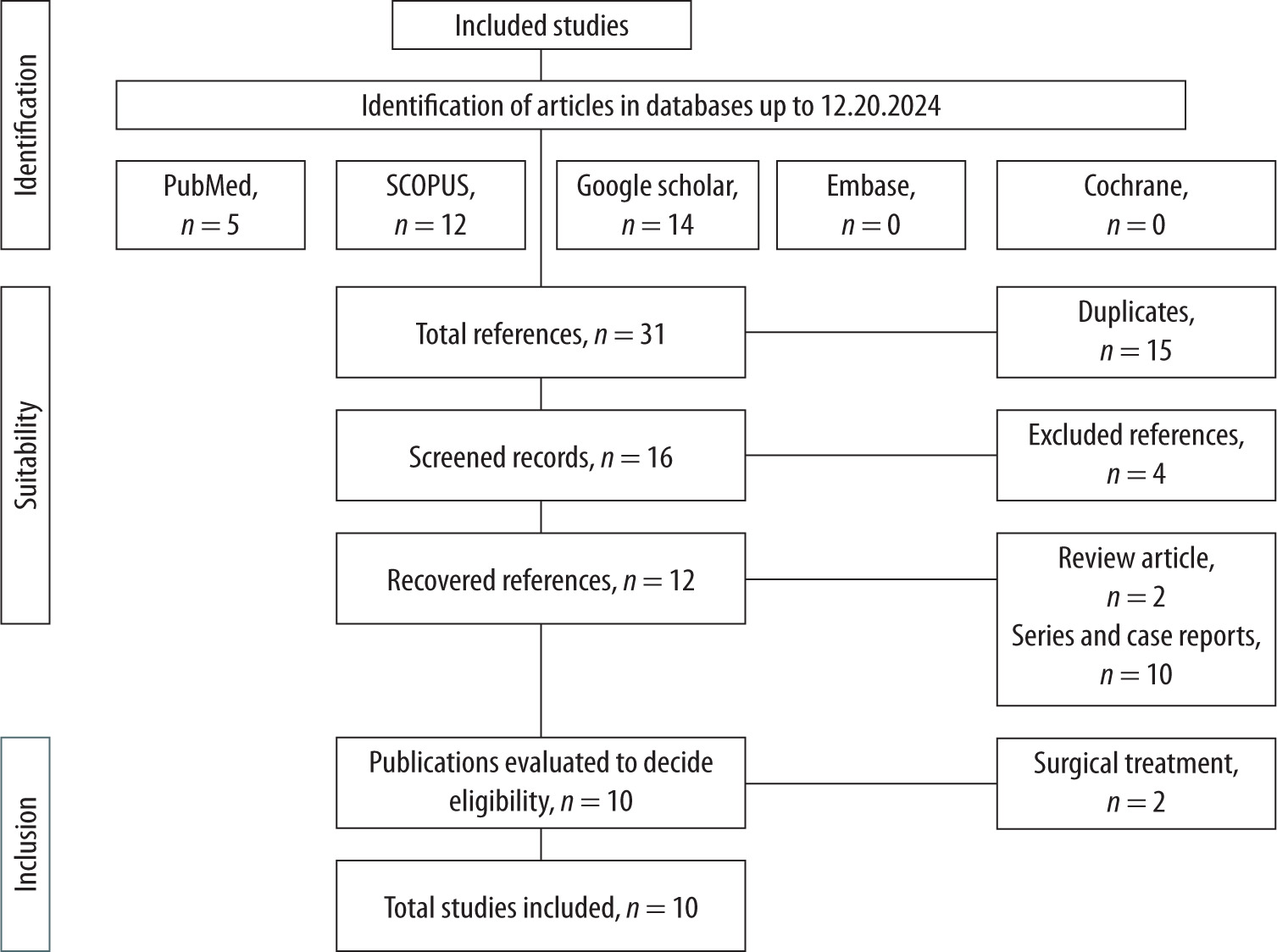
The review was carried out in several stages. In the first stage, two independent collaborators made the selection to avoid selection bias during the search for all studies, according to titles and abstracts matching our keywords and full texts. Adult patients were included without limitations on language, year of study, or publication. All studies in pregnant patients or the pediatric population were excluded. The identification of studies and literature reviews was done through a bibliographic search in the databases PubMed, Scopus, Embase, Google Scholar, and SpringerLink, in addition to a manual search of identified articles that were considered valid.
Additionally, a search was carried out in gray literature in the NTIS and EAGLE databases to increase sensitivity and ensure that all relevant information was captured. The search terms focused on three concepts using MESH and EMTREE terms when appropriate – thoracic, compartment, and syndrome – from the journal’s beginning to December 20, 2024. The second stage involved screening the identified articles, and in the third stage, articles that met the minimum inclusion and exclusion criteria for the full-text review were included (Figure 1 and Table 1).
DISCUSSION
The human body is commonly described in the literature as having four compartments: head, thorax, abdomen, and extremities [1]. The perfusion pressure (PP) of an organ depends on the inflow pressure (mean arterial pressure – MAP) and the outflow pressure (venous pressure – VP):
PP = MAP – VP [4]
In turn, the pressure of the cavity in which these organs are contained is inversely related to their perfusion pressure, due to the collapse of the venous drainage system by the drop in transmural pressure, which leads to a decrease in blood flow corresponding to each organ, as in the case of intracranial perfusion pressure (IPP).
IPP = MAP – ICP [4]
PP assessment should be evaluated objectively in each of the compartments. In the thoracic compartment, there is a surrogate for intrathoracic pressure (ITP) measured through an esophageal pressure catheter (Pes); however, the availability of this is low in most intensive care units around the world, for which a surrogate in patients with invasive mechanical ventilation is the peak inspiratory pressure (PIP) measured by the ventilator, considering that this could be affected by other pathologies such as increased airway resistance [1, 5].
TCS was initially described in 1975 by Riahi et al. [6] in postoperative (POP) patients undergoing cardiac procedures with prolonged intraoperative time. These patients present pathophysiological alterations during the procedure, such as myocar-dial edema, pulmonary edema, acute ventricular dilation, and premature sternal closure, which increases the risk of developing cardiac tamponade in the POP period [1]. Subsequently, it was described in non-surgical populations such as closed chest trauma with primary space-occupying lesions (hemothorax, pneumothorax, and hemopericardium) [7].
Finally, in recent decades, it has been described in other medical conditions in intensive care, such as acute respiratory distress syndrome [1].
Causes of TCS
They are classified as primary due to injuries or conditions that compromise the intrathoracic organs or secondary due to increased pressure in one cavity being transmitted from an adjacent one (Table 2) [1, 2, 8].
TABLE 1
Selection of studies and proposed definitions
Impact on physiology and fluid dynamics
The thorax is a semi-rigid cavity surrounded by the rib cage and delimited by the thoracic inlet (superior thoracic aperture) and the diaphragm at the lower part. Inside are three compartments separated by fibrous tissue: 2 pulmonary cavities delimited by the pleura and the mediastinum, which contains all other structures within the thorax. The transverse thoracic plane at the T4 vertebral level further divides the mediastinum into a superior and inferior compartment. The superior mediastinum contains the great vessels, and the inferior mediastinum comprises the space between the transverse thoracic plane and the diaphragm [9].
The inferior mediastinum is divided into anterior, middle, and posterior portions [9]. The heart, contained within the pericardium, is in the middle mediastinum. The outer layer of the pericardium – the parietal pericardium – is attached to the walls of the great vessels and the diaphragm [10]. The inner layer is the visceral pericardium, which is in direct contact with the heart. Between these two layers is a space with a small amount of lubricating fluid that reduces the friction generated by cardiac movement [9], maintaining a pressure between 0 and 5 mmHg. When this pressure exceeds the intracardiac pressure, it can cause a collapse of the cardiac chambers [11]. All these layers of fibrous tissue that contain the intrathoracic organs communicate with each other, creating continuity between all the structures that make up the thorax and, therefore, the ability to transmit pressures from one organ or compartment to another.
The intrathoracic compartments are delimited by structures allowing pressure to be transmitted to another, impacting the adjacent organs [9–11]. In the case of a tension pneumothorax, the expansion of the pleural cavity displaces the mediastinum, causing compression of the cardiac chambers and vessels, leading to obstructive shock [12]. Therefore, the thorax behaves as a multicompartmental space in which each compartment depends on the others.
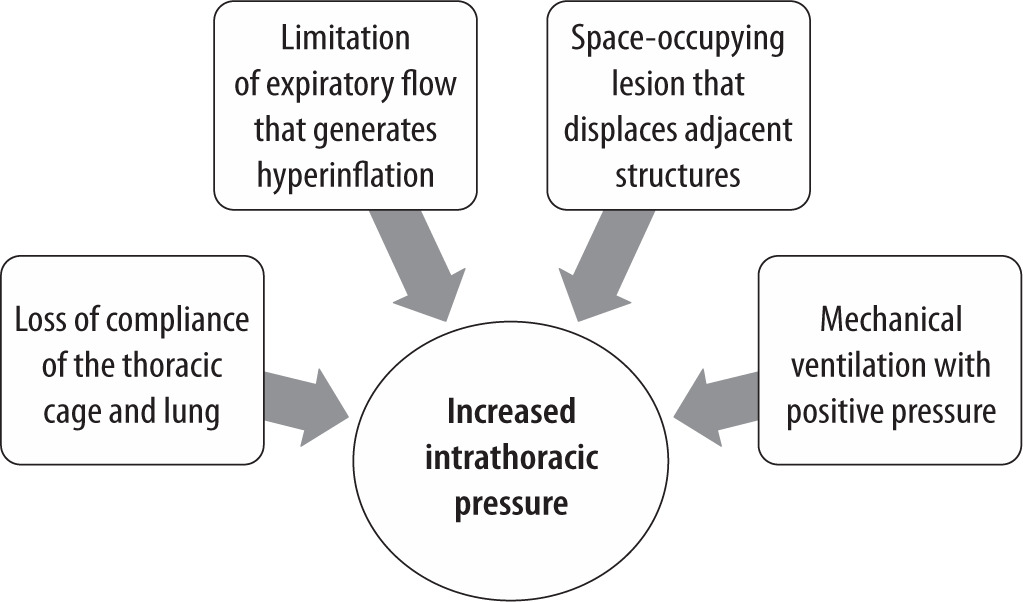
Normal ITP ranges from 5 to 7 mmHg and can be measured directly via a Pes catheter or indirectly using surrogate markers such as PIP. ITP exceeding 15 mmHg defines intrathoracic hypertension (IH), while TCS is typically associated with ITP above 25 mmHg [1, 5, 13]. However, TCS diagnosis should not rely solely on pressure thresholds but also consider the resulting organ dysfunction [1–3, 14] (Figure 2).
TABLE 2
Causes of thoracic compartment syndrome
Heart-lung interaction
Intrathoracic pressure directly affects the pre-load and afterload of the right ventricle (RV) and left ventricle (LV). Negative ITP increases venous return, decreases RV afterload, and increases LV afterload. When pleural pressure increases, this heart-lung interaction reverses, affecting normal cardiovascular function, as occurs during positive pressure ventilation. In cases of low lung compliance, the changes in intrathoracic pressure and hemodynamics are more pronounced [15, 16].
This increase in ITP is transmitted to the right atrial pressure (RAP). According to Ohm’s law, venous return (VR) depends on the pressure gradient between the mean systemic filling pressure (Pms) and RAP, while venous resistance (Rv) opposes this return.
VR = (Pms – RAP)/Rv) [17]
FIGURE 3
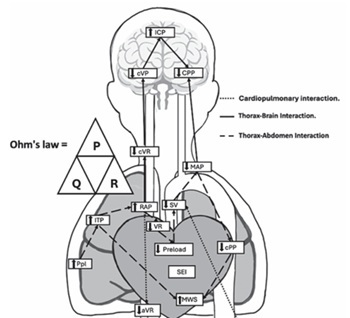
Multicompartment syndrome: the increase in ITP transmitted to the right atrium generates a decrease in venous return based on Ohm’s law; this, in turn, generates an increase in venous pressure in the abdominal and cerebral compartments, which decreases the perfusion pressure of the contained organs, leading to oxygen debt and multiorgan dysfunction [40]. The limitation to VR also decreases stroke volume, increasing hypoperfusion and hemodynamic instability
Ppl – pleural pressure, ITP – intrathoracic pressure, RAP – right atrial pressure, VR – venous return, SV – stroke volume, MAP – mean arterial pressure, CPP – coronary perfusion pressure, MWS – myocardial wall stress, SEI – subendocardial ischemia, CVR – cerebral venous return, CVP – cerebral venous pressure, ICP – intracranial pressure, CPPc – cerebral perfusion pressure, AVR – abdominal venous return, AVP – abdominal venous pressure, IAP – intra-abdominal pressure, PP – perfusion pressure, ACS – abdominal compartment syndrome, DeOX – oxygen debt
An increase in RAP will lead to a reduction in VR, which results in a decrease in stroke volume and cardiac output (CO) of the LV [1]. This pressure is also transmitted to the rest of the cardiac chambers, which increases myocardial wall stress [18]. Additionally, the increase in ITP causes airway compression, increasing respiratory system resistance with an increase in PIP, plateau pressure, and mean airway pressure, and a decrease in respiratory system compliance.
The decrease in CO due to the mechanisms described leads to metabolic acidosis and hemo-dynamic instability, with a drop in systemic arterial pressure combined with an increase in LV end-diastolic pressure, resulting in a decrease in coronary perfusion pressure, inducing subendocardial ischemia, which worsens the hemodynamic state [18].
Increased ITP, as the pericardium and sternum limit ventricular diastolic function, generates a limitation in LV filling. Accordingly, prolonged open sternotomy has been proposed as an alternative in cases of cardiac surgery in patients with other risk factors or comorbidities that facilitate TCS [2, 19].
Additionally, hemodynamic evaluation in patients with IH can be limited because the values of central venous pressure (CVP), right ventricular pressure, or pulmonary artery wedge pressure (PAWP) measured by the pulmonary artery catheter can be overestimated due to the alteration of the transmural pressure of the great vessels in this pathology. Some authors recommend adjusting the values, using end-expiratory filling pressures, taking into account that venous return is greater at end-expiration and considering transmural pressures. Some of the described formulas include [1]:
Transmural central venous pressure (CVPtm) = CVP – ITP [1]
Transmural pulmonary artery wedge pressure (PAWPtm) = PAWP – ITP.
Another option for performing an adequate hemodynamic assessment in cases of TCS is to use the measurement of extravascular lung water using the PiCCO catheter or non-invasive methods such as bedside ultrasound [20].
Impact on other compartments
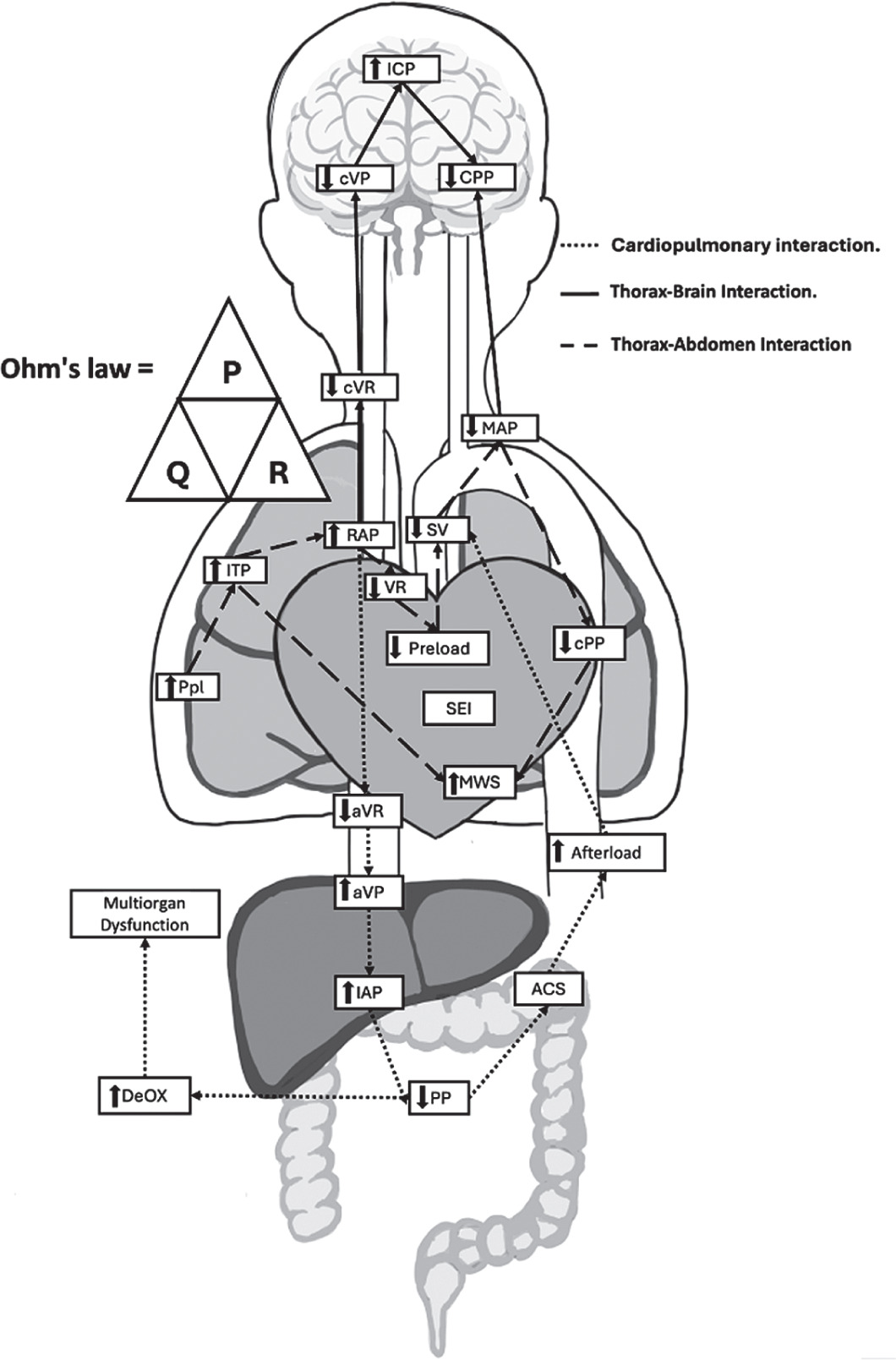
When TCS occurs, the increase in pressure does not only affect intrathoracic organs; this pressure increase is transmitted to other adjacent compartments, especially the cranium and abdomen. The increase in pressure in the cardiac chambers generates a significant limitation to VR, leading to an increase in cerebral venous pressure, resulting in intracranial hypertension, and at the abdominal level, a decrease in renal, hepatic, and intestinal tissue perfusion pressure [1, 17, 20, 21] (Figure 3).
CONCLUSIONS
TCS is a pathology that is poorly described in the scientific literature; however, it can occur in a wide range of surgical and medical conditions, in which it can worsen the clinical status and even lead to death. Despite being a potentially fatal condition, there is no clear definition to reach its diagnosis. In this article, a definition based on the evidence and the previously described pathophysiological behavior was proposed.
TABLE 3
Proposed definition of thoracic compartment syndrome
[i] *In patients with acute respiratory distress syndrome, cutoff points of peak inspiratory pressure > 35 cmH2O should be considered. **As per ASE/EACVI 2016 recommendations [28].
ITP – intrathoracic pressure, IH – intrathoracic hypertension, SBP – systolic blood pressure