
Intensive care is a goal-oriented aspect of medical practice, its objective consisting in helping the patients survive acute threats to their life while preserving and restoring its quality. The goal cannot be achieved in all patients, with the attempted medical procedures not only not bringing benefits to the patients, but also exposing them to additional suffering, thus constituting futile therapy. The first papers to open up the discussion on futile therapy were published in the English-language literature in the 1990s [1]. Futile therapy is a global problem, posing significant challenges to healthcare systems regardless of binding legislative solutions, culture, or religion. In Poland, futile therapy was defined by the Polish Working Group on End-of-Life Ethics in 2008 [2]. In 2011, guidelines for discontinuation of futile therapy in paediatric patients were published [3], followed by the 2014 guidelines of the Polish Society of Anaesthesiology and Intensive Therapy (PTAiIT; Polskie Towarzystwo Anestezjologii i Intensywnej Terapii) including a protocol for the withholding/withdrawal of futile therapy in intensive care unit settings [4], and by the 2015 ethical standards for the care of terminally ill newborns [5]. In 2021, a panel of experts in ethics, medicine, and law, appointed by the Patient’s Rights Ombudsman, published the Standards of Practice for End-of-Life Medical Therapies [6]. Proposals for legislative changes were also included in this broad-ranging study, as the current Polish legislation does not cover important issues concerning the principles for the management of end-of-life patients incapable of making decisions for themselves. The expert panel recommended the use of the protocol developed by PTAiIT as being appropriate for the procedure of withholding/withdrawing futile therapy. A year later, recommendations were published regarding discontinuation of therapy in paediatric patients treated in intensive care units [7]. The most recent Polish document extensively discussing the issues of end-of-life medical care is the position statement of the Polish Society of Internal Medicine Working Group on Medical Futility at Internal Medicine Units [8].
The purpose of this survey was to investigate the opinions on futile therapy among anaesthesiologists and residents in anaesthesiology and intensive therapy as well as to determine the frequency of the “futile therapy protocol” being used. An attempt was also made to determine the factors responsible for futile therapy still being practised in intensive care units despite the PTAiIT protocol for the procedure of withholding/withdrawing futile therapy being recommended by the expert panel appointed by the Patient’s Rights Ombudsman.
METHODS
The study was approved by the Independent Bioethics Committee of the Medical University of Gdansk (NKBBN/80/2023).
A questionnaire was developed solely for the purpose of the study. In addition to questions about demographic, professional experience, and place of work, questions regarding aspects of futile therapy in the context of medical decision-making were included in the study tool. One of the questions regarding factors that may influence the conduct of futile therapy in intensive care units made use of the wording used as codes for open-ended statements to be provided by physicians in the 2016 study by Willmot et al. [9]. In our study, the codes were used to ask how often, in the opinion of the respondent, the reasons proposed by the doctors participating in that study might be the actual reasons for the provision of futile therapy. Three external factors related to the social perception of futile therapy were included in the questionnaire. The respondents were also asked whether they thought that the COVID-19 pandemic might have influenced the perception of futile therapy. In the case of affirmative answers, a request to provide a more detailed description of any such change was included.
The reliability analysis of the test was performed using Cronbach’s alpha (a). The value of the coefficient (for questions P6_1–P6_21) was 0.903 (a > 0.9).
The survey was conducted using the computer-assisted web interview (CAWI) technique. The questionnaire was sent electronically to the intensive care units of provincial hospitals and large academic hospitals, following telephone contact. A survey with a cover letter was also uploaded on the Polish Society of Anaesthesiology and Intensive Therapy’s website and Facebook. The questionnaires were completed by respondents in an online form between May and October 2023.
Statistical analysis of the results was carried out using the IBM SPSS Statistics 25 software. The data obtained in the study were analysed by means of statistical description. The results in subgroups were compared using the c2 test, Student’s t-test, and ANOVA analysis, where appropriate. P-values < 0.05 were considered to indicate statistical significance.
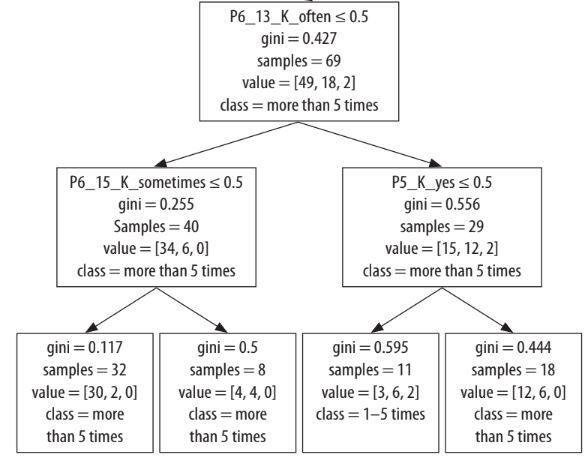
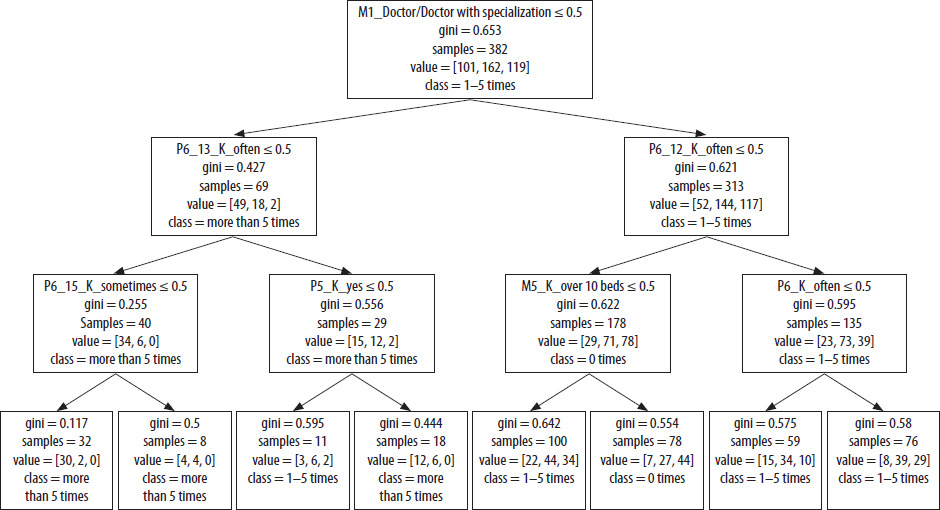
The data on the group of doctors (n = 386) who had participated in the decisions whether to abstain from or discontinue futile therapy were classified using the decision tree data-mining methodology (the Scikit-learn [sklearn] Python library). The classification threshold was assumed at the minimum of 5% of the study group (N(min)~20) on the basis of the GINI importance index, i.e. the sum of the number of classes encompassed within a particular feature in proportion to the number of classified samples (see Figure 1).
RESULTS
The study group consisted of 488 respondents including anaesthesiologists and residents in anaesthesiology and intensive therapy (265 women, 223 men). The characteristics of the study group are presented in Table 1.
TABLE 1
Characteristics of the study group (N = 488)
About 80% of the respondents (389 individuals) were anaesthesiologists, with an average ICU experience of about 15 years, while about 20%, or 99 individuals, were residents in anaesthesiology and intensive therapy, with an average work experience of 3 years. Among the anaesthesiologists, 152 had signed the futile therapy protocol 1–5 times during the last 12 months, as compared to 122 anaesthesiologists who had signed the protocol more than 5 times and 115 anaesthesiologists who had not signed the protocol even once during the past year. To the question of whether the decisions regarding the limits of intensive care should be made by physicians, a unanimous affirmative answer was provided by all anaesthesiologists. The vast majority of respondents, namely 458 individuals, were of the opinion that the decisions on intensive care limits should be subject to legal regulations.
To the question of whether medical decisions regarding the limits of intensive care should be considered by hospital ethics committees, affirmative answers were given significantly more often by doctors who had not yet participated in the work of a team deciding on the withholding/withdrawal of futile therapy, while doctors having had the experience of working in such a team (130 individuals) and those who had signed the protocol more than 5 times in the last 12 months were statistically significantly more likely to provide a negative answer.
To the question of whether the decision to with-hold/withdraw futile therapy should be based solely on medical criteria (in a manner analogous to the decision on ICU admission, which is based on medical criteria alone), an affirmative answer was provided by 76% of the general respondent group (373 individuals), with anaesthesiologists with more than 20 years of experience providing this answer significantly more frequently (93%) than anaesthesiologists with less seniority.
The results regarding the responses to questions related to factors potentially influencing the decisions on futile therapy are presented in Table 2.
TABLE 2
Responses to questions related to factors potentially influencing the decisions on futile therapy (N = 488)
The question of whether there were any other factors that could influence the decisions on futile therapy within the ICU setting was answered in an affirmative manner by 17% of respondents (82 individuals).
Half of the respondents (245 doctors) provided affirmative answers to the question of whether the COVID-19 pandemic had any impact on the perceptions of futile therapy; doctors with seniority of 11–20 years, and those who had signed the protocol more than 5 times during the past year, chose this answer significantly more often. Open-ended responses included statements suggesting that the pandemic had explicitly revealed the limitations of medical science, the inevitability of death, and the irreversibility of disease processes, shedding light on the phenomenon of patients with no good prognosis. A change in awareness among doctors of other specialties was noted as well.
Doctors who had participated in teams deciding whether to withhold or withdraw futile therapy (n = 386) had signed the protocol 1–5 times (n = 165), more than 5 times (n = 119), or 0 times (n = 102) in the past 12 months. The data were classified using the decision tree data-mining technique (the Scikit-learn [sklearn] Python library) [10].
In this way, 8 classification groups were identified, and the results were interpreted in the discussion section according to the seven factors studied. For a description of this analysis see Figure 1.
DISCUSSION
Our survey revealed that the subject of futile the rapy and its discontinuation is widely known among Polish anaesthesiologists, with most of the doctors taking part in the survey stating that they had been using the recommended protocol for the withholding/withdrawal of futile therapy with full confidence in the tool. At the same time, the ambiguous legal situation was highlighted by the respondents. It is very important to note that the frequency of decisions to withhold/withdraw futile therapy was related to the degree of doctor’s certainty regarding the number of previously signed protocols.
The results of the survey point to two key psychological aspects regarding competence of medical personnel to discontinue futile therapy. Firstly, the specialist should be convinced that their decision is right; the conviction is acquired through expertise and experience. Secondly, the specia list should also be convinced of having a personal psychological predisposition to withhold/withdraw futile therapy. The reluctance to take away the patient’s/family’s hope can be aggravating as the treatment process is frequently long and the emotional factor associated with the physician-patient relationship becomes involved. Acquisition of appropriate skills in communication and empathy in the relationship with the patient/family, as well as between the members of the medical staff, is an important factor in the process of becoming aware of one’s personal limitations and in the lifelong professional development.
There is a problem in the definition of medical futility, which cannot be unambiguous and precise, as it encompasses a plethora of techniques and treatments, most frequently invasive, each having the potential to be defined as either medically appropriate and desirable or futile depending on the condition of the patient and the stage of his/ her disease. The medical criteria for the initiation of treatment within the ICU setting are clear and widely accepted, but it is considerably difficult to objectively determine when to discontinue this therapy, who should make the relevant decision, and what criteria should be used as the basis for the decision [11]. In this aspect, the important factor of the psychological burden on doctors as regards the decision to discontinue therapy is also worth noting. The emotional consequences of having to take a particular course of action often result in a tendency for the withdrawal of futile therapy to be postponed. This frequently contributes to the development of professional burnout syndrome in the described group [12]. Some publications have raised issues of demands to discontinue therapy being made by the patient’s family – a case has been described where the parents demanded that the therapy of their child be discontinued, while the treating doctors were completely different in their assessment of the child’s chance of responding to the treatment [13]. A problem has also been described regarding the availability of therapy and the possible costs of the requested continuation of futile therapy [14]. In our study, the doctors who had already signed futile therapy protocols were significantly more likely to indicate that the request of the patient or the patient’s family was rarely a factor in the decision to pursue futile therapy as compared to doctors having no such experience.
Adequate time should be given for conversation and reflection on the decision. The whole process should be based on candid, respectful communication and holistic end-of-life care aimed at the patient’s physical, psychosocial, and spiritual needs [15]. Arbitrary paternalism can be avoided by prospectively reviewing futility in second medical opinions (consultations) and institutional ethics committees/review boards [16]. In our survey, anaesthesiologists unequivocally stated that the decision to discontinue therapy should be made by specialist physicians, with no need for authorization by institutional ethics committees/review boards. The requirement for authorization from ethics committees was more frequently suggested by physicians having had no previous experience with the futile therapy protocol. However, it seems that any contentious situations should best be resolved in a consultation-oriented manner while avoiding a paternalistic attitude.
As in other studies, the doctors participating in our study voiced their concerns regarding the legal consequences of their decisions and thus raised the question of the necessity of relevant state regulations. Declarations of will were the most popular solution proposed to address contentious cases [17, 18]. Consideration of the patient’s will and autonomy in making the decisions regarding their own treatment would, in the opinion of the authors, be a gesture of respect for the patient’s right to make decisions; meanwhile, it is very often the case that the patient has no say on what their last days of life should look like.
A key question relates to who should make the decision to withhold/withdraw futile therapeutic procedures when the patient is unconscious and cannot make the decision on their own. Studies on the decision-making by family members have shown significant discrepancies. In 2016, the Society of Critical Care Medicine Ethics Committee published a position statement and guidelines to help with the decision-making process when the patient or their family disagrees with the physicians’ position [19]. In our study, the factor of lack of information about the patient’s/the patient’s family’s wishes was significantly more frequently mentioned by residents in anaesthesiology and intensive therapy as compared to anaesthesiologists already experienced with the protocol.
It is worth noting that the factors differentiating the decision to abandon futile therapy can also be analysed by the frequency of the particular characteristics included in the study. As shown by the presented decision tree analysis, the decision to abandon futile therapy is influenced by the doctor’s specialization status, social acceptance of discontinuation of futile therapy, the doctor’s personal experience, and information about the patient’s wishes or objections. It seems obvious that the age factor as identified in the decision tree analysis is also related to the professional experience of doctors.
In the context of the discussion on futile therapy, public education is of utmost importance, in order to point out that despite the tremendous progress, medicine has its limitations, and it is impossible to achieve the initially intended goals in all patients. Unfortunately, patients and their families alike sometimes develop unrealistic expectations concerning therapy and its outcomes in terms of improvement in health and quality of life. Patients, in the context of reliance on advanced medical technologies, tend to believe that life and death are in the hands of medical science, not nature. Consequently, this leads to a wrong conclusion that the patient dies because medicine has failed, not because life is limited by death [20].
It is crucial that the decision to withhold/withdraw futile therapy is made by a competent team of doctors guided by the best interests of the patient. The decision, and the process behind it, must be explained to the family. Although difficult, it should not be avoided by adopting a wait-and-see attitude.
CONCLUSIONS
Anaesthesiologists working in intensive care units believe that decisions regarding the limits of intensive care lie within the boundaries of their professional responsibility. They also recognise the need to regulate the decision-making process as part of the legal system while not perceiving a need for their decisions to be subject to authorization by hospital ethics committees. Respondents also note the need to educate the public on the subject of end-of-life care. It is also worth noting that doctors are influenced by external factors that shape their experience as being directly related to their specialty. Thus, the question whether the current process of specialty training is capable of offsetting the factors of external influences on doctors making decisions not to pursue futile therapy remains an open one.