
Low back pain (LBP) is an overwhelming health problem, involving multiple etiology such as spinal joints, intervertebral disc, vertebral bodies and paravertebral soft tissues, which develops in 28% to 42% of individuals between 40 years and 69 years old [1]. Defined as pain persisting for more than 12 weeks, chronic LBP occurs in about 13% of adults. It is a pervasive and debilitating condition affecting a total of 60.1 million person-years living with disability globally and causing extensive medical expenditure, social burden, as well as productivity loss to families, communities and countries [2, 3]. Intervertebral disc degeneration has been reported as the leading cause of chronic LBP, which is called discogenic low back pain (DLBP) and accounts for approximately
39% of all cases [4]. It is a significant clinical condition arising from degeneration of the intervertebral disc and a common yet complex cause of chronic pain with a multifactorial pathogenesis involving processes such as mitochondrial dysfunction, accumulation of advanced glycation end products, and pyroptosis, all contributing to disc degeneration and subsequent pain [5]. Although most patients will not require surgery, lumbar interbody fusion surgery is frequently considered for patients with persistent functional disabilities and pain from progressive spinal stenosis, worsening spondylolisthesis or herniated disk and failure of conservative treatment [6, 7].
Nevertheless, pre-operative diagnostic tests identifying the causative segment of disc precisely remain elusive. Computed tomography (CT) or magnetic resonance imaging (MRI) often reveals degenerative findings of the intervertebral disc in more than one lumbar motion segments; thus, provocative discography, by reproducing the concordant pain, was needed to confirm the diagnosis [8, 9]. A procedure called lumbar disc block that blocks pain by injection with a small amount of local anesthetic has been proved to be effective as an alternative tool for the diagnosis of DLBP [9, 10]. Currently, these procedures are routinely performed under fluoroscopy (FL) or even CT with contrast [11]. Although ultrasonography (US) has been a widely recognized imaging modality for guiding administration of nerve blocks due to the clear visualization for paravertebral images, the real-time guidance for needle insertion and the repeated examinations without radiation exposure, only case reports, attracting increasing clinical attention, of lumbar disc block have been reported to date [12–14].
Therefore, our study retrospectively analyzed the usefulness of US-guided lumbar disc block for detecting the definitive culprit disc for fusion surgery. Additionally, aiming to determine whether this technique could provide noninferior predictive value for successful clinical outcomes after surgery compared to routine lumbar discography under FL guidance, and facilitate the procedure under real-time sonographic guidance to allow easier accessibility and less radiation exposure.
METHODS
Study design and participant selection
After obtaining the ethical approval from the institutional Ethics Examining Committee of Human Research (xw-ky-2025011), the case-control retrospective study was conducted in accordance with the principles of the Declaration of Helsinki.
Written informed consent was obtained from all participants. The study was reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [15].
Between January 1, 2023 and November 31, 2024, patients who were admitted to the department of pain management and underwent lumbar discography or disc block procedures for the diagnosis of DLBP for fusion surgery were reviewed through the electronic medical records (EMRs). Inclusion criteria were: (1) experiencing LBP with or without radicular pain; (2) lumbar disc degeneration in more than one segment on CT or MRI; (3) failure of medications or conservative treatment for at least 6 months; (4) aged at least 18 years. Patients undergoing lumbar surgery other than specifically lumbar fusion, and patients with previous lumbar spine surgery, high iliac crest exceeding the midpoint of the fifth lumbar pedicle based on the lateral radiography, psychiatric disorder according to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-4), pregnancy, conversion to other treatments during follow-up period, and incomplete medical data were excluded.
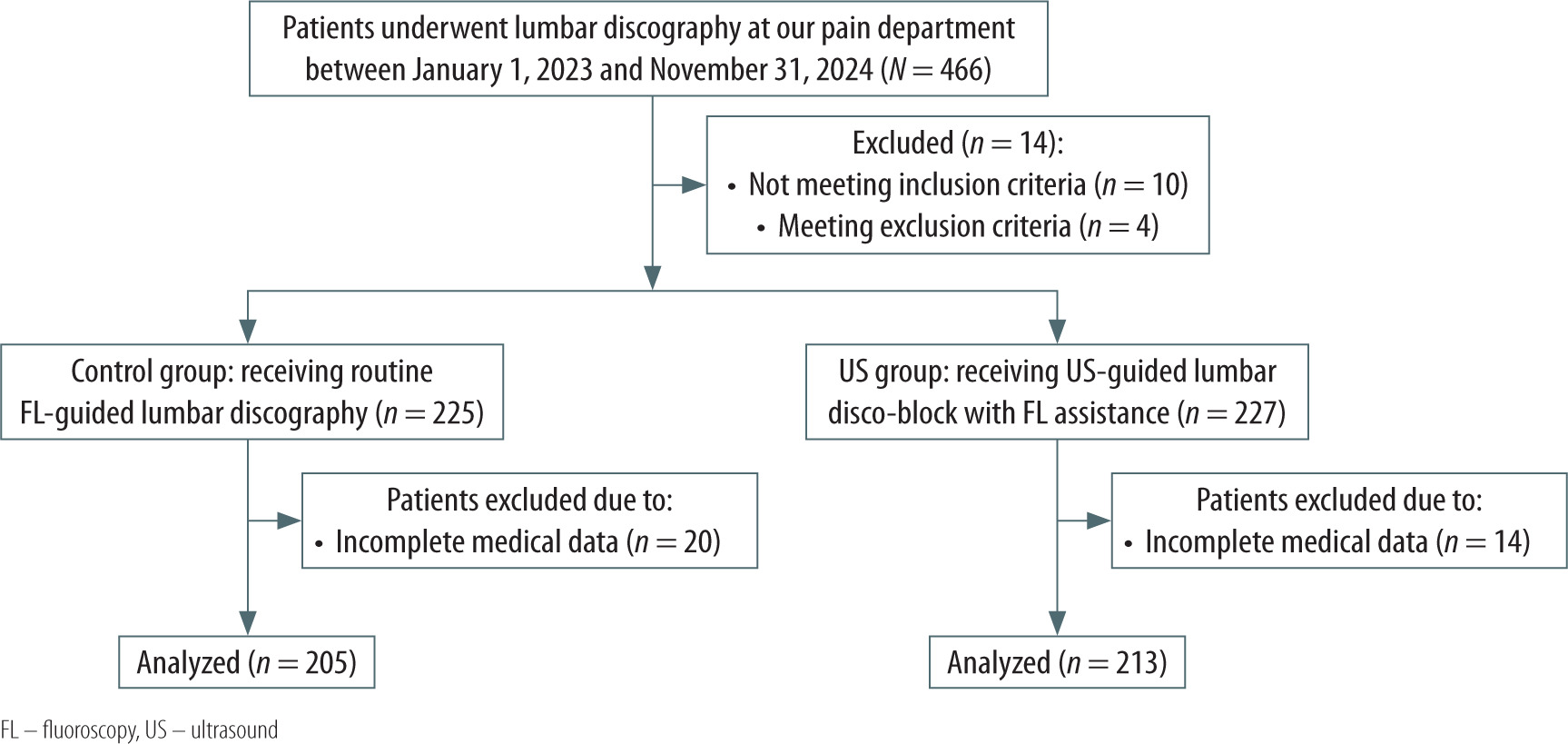
A total of 469 patients were included and divided into two groups based on the procedure they received: the US group, receiving lumbar disc block under US guidance with the concomitant use of FL for confirmation, or the control group, receiving lumbar discography with the assistance of conventional FL and matched to cases in the US group at a ratio of 1 : 1 using a propensity score based on baseline characteristics (Figure 1).
Procedure management
The procedures were performed by the same team of pain interventionists with more than 5 years’ expertise in invasive techniques for chronic spinal pain in the outpatient operating room. The proceduralist decided which disc to perform based on the spine surgeon’s request. Patients were prepared in a prone position and monitored by electrocardiography (ECG), non-invasive blood pressure and pulse-oximetry (SpO2).
Fluoroscopy-guided lumbar discography procedure
With a radiopaque marker in the mid-region of the lumbar spine as a point reference, a single anteroposterior (AP) view was performed to note the level intended to be injected. The C-arm was then tilted to line up with the endplates of the intended vertebral level. An image of the mid-portion of the intended disc was obtained to align the edge of the superior articular process, when the C-arm was rotated towards the side of skin entry. After sterilization, a 22-gauge needle (Nerve Block Needle, 15 cm, Shenzhen Huasheng Medical Technology Co., Ltd., China) was inserted through the skin entry point and advanced towards the center of the intervertebral disc (IVD) in this oblique view. Both an AP and lateral fluoroscopic view were manipulated to confirm the accuracy of the needle tip position in the center of the disc. The precise position of the needle tip was adjusted by advancing it slightly deeper and not beyond the 6 o’clock position of the vertebral pedicle under FL without contrast medium confirmation. After negative aspiration of blood or cerebrospinal fluid, an injection of contrast medium was administered under pressure, and initial contrast spreading into the nucleus pulposus was then verified under fluoroscopy with the final AP and lateral view.
Ultrasonography-guided lumbar disc block procedure
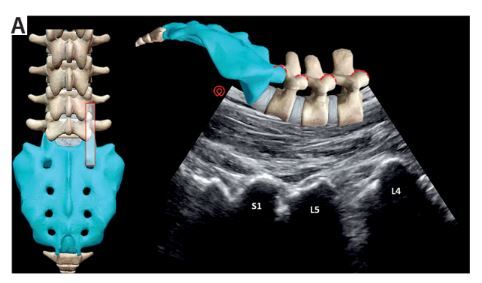
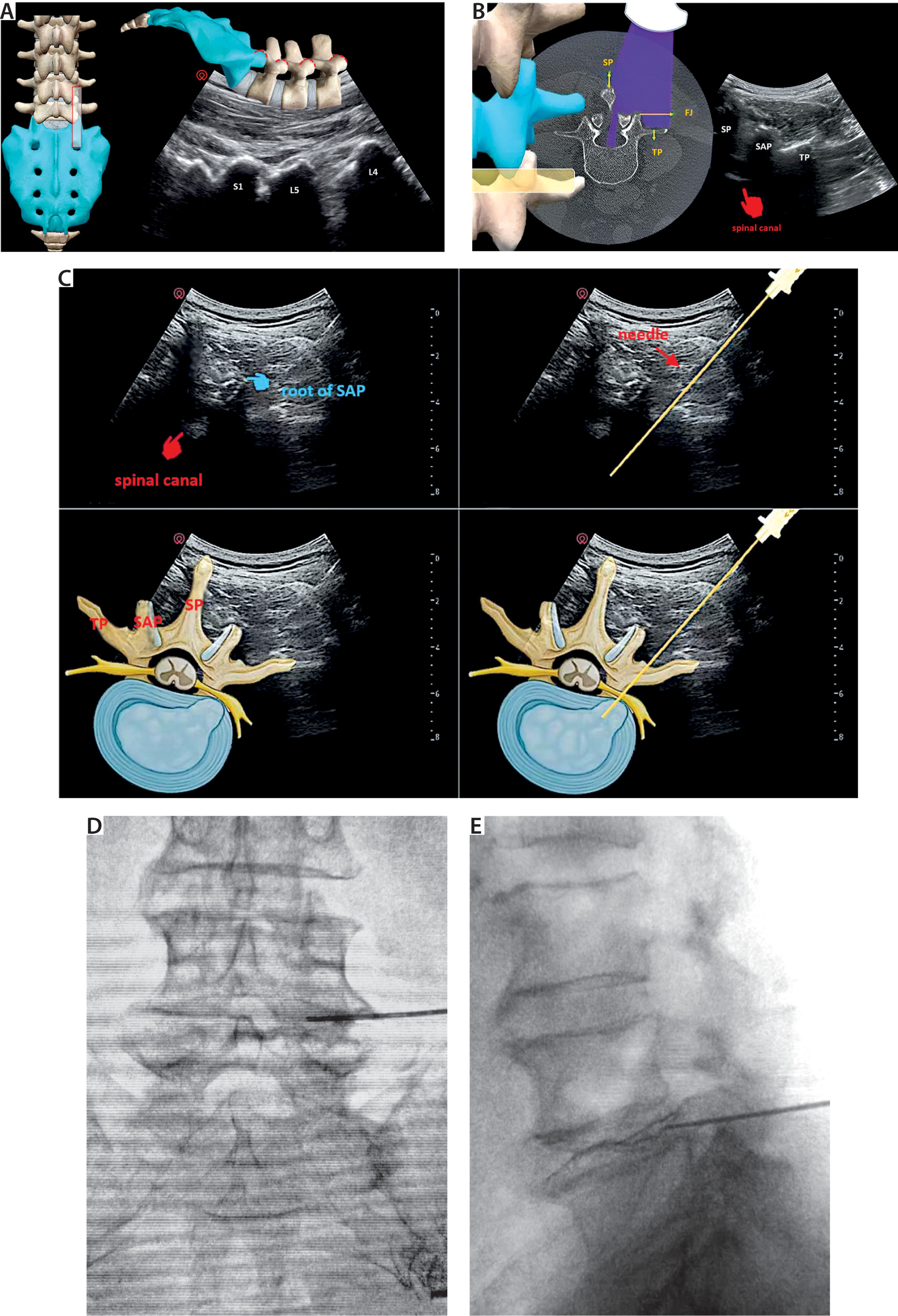
Patients were placed in the prone position with the same monitor as the FL group. A 2–5 MHz curvilinear probe (Labat, Shenzhen Huasheng Medical Technology Co., Ltd., China) was longitudinally positioned on the midline to visualize the spinous processes to count the levels of the lumbar spine. The transducer was moved to the lateral position until the spinal canal was seen between the two adjacent laminas; in turn, the window for the facet joints was visualized on this paramedian sagittal US image by moving the probe further laterally (Figure 2A). As the probe was rotated to the axial plane at the targeted lumbar segment, the facet joint was identified as a hyperechoic curve with its acoustic shadowing beneath. By means of slightly moving the transducer caudally, the two hyper-echoic bony cortices of the superior articular process (SAP) and the transverse process (TP) were connected in the sonographic short-axis view (Figure 2B). As the probe was manipulated slightly backwards cephalad just above the TP, the intervertebral space was situated under the root part of the SAP, which should be emphasized as the landmark used in the US approach. The trajectory of the needle was pointed to the center of the interlaminar space, passing just outside the SAP, known as the “camel’s hump” sign, until the bony structure of the posterior vertebrae just disappeared on US imaging. The same 22-gague puncture needle as the FL group was inserted at the skin entry point and advanced slowly using the in-plane approach under real-time US guidance (Figure 2C). The needle tip was adjusted slightly caudally if patients reported paresthesias due to irritation of the nerve root by the needle. After it entered the IVD with a distinctive decrease in resistance, the transducer was titled back to the long axis of the lumbar spine to confirm that the needle tip was inside the IVD using the out-of-plane technique. Needle tip positioning and intradiscal contrast dispersion were verified under the AP (Figure 2D) and lateral view of FL by injection of contrast agent (Figure 2E). Accordingly, a total of 0.75 mL of 0.5% bupivacaine was injected into the disc for the disc block.
FIGURE 2
Photograph showing the ultrasound (US)-guided lumbar disc block with fluoroscopy verification. A) The long axis of the facet joints was visualized by placing the US transducer from the midline to the lateral. B) The short-axis image showing the hyper-echoic bony cortex with its acoustic shadowing beneath consisted of the superior articular process (SAP) of L5 and the transverse process (TP) of L5. C) The trajectory of the needle was directed towards the center of the interlaminar space, passing just posterior to the root of the SAP of L5, identified as the “camel’s hump” sign on the transverse US scan, until the TP of L5 just disappeared from view. Fluoroscopic anteroposterior (D) and lateral view (E) verified intradiscal contrast dispersion in disc L4/5 following the US-guided approach
Measurement of outcomes
All patients were followed up for a period of 1 month after surgery by specially trained nurses from the department of orthopedics according to the routine protocol. Data collection was performed by our investigators. An 11-point numeric rating scale (NRS) ranging from 0 to 10 was used to assess the severity of LBP [16]. The Oswestry Disability Index (ODI) was used to assess functional disability, which comprised ten items about various daily activities related to LBP. Each item was scored on a Likert scale of 0 to 5 points, and the final score was transformed to a scale of 1 to 100 by multiplying the total score by two. A higher score indicated more severe disabilities [17]. Positive discography was defined as significant pain reproduction with an NRS score ≥ 7 during the procedure, while positive disc block was defined as a significant pain reduction with a decrease of the NRS score ≥ 50% at 60 min after the procedure. The level of response to the diagnostic procedures in both groups was taken into consideration for a subsequent operation. The confirmatory rate was pre-defined as the rate of clinical success following lumbar fusion surgery by an NRS score ≤ 2 and an ODI score ≤ 15 at the 1-month follow-up point, without use of any analgesic. Intradiscal contrast spread during the procedure was predefined as contrast accumulated locally in nucleus pulposus without peri-radicular filling. Procedure time was defined as the time from skin anesthesia to the completion of contrast injection to the IVD. The number of attempts to adjust the needle until contrast was given, radiation dosages and complications during the procedure were also recorded.
The primary outcome was the confirmatory rate of provocative discography or successful disc block, as confirmed by the NRS score in combination with the ODI score at postoperative 1-month follow-up.
Sample size calculation
Sample size was calculated using PASS software version 16 (NCDS, LLC. Kaysville, Utah, USA). The study was designed to establish the non-inferiority of the US-guided lumbar disc block compared to routine discography. Historically, discography has demonstrated a confirmatory rate for successful outcomes after surgery from 60% to 80% [18–20]. The authors would recommend the US-guided disc block even if it were slightly less effective. To detect a noninferiority margin of –10% between two groups, a sample size of 186 cases in each group at a ratio of 1 : 1 was calculated to achieve a power of 90% and a one-side statistical significance of 2.5%, assuming the actual difference ranges from –10% to 5%. Anticipating 20% loss to follow-up, the sample size was adjusted to 233 discs in each group.
Statistical analysis
Statistics were performed using SPSS 22.0 (IBM Corp.). Significance was set at P < 0.05. The Kolmogorov-Smirnov Z test was performed to assess the normal distribution of all data. Normally distributed data, non-normally distributed data, and categorical data were expressed as mean ± standard deviation (SD), median ± interquartile range (IQR), and frequencies/percentages, and compared between groups using Student’s t-test, the Mann-Whitney U test, and the χ2 test. Repeated-measures, mixed-design analysis of variance (ANOVA) was used to compare the repetitively measured data over time, taking their baseline value as a covariate. Post-hoc comparison was conducted using Bonferroni correction at an adjusted significance level of 0.05/3 = 0.017.
RESULTS
Figure 1 illustrates the study flow diagram. As shown in Table 1, patients’ demographic and clinical characteristics were well balanced between the two groups at baseline.
TABLE 1
Demographic information and clinical characteristics for two groups at baseline
The clinical outcome between-group comparisons are presented in Figure 3 and Table 2. Intradiscal contrast dispersion was observed in 95.8% of cases in the US group, and 97.1% in the control group (P = 0.601). NRS pain scores in both groups were significantly decreased over time after lumbar fusion surgery, compared to the baseline value. Similar, the post-operative ODI scores of the two groups across all time points were significantly improved compared with those before surgery. However, there were no between-group differences in NRS scores and ODI scores at the 7-day and 1-month follow-up point. The confirmatory rate was 71.8% in the US group and 73.2% in the control group, with a mean difference of –1.3% (95% CI: –9.9%, 7.2%). With the lower limit of the 95% confidence interval above the non-inferiority margin, the results revealed that lumbar disc block under US guidance was non-inferior to conventional lumbar discography using FL assistance in the diagnosis of DLBP for fusion surgery.
FIGURE 3
Numeric rating scale (NRS) pain scores and Oswestry Disability Index (ODI) scores in both groups over time. Significant reductions in NRS scores (A) and ODI scores (B) after lumbar fusion surgery were observed, compared to the baseline value. There were no between-group differences at the 7-day and 1-month follow-up point
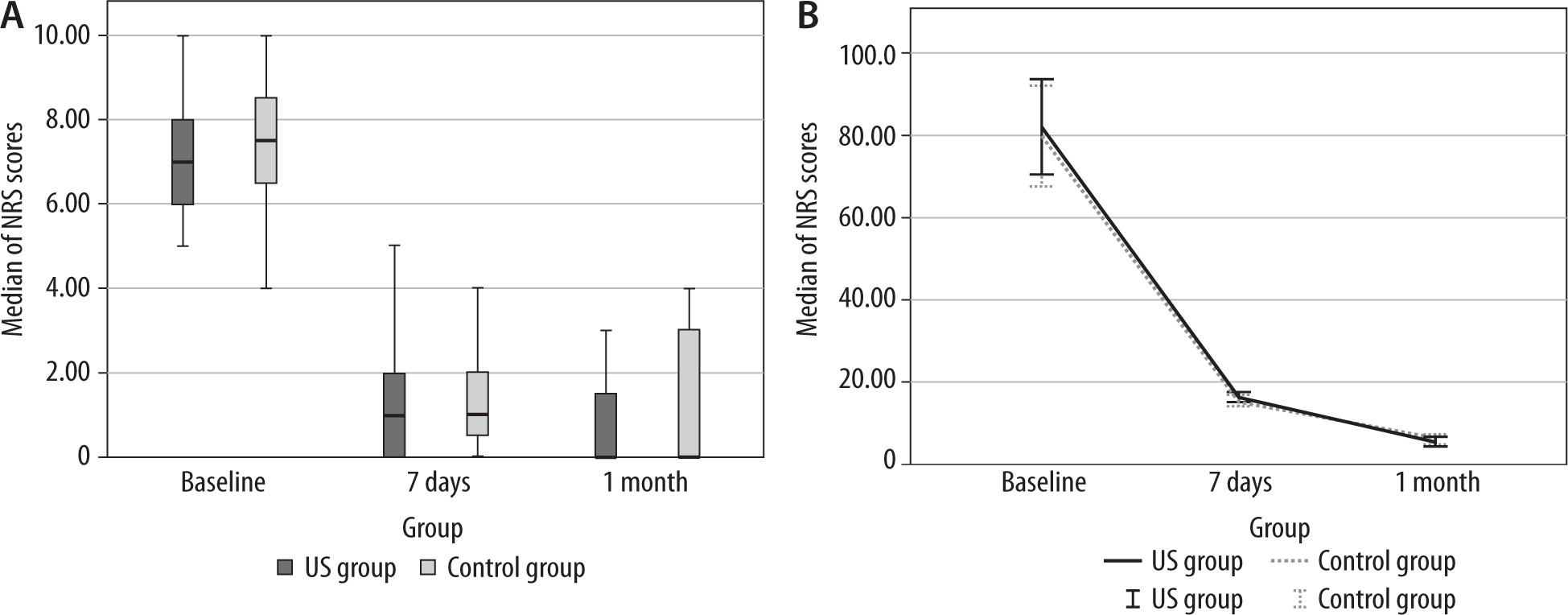
TABLE 2
Comparison of procedure variables between US group and control group
The number of needle insertions until administration of contrast was statistically lower in the US group [2 (IQR: 1–3) (range: 1–5) vs. 5 (IQR: 4–6) (range: 2–7), P < 0.001], indicating that the application of US real-time guidance significantly facilitated the needle placement during procedures. As a result, the procedure time in the US-guided group (8.94 ± 2.28 min) was significantly shorter than that in the FL-guided group (16.13 ± 3.39). The actual disc access time was also shorter in the US group (2.13 ± 0.82 vs. 2.86 ± 1.04, P < 0.001). The mean radiation dosage significantly decreased to 1689.56 ± 898.54 μGy m2 as compared to that for the FL-guided group (8293.50 ± 1039.09 μGy m2) (Table 2).
Serious complications including disc infection, visible hematoma, nerve root injuries, and vascular injection were not encountered in either group. Only 6.7% of nerve root irritation occurred in the US group, compared to 13.0% in the FL group (P = 0.044). Minor side effects such as dizziness, nausea, vomiting, facial flushing, and severe puncture point pain were detected in 10.8% and 14.5% of cases in the US- and FL-guided group (P = 0.295), all of which were resolved within 30 min.
DISCUSSION
This retrospective case-control analysis is the first to estimate the confirmatory rate of US-guided lumbar disc block with FL verification, supporting the use of a simplified sonographic approach, as compared to the conventional FL-guided discography. Our results demonstrated that contrast- enhanced US-guided lumbar disc block potentially possesses both the diagnostic ability for DLBP suspected of requiring surgery and the functional capability of shortening performance time as well as reducing radiation exposure.
Lumbar interbody fusion surgery with or without Da Vinci Robot assistance has been considered as the gold standard in these DLBP cases. The risk-benefit balance must be carefully weighed due to fusion failure caused by adjacent segment degeneration [5, 21]. In this regard, the most urgent need is to identify the responsible disc. The function of the IVD is to distribute pressure evenly across the spine and allow for its flexion, extension, and rotation. The IVD has two major parts: the nucleus pulposus (consisting mainly of a proteoglycan network and hydrated gel), which provides most of the shock-absorbing properties, and the annulus fibrosus, which surrounds it and anchors the disc to the vertebral endplates. The fissures in the postero-lateral aspect of the anulus allow the inner nuclear material to extrude through and evoke the DLBP [5]. A meta-analysis revealed that the presence of degenerative events including a high-intensity zone (HIZ), Modic changes ≥ one-third of vertebral body height, and significant disorganization of the nucleus on T2-weighted magnetic MRI images may predict DLBP. However, it is not validated for the diagnosis of discogenic pain due to low predictive value [22]. Provocative discography may still be employed as the ideal test when there is a moderate to high pretest probability that the pain is suspected to be of discogenic origin on MRI, and the primary pain generator remains unclear [23].
In accordance with the practice guidelines from the Spine Intervention Society (SIS) and the International Association for the Study of Pain (IASP), to date, different approaches for the routine diagnostic application of lumbar discography have been reported: fluoroscopy- or CT-guided [24]. With the fluoroscopic approach, once the center of the disc is visualized just lateral to the SAP and above the TP, direct access to the disc is easy. However, the major difficulty in the two modalities was to keep the needle at the axis of the laser beam during initial insertion through the skin [25]. In addition, since its initial application by Lindblom, the accurate placement of the needle tip is the most basic for an accurate discography. Theoretically, the center of the disc was considered as the most accurate position for the needle tip [26]. Nevertheless, to our knowledge, it was difficult to place the needle tip exactly in the center, and the needle tip was inserted somewhat removed from the center of the disc in many instances in clinical settings. A previous study reported that 85% to 90% of needles were successfully positioned in the nucleus pulposus [25]. Their data objectively proved the importance of accurate placement of the needle tip in lumbar discography, strongly agreeing with our results.
In contrast to fluoroscopic techniques, US imaging overcame these limitations and provided better visualization of soft tissue, peripheral nerves, and vascular structure. The needle positioning can be tracked in real-time image guidance while overcoming the major difficulty in the current techniques [27]. The use of US-guided intradiscal injection has been recently described in a few studies with a series of cases and proved the intradiscal needle placement [14, 28, 29]. Consistent with the previous literature, our study employed a short-axis US scan to help in viewing the sonographic anatomy of the SAP at the targeted lumbar segment to validate the needle tip in the intervertebral disc for the disc block procedures. The trajectory of the needle could be seen clearly from the skin entry to the targeted point inside the annulus fibrous on the US plane. After penetration of the annulus fibrous, it was easier to insert the guiding needle 1–2 cm into the nucleus pulposus instead of advancing it to the center of the nucleus pulposus. The clinically acceptable range of the needle tip position for intradiscal injection was limited to the central 2/4 of the disc on the posteroanterior image and to the central 2/5 to 3/5 of the disc on the lateral view by FL [28]. Subsequently, contrast spread was confirmed under FL. As expected, intradiscal contrast dispersion was observed in 95.8% and 97.1% of cases in the US and control group, respectively. As a result, the confirmatory rate was 71.8% for the US group and 73.2% for the control group, which proved that US-guided disc block was not inferior to conventional FL-guided discography in diagnosis of DLBP.
Another disadvantage of fluoroscopic techniques is radiation exposure of the pelvis and gonads. According to a conventional fluoroscopic guidance, the precise needle placement was always adjusted radiographically, and then the access site was subsequently chosen. Usually, more attempts and insertions for needle placement with a longer performance time were observed during the FL-guided discogram, and CT-based procedures were associated with a much higher radiation exposure [29, 30]. Conversely, it became technically feasible to perform when US with FL assistance was used, because the in-plane technique kept the full length of the needle at the axis of US imaging under real-time visualization. There was complete agreement between the present study and previous research reporting the easier accessibility of US-guided needle insertion with or without FL assistance with a shorter procedure time and actual disc access time [31]. Based on our findings, the radiation dosages were also significantly lower in the US-guided method than the approaches by means of fluoroscopic guidance alone.
With regard to the complications, a previous review showed that post-discography complications were uncommon, since safety measurements were implemented during the invasive procedures of discography. Major risks usually included disc infection, vascular injury or hemorrhage, and nerve root injury [32]. The incidence of discitis was 0.25% among the 4981 patients analyzed in a comprehensive review, with most of the studies analyzed not administering prophylactic antibiotics [33]. No discitis was reported in the present study, which might be attributable to the meticulous maintenance to the strict sterile technique. At the same time, we emphasized that any patient who complained of worsening pain or fever at 1 week after the procedure warranted re-assessment for this potential complication. Given the approach of Kambin’s triangle to the disc space and the smaller size of the needles generally used, serious bleeding or nerve injuries were extremely unlikely [34]. In this study, the trajectory for needle insertion staying close to the SAP at the targeted lumbar segment could keep the needle tip as far as possible from the traversing nerve root. In our experience, a total of 419 discs were tested without any complication of vascular injection or nerve root injury. In addition, paraesthesia on account of the irritation of the traversing nerve root was reported in fewer cases in the US group than the control group (6.7% vs. 13.0%, P = 0.044). Furthermore, a comparable incidence of minor side effects, such as nausea, dizziness, and post-procedure back pain, was reported in both groups, which was also in accordance with previous evidence [35].
There were several limitations. Firstly, confounders and bias might occur due to the retrospective nature of this study with observational data. Secondly, mitigation of irritation of the traversing nerve root would be highly dependent on the learning curve experience with needle placement using the US guidance technique. Thirdly, a well-designed, randomized, controlled study will be required to confirm our results in future.
CONCLUSIONS
In this study, the use of a simplified approach of contrast-enhanced US-guided lumbar disc block provided noninferiority in terms of confirmatory rate for successful outcome following lumbar fusion surgery versus conventional FL-guided discography. The real-time guidance facilitated needle placement, attenuated radiation exposure, and decreased the risk of vascular injection or nerve injury. Therefore, this technique might serve as an alternative to surgery.