
Dear Editor,
Etomidate is often consider-ed an ideal induction agent in cases with a high risk of post-induction hypotension [1]. In addition to its anaesthetic properties mediated by g-aminobutyric acid type A receptors, it has a stimulatory action on central a2 adrenergic receptors, resulting in little change in blood pressure and heart rate. Etomidate is a potent inhibitor of steroid synthesis, with inhibition of the enzyme 11b-hydroxylase. This effect has not transformed into clinically significant hypotension or mortality in the available studies among surgical patients. Large retrospective series among cardiac surgery patients showed no increase in post-operative hypotension, ICU stay, or hospital stay with etomidate [2]. Evidence on mortality with etomidate from meta- analyses of studies on sepsis has provided conflicting results. A 2012 meta- analysis of 5 studies showed an increase in mortality [3], whereas a 2015 meta-analysis of 18 studies showed no increase in mortality [4]. Both these studies did show an increased risk of adrenal insufficiency with etomidate use in sepsis. We describe a case where the patient developed hypotension 8 hours (h) after the surgery, requiring vasopressor support for more than 48 h, owing to adrenal insufficiency, with a prompt response to steroid administration. Written informed consent for publication was obtained from the patient.
A patient in their 50s presented with abnormal uterine bleeding of 6 months duration due to multiple uterine fibroids and was planned for a total abdominal hysterectomy. History was significant for coronary artery disease with dilated cardiomyopathy, diabetes, hypertension, and rheumatoid arthritis. The usual medications included oral aspirin, atorvastatin, hydroxychloroquine, valsartan, glimepiride, and sitagliptin. There was no history of steroid use in the last 5 years. Examination showed a weight of 54 kg, height of 148 cm, heart rate of 68/min, blood pressure of 110/ 66 mmHg, room air saturation of 99%, and normal airway. Twelve-lead electrocardiography (ECG) showed normal sinus rhythm and T inversions in leads II, III, and aVF. Echocardiography showed features of dilated cardiomyopathy with a left ventricular (LV)ejection fraction of 35%, dilated LV, grade II LV diastolic dysfunction, moderate mitral regurgitation, and tricuspid regurgitation. Routine laboratory investigations were normal with a haemoglobin level of 10.8 g dL–1. General anaesthesia with epidural and intra-arterial blood pressure monitoring was planned because of dilated cardiomyopathy. Fasting blood sugar was 130 mg dL–1 and serum sodium was 142 mEq L–1. In the operating room, pulse oximetry, ECG, and non-invasive blood pressure monitors were applied. A 16G peripheral intravenous cannula was secured and the right radial artery was cannulated for invasive blood pressure monitoring. Under strict asepsis, a 20G epidural catheter was placed in the L2–L3 intervertebral space using loss of resistance to air technique. After preoxygenation, the patient was induced with fentanyl 100 µg, etomidate 10 mg, and atracurium 30 mg, the airway was secured with a 7.00 mm cuffed endotracheal tube, and ventilation with O2, air and sevoflurane was initiated. Epidural morphine 3 mg was given and 0.2% ropivacaine infusion was started at the rate of 5 mL h–1. Total intraoperative blood loss was estimated at 400 mL. The patient received 650 mL of crystalloids, 1 g of paracetamol, and 8 mg of ondansetron intraoperatively. The patient was hemodynamically stable throughout the procedure, extubated on table and was shifted to the postoperative ICU with the arterial line in situ.
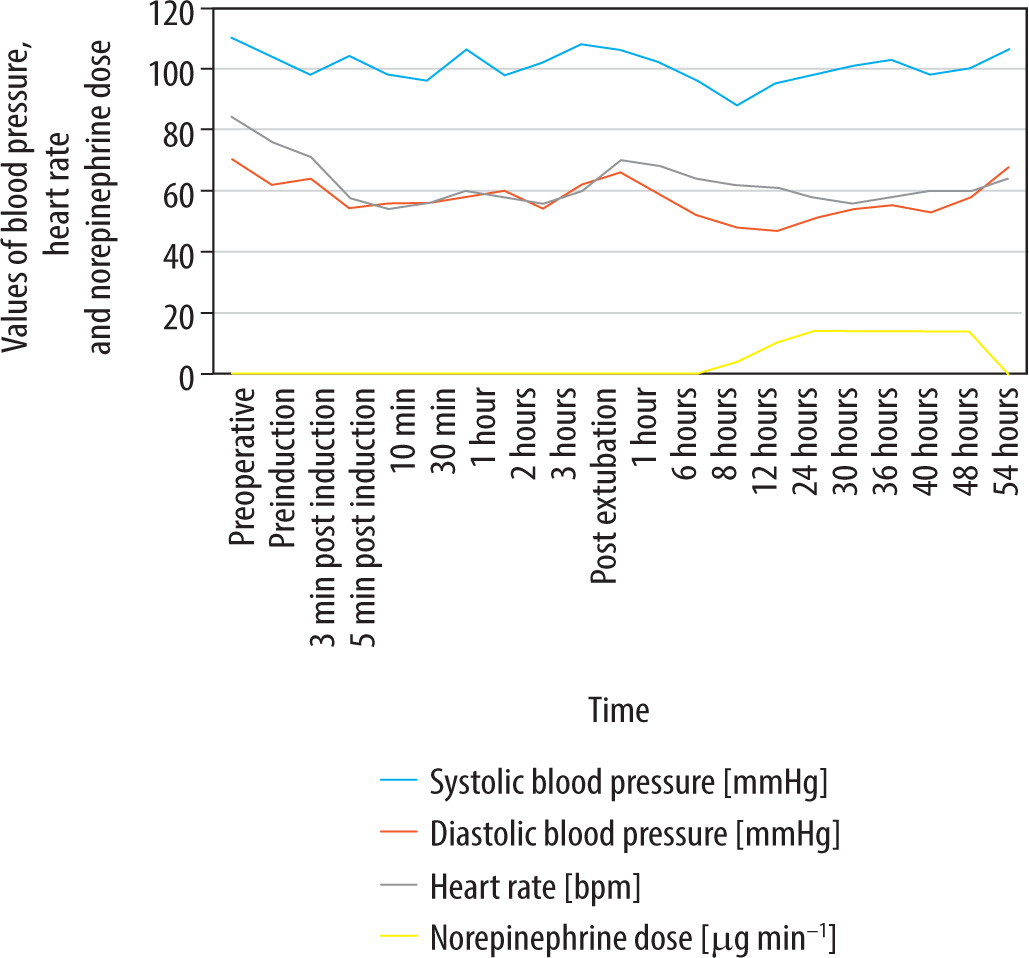
At 8 h postoperatively, the patient developed hypotension, which responded to 250 mL of saline boluses but recurred within a short time. The total amount of fluid received in the first 8 h postoperatively was 700 mL, including intravenous crystalloids at 60 mL h–1 and oral intake. No blood products were given. There was no hypoxia, skin rashes, urticaria or bronchospasm. There were no signs of acute bleeding or ongoing sepsis. A bedside ultrasound ruled out deep vein thrombosis. Cardiac assessment with ECG and echocardiography showed no new regional wall motion abnormalities, normal troponin at 10.6 pg mL–1, and the inferior vena cava diameter was 18 mm with respiratory variability of 30%. Norepinephrine (NE) infusion was started at the rate of 4 µg min–1 and titrated up to maintain the mean arterial blood pressure of 65 mmHg, requiring a ma-ximum of 14 µg min–1 infusion rate. Repeat haemoglobin was 9.5 g dL–1. Tapering NE was attempted but failed and infusion continued at the rate of 14 µg min–1 (Figure 1).
After ruling out the common causes, the probability of etomidate-induced adrenal suppression was considered. At 48 h after the surgery, a high-dose adrenocorticotro-pic hormone stimulation test was conducted with a 250 µg dose. Serum cortisol measured at 30 min and 60 min after injection showed results of 6.08 µg dL–1 and 6.46 µg dL–1, respectively, suggestive of adrenal insufficiency. The patient was given a dose of 100 mg of hydrocortisone intravenously and 50 mg 6 hourly was continued. After steroid supplementation, hypotension resolved, and vasopressors were weaned off in 4 h. Steroids were tapered and stopped over the next 5 days, and subsequently the patient was discharged home.
This case was unique because of the delayed presentation of hypotension and the presence of cardiac comorbidities, which made the diagnosis of adrenal insufficiency challenging. Patients at risk of adrenal insufficiency include those on long-term exogenous steroid use for more than 3 weeks within the previous 3 months, high-dose opiate use, and secondary adrenal insufficiency due to pituitary tumours, infiltrative diseases, and head injury [5]. Our case had no such identifiable risk factor. The prolonged hypotension lasting more than 48 h postoperatively in our patient is also distinctive as relative adrenal insufficiency (RAI) with etomidate was demonstrated to be insignificant after 48 h of surgery [6].
A meta-analysis of propofol versus etomidate in patients undergoing gastrointestinal endoscopies showed a statistically significant reduced incidence of hypotension with etomidate, with an odds ratio of 0.2 [7]. Compared to propofol, it has been shown in randomized studies to cause less hypotension when used as the induction agent [8]. In patients with left ventricular dysfunction undergoing coronary artery bypass graft, etomidate provides superior hemodynamic stability compared with a ketamine–propofol combination [9]. This hemodynamic stability during induction contrasts with the post-operative hypotension due to RAI with etomidate. Studies that looked at adrenal function objectively with post-operative corticotropin stimulation tests among patients undergoing cardiac surgery have demonstrated an increased incidence of RAI lasting up to 24 h postoperatively. A prospective cohort study demonstrated an increase in the norepinephrine dose in patients with RAI, the majority of whom had received etomidate induction [10]. Among critically ill patients, the use of etomidate for intubation was associated with an increase in mortality with a number needed to harm of 31 [11]. In emergency department intubation patients where single-dose etomidate was compared with ketamine, there was no increase in 24-hour and 7-day mortality, but there was an increase in the use of vasopressors after intubation in the etomidate group [12]. Evidence for adrenal insufficiency in critically ill patients is more compelling, with a duration of up to 72 h in 7% of patients receiving single dose etomidate for intubation as deter-mined by the corticotropin stimulation test [13, 14]. In cardiac surgery patients, RAI was shown to be associated with poor long-term survival compared to patients without RAI [15]. Risk factors for adrenal insufficiency include exogenous steroid intake and pituitary diseases, but our case highlights that RAI can occur in the absence of such risk factors with etomidate use. This case report highlights that RAI in noncardiac procedures may also lead to morbidity in terms of prolonged hospital stay and needs to be considered among the differential diagnoses of post-operative shock.