

Dear Editor,
Bezoars are retained concretions of indigestible conglomerations caus- ing various degrees of obstruction within the gastrointestinal tract, most commonly in the stomach; however, occasionally, bezoars originate in the esophagus, resulting in esopha- geal obstruction [1]. Altered gastro-intestinal anatomy and/or motility, supine position, low gastric acidity, diabetes mellitus, neurological conditions, hypothyroidism, other medical conditions, and some medications are predisposing factors for bezoar formation [2].
Enteral feeding by a nasogastric tube (NGt) is a standard form of medical care for patients in the intensive care unit (ICU) due to convenience, low cost and good safety profile [3, 4]: the enteral route tends to attenuate the mucosal barrier breakdown subsequent to bacterial translocation [5]. Bezoar formation due to enteral feeding represents an uncommon complication of malposition of the NGt [6–12].
The following is a report of a case in which a patient with a wide esophageal enteral feed bezoar was managed successfully and quickly by overture-assisted endoscopic removal.
Written consent was obtained from the patient’s relatives for the study and for publication of this case report.
An 80-year-old male patient was admitted to our ICU in a coma with a Glasgow Coma Scale score (GCS) of 6/15 (e4V1M1) after viral encephalitis with spontaneous breathing through a tracheostomy tube. His BMI was 26 kg/m2. He suffered from schizoaffec- tive disorder, was under pharmaco- logical treatment, and had arterial hypertension, non-insulin-dependent diabetes mellitus, osteoporosis, and chronic hepatitis C.
He received total enteral feeding by NGt (Nutricia Flocare, 14-French Polyurethane [PUr] fine-bore tube, length 110 cm). The NGt tube tip po- sition was confirmed using low chest radiography to be in the gastric an- trum. He was started on Jevity Plus (Abbott Nutrition) enteral feeding at 1000 mL per day plus 1 sachet twice a day of Abound (Abbott) dissolved in 250 mL of physiological solution as a protein supplement. Medications administered through the NGt were nebivolol, acetylsalicylic acid, lanso- prazole, amlodipine, and doxazosin.
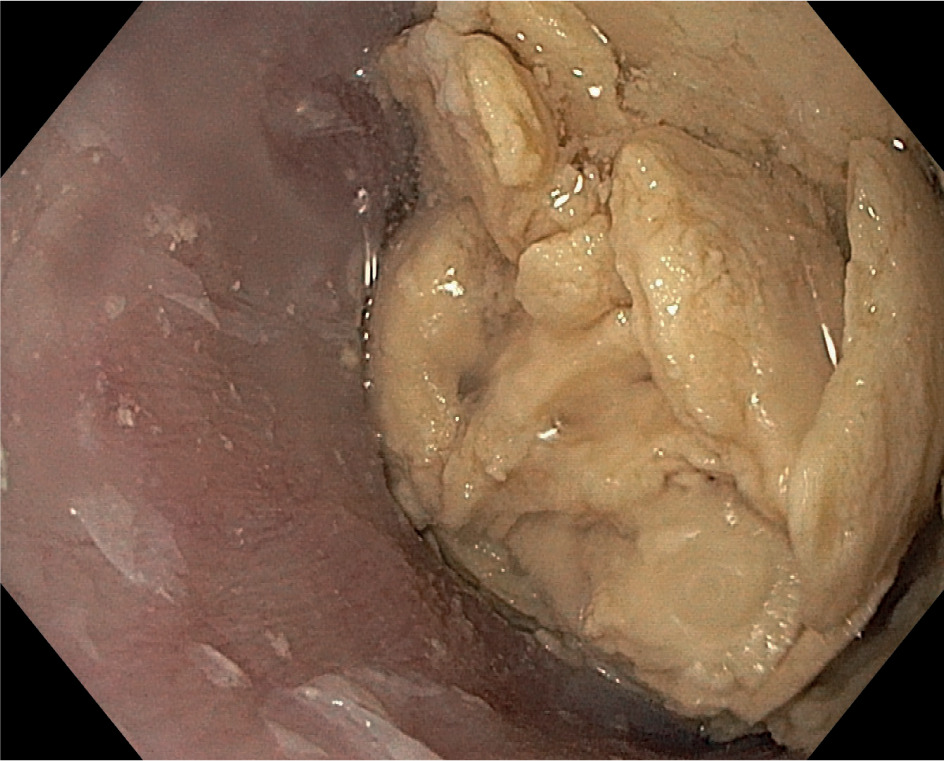
On the 12th day of enteral feeding, the NGt tube tip position on low chest radiography was at the passage be- tween the cardia and gastric fundus. On the 13th day of enteral feeding, due to the patient’s neurological condition and planning his further admission to a rehabilitation center, the NGt was removed and the patient underwent esophagogastroduodenoscopy at the ICU for percutaneous endoscopic gastrostomy (PeG) tube placement, which identified a hard, yellow con- cretion causing a complete obstruc- tion of the esophagus at 30 cm from the incisors (Figure 1). A new NGt could not be inserted. Subsequently, thoracic and upper abdomen com- puted tomography (Ct) scans with- out contrast agent was performed and showed that the length of the enteral feed bezoar was about 7 cm and it completely filled the distal esophageal lumen with associated increased eso- phageal wall thickness.
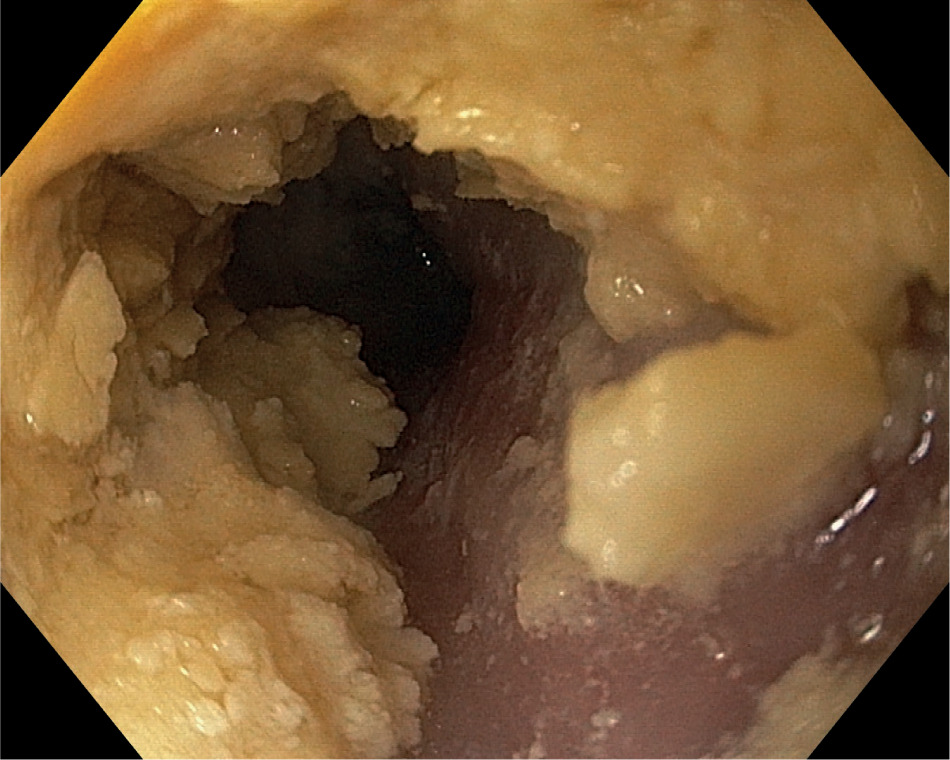
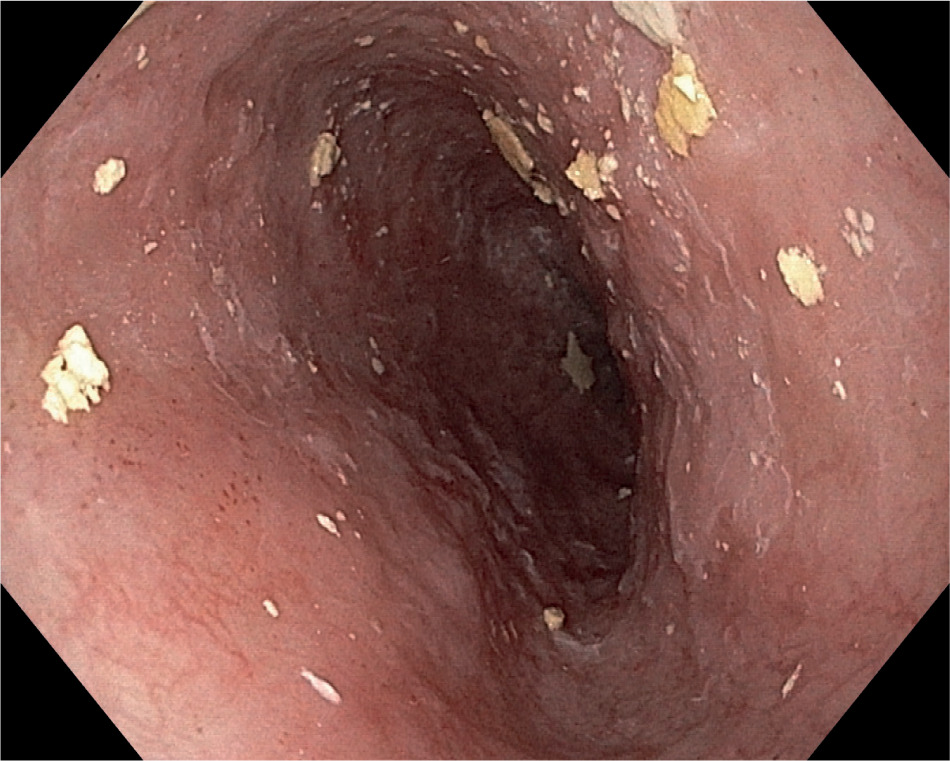
After the Ct scan, the bezoar was safely and quickly removed under the guidance of a Guardus overtube (Steris) 25 cm in length, using both endoscopy devices, such as a retrieval net and a tripod grasper, and a por- table suction aspirator (Figure 2). Partial removal of the enteral bezoar was performed by fragmentation and retrieval by the oral route. Then under water irrigation of the endoscope and simultaneously using a portable suc- tion aspirator the tip of the retrieval net was used to crush the bezoar and create a central tunnel extending to the stomach (Figure 3). The residual bezoar lining the esophagus was frag- mented and pushed into the stomach. No mucosal damage after esophageal bezoar removal was documented (Figure 4).
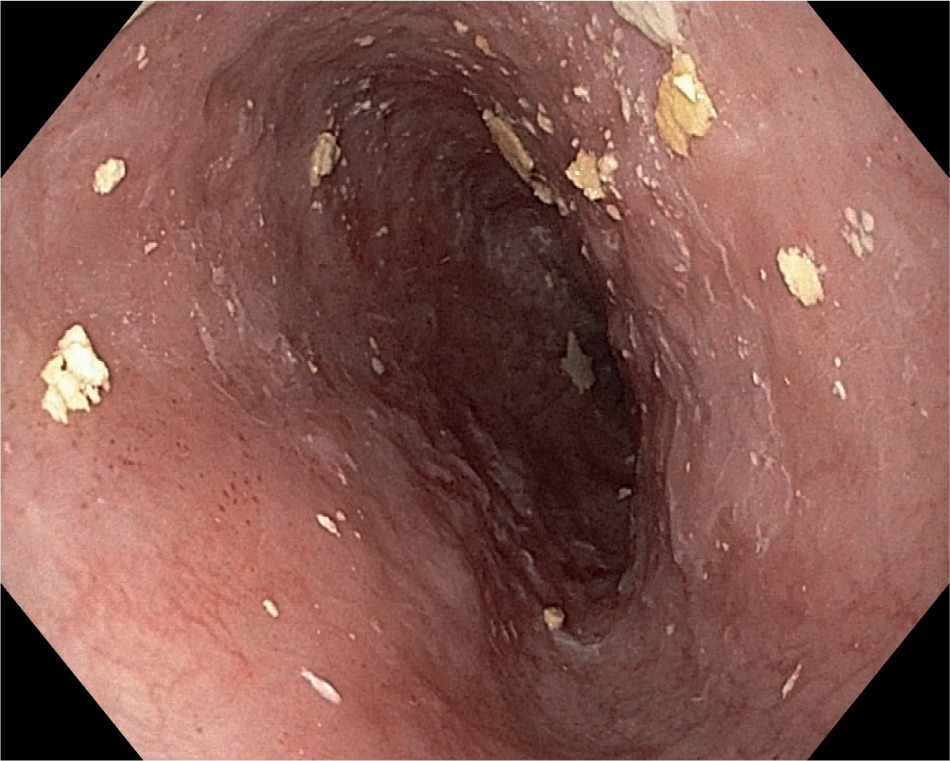
FIGURE 3
Central tunnel extending to the stomach, created using the tip of the retrieval net and portable suction aspirator
Bezoar formation is an uncommon and insidious enteral nutrition complication. Enteral feed bezoars formed during NGt feeding consist of clotted casein (the major protein constituent of milk feeding formula), medications, as well as bacteria, foci of calcifica- tions and cells of the gastrointestinal mucosa [6–8]. Most reports of enteral feed bezoars are related to NGt mis- placement in the distal esophagus, as in our case [12], and their removal rep- resent a challenge. The pathogenesis of esophageal bezoar formation fol- lowing enteral nutrition varies; how - ever, in an in vitro study, Irgau et al. [13] found that stasis of enteral feed for- mula and its fiber does not cause soli- dification by itself, but that it is due to acid gastroesophageal reflux. Ca- sein in the enteric formula clots upon esophageal acid exposure, resulting in bezoar formation [10]. Marcus et al. [6] postulated that casein-based enteral feeding, when exposed to a ph of less than 5, could solidify within 5 minutes, especially in the case of formulas de- ficient in enzymatic substances such as pepsin and pancreatic enzymes [6, 7, 9, 14]. In an in vitro study, turner et al. [14] confirmed this postulate; a similar condition occurred in the third distal esophagus during acid gastroesophageal reflux, as probably happened in our case.
Critically ill patients in the ICU have many factors predisposing to acid gas- troesophageal reflux such as supine position, diabetes mellitus, neurolo- gical disorders, obesity, mechanical ventilation, hypothyroidism, achala- sia, peptic ulcer, casein-based enteral feeding and some bezoar-forming medicines such as sedative analge- sic drugs, drugs containing cellulose acetate, cholestyramine, aluminium, sucralfate and acetylsalicylic acid. All considered, in our case, several risk fac- tors were identified for the formation of the esophageal bezoar, including acid reflux, gastric stasis, the patient’s pathological condition – diabetes mellitus, neurological disorders, and hypothyroidism – and casein-based enteral feeding (Jevity Plus, Abbott Nutrition) through an NGt that was unfortunately displaced in the distal esophagus [8, 10, 14–18].
The NGt increases the risk of ga- stroesophageal reflux since it may induce relaxation of the lower eso- phageal sphincter and interfere with normal esophageal motility and sphincter function [15, 19]. Radio- graphic confirmation of the proper placement of the NGt within the sto- mach is crucial and is considered to be the gold standard [20]. However, even after radiographic confirmation, NGt has been reported to be displaced (e.g. vomiting or in delirious patients) [7, 20, 21]. While routine chest radio- graphy is the gold standard to check NGt insertion, in daily practice, air in- sufflation and auscultation me thods are mostly used to check the correct position of the NGt inside the stomach, and radiology is performed only to answer specific clinical questions, as in our case [3].
In our case, two days before en- doscopic identification of the bezoar, low chest radiography showed the tip NGt position at the passage between the cardia and the gastric fundus. This partial displacement was underes- timated because the NGt was func- tioning properly. In our case, in a few days the NGt misplacement along with casein-based enteral feeding and some crushed bezoar-forming tablets such as drugs containing cellulose acetate, aluminium, and acetylsali cylic acid led to a complete obstruction of the esophagus by the pharmacobe- zoar, but not of the NGt, resulting in an endoscopic incidental finding in an asymptomatic patient. In contrast to our case, the diagnosis of esophageal bezoar is usually performed by radio- logical and endoscopic tests following some presenting symptoms such as regurgitation of the feeding formula, aspiration pneumonia, tracheal com- pression, and bowel occlusion [6–8].
Some measures to prevent esopha- geal bezoar formation should be implemented, such as feeding in a semi-recumbent position, regu- lar flushing of the NGt, radiological periodic checking of the NGt tip, as well as considering administration of prokinetic agents and potentially the endoscopic position of the NGt for feeding [6, 9, 21]. In our case, although the patient was fed in a semi-recum- bent position with a regular infusion rate by an NGt that was regularly flushed and with periodic radiologi- cal checking of the NGt tip, the par- tial displacement of the NGt could lead to serious complications due to bezoar formation (e.g. malnutrition, pharmacological malabsorption, ulcerations of the esophageal mucosa up to the perforation, bleeding, intes- tinal obstruction and the need for life- saving surgery).
Treatment of enteral bezoars is a challenge, and no standardized ap- proach is available; treatment modalities include endoscopic removal, efferves- cent liquids (e.g. Coca-Cola) to soften the mass, dissolution of the mass us- ing pancreatic enzyme extract or bi- carbonate solution, laser lithotripsy fragmentation, and surgical removal [4, 21–23]. Esophago-gastroduodenos- copy is considered the best diagnostic as well as therapeutic tool for gastro- intestinal bezoars [6, 13]. Successful endoscopic treatment involves dis- solution, fragmentation and retrieval of bezoars. Endoscopic management of a bezoar in the esophagus is de- manding to treat, especially due to certain risks such as aspiration during fragmentation and mucosal damage during retrieval, which can be reduced by a protective device such as an over- tube. Overtube-assisted endoscopy is also useful because of multiple pas- sages of the endoscope, especially for a larger bezoar, as in our case, where we successfully, safely, and quickly treated a large bezoar that was occlud- ing all the lumen of the distal esoph- agus using the Guardus overtube (Steris) to guide endoscopy devices such as a retrieval net and tripod grasp- er as well as a portable suction aspirator.