
Stroke is a critical medical emergency that has a significant mortality rate. Currently, it ranks as the second leading cause of death worldwide. Carotid artery stenosis, which is in more than 90% of cases caused by atherosclerotic plaque, is responsible for 15–20% of ischemic strokes [1, 2]. The primary underlying mechanism behind ischemic stroke is atherosclerosis, which involves the formation and progression of atherosclerotic plaques in the carotid arteries [3–5]. While atherosclerotic plaques often do not produce specific symptoms, vulnerable or un-stable plaques pose an increased risk of ischemic stroke [3, 5].
Carotid endarterectomy (CEA) is the most effective and commonly performed surgical intervention for severe carotid stenosis cases [6–8]. This procedure involves surgically removing the atherosclerotic plaque from the bifurcation of the common carotid artery and the internal carotid artery, aiming to reduce the risk of stroke development [9]. CEA surgery can be performed under general anes thesia and regional blockade. The selection of the appropriate method of anesthesia is essential for the entire surgical procedure [10].
Both carotid plaque removal by CEA or isolation by carotid artery stenting has been shown to decrease the risk of ischemic stroke (NASCET, ECST, ACAS, ACST, ACST2, CREST). The high efficiency of the method is also evidenced by the fact that various published studies have reported post-endarterectomy restenosis (the recurrence of stenosis, a narrowing of a blood vessel, leading to restricted blood flow) rates ranging from 5% to 37%, depending on the definition of restenosis and the duration of follow-up [11–13].
Because of a lower risk of periprocedural stroke, CEA is recommended as the first option in patients with acceptable surgical risk (guidelines).
The CEA technique requires clamping of the carotid artery, which may be associated with the risk of ischemia. However, literature data showed that due to the collateral circulation through a circle of Willis, only 10–15% of patients present signs of brain ische mia after clamping and require temporary shunting. Even if clinically uneventful, CEA is associated with transient deterioration in cognitive functions [14].
We hypothesize that this transient deterioration may be caused by a local inflammatory process induced by brain ischemia during clamping, even without clinical signs. The relationship between ischemia and inflammation has already been documented in the literature [14–16]. C-reactive protein (CRP) is a well-known and commonly used inflammatory biomarker. It is produced in the liver in response to proinflammatory cytokines.
Pentraxin 3 (PTX3) is also an acute phase protein secreted, among other cells, by endothelial cells, smooth muscle cells, and macrophages, and is perceived as a marker of local inflammation. Thus, it may be more specific to CRP. Moreover, in distinction to CRP, its serum concentration rises rapidly after the emergence of inflammatory stimuli, reaching its peak within 6–8 hours. It has been demonstrated that the diagnostic sensitivity and specificity of PTX3 for acute coronary syndrome are superior to those of troponin T [14, 17, 18].
The purpose of the study was to analyze the relations between cognitive functions, local inflammation (PTX3 concentration), and duration of brain ischemia in patients undergoing clinically uneventful CEA.
METHODS
Study participants and ethics
The study was conducted on patients who underwent carotid artery stenting or CEA due to carotid stenosis from July 2019 to 2020, and the subjects were screened according to the inclusion/exclusion criteria. Inclusion criteria were as follows: age 20-75 years, ability to provide informed consent, New York Heart Association (NYHA) class II/III, well or moderately controlled asthma, and chronic obstructive pulmonary disease.
Exclusion criteria were as follows: the patient did not consent to regional anesthesia, use of sleeping pills and sedatives in 2 months before the planned procedure, blood pressure exceeding 160 mmHg, or no use of antihypertensive drugs, heart rate below 55 or above 100, glycemia level above 250 mg% or glycated hemoglobin level above 8.5 mg%, glucosuria and ketonuria in the urine, two or more episodes of myocardial infarction, attack or exacerbation of pulmonary disease in the last 30 days before the planned surgery, severe hearing loss or deafness, history of CEA, paresis after stroke, NYHA IV surgery for urgent indications, ejection fraction below 40% and ventricular arrhythmias, paroxysmal atrial fibrillation, patients with active cancer disease. The research was conducted in MSWiA Hospital, Anesthesia Intensive Care Pain Medicine Unit in Poznan, Poland, according to the principles stated in the Declaration of Helsinki. The protocol was approved by the Clinical Research Ethics Committee of Poznan University of Medical Sciences (64/2020).
Cervical plexus block procedure
The blockade was performed under ultrasound control (Drager device, Wiscon WA55-0700998 Ultra sonic diagnostic System Navi S, London, UK) using a 13MHz linear transducer. The local anesthetic was injected using a 70 mm 25GA needle for regional blocks (Vygon Echoplex, Ecouen, France). The superficial cervical plexus block was performed in the patients, depositing 10–20 mL of a local anesthetic between the sternocleidomastoid muscle fascia and the deep cervical fascia at the level of the transverse process C4. The appropriate level of needle insertion was selected by following the course of the brachial plexus from the supraclavicular area to the place where the elements of the brachial plexus disappear. The needle was inserted slightly higher than this point. An additional 5–7 mL of local anesthetic was administered subcutaneously and at the exit of the drain. The effectiveness of the blockade before the start of the procedure was assessed by determining the loss of temperature sensation on the neck skin on the operated side and the lack of heat and cold sensation. The patient was given multimodal analgesia during the procedure. The patient’s vital parameters were monitored: electrocardiogram, blood pressure, body temperature measurements, and saturation measurement.
Carotid endarterectomy method
The patient was placed in a supine position, with the head tilted to the opposite side. Through a longitudinal skin incision along the anterior border of the sternocleidomastoid muscle after sharp division of subcutaneous tissue and platysma and opening of the carotid sheath, the common carotid, internal carotid, and external carotid arteries together with the superior thyroid artery were exposed. The patient was heparinized. The internal carotid, common carotid, external carotid, and superior thyroid arteries were clamped. The patient was observed for signs of brain ischemia. A longitudinal arteriotomy of the common and internal carotid arteries was performed. If signs of brain ischemia occurred, a carotid shunt was performed. The atherosclerotic plaque, together with the inner layer of the media, was separated by blunt dissection from the vessel wall and removed. The backflow bleeding from the internal carotid artery was ascertained. The arteriotomy was closed with a 6/0 continuous polypropylene suture. The use of a carotid patch was left at the discretion of the surgeon. Before the closure of the arteriotomy was completed, the shunt, if placed previously, was removed. The superior thyroid, external carotid, and common carotid arteries, followed by the internal carotid artery, were de-clamped. Once the haemostasis was ascertained, the Redon drain was placed, and the wound was closed.
Blood sampling
Blood for the test was taken directly from the vessel prepared during the procedure before and after placing the vascular clamp using BD Vacutainer SST II Advance tubes (BD Diagnostics, New Jersey, USA). The blood samples were left at room temperature for 15–20 minutes to form a blood clot and then centrifuged for 12 minutes at 3500 × g and 4°C. The serum samples were divided into portions, transferred to 0.5 mL tubes, and stored at –80°C until analysis.
Mini-Mental State Examination
The Mini-Mental State Examination (MMSE) test was performed one day before the procedure, on the first day after surgery, and 30 days after surgery. The NRS (Numerical Rating Scale) test was performed on the first postoperative day every 6 hours to assess the pain scale, and every 12 hours on each subsequent day of the patient’s stay in the vascular surgery department. Pain was treated according to the protocol. Patients received non-steroidal anti-inflammatory drugs, metamizole, tramadol, or drugs from the group of opioids if the NRS exceeded 6. The patient underwent a pre-aesthetic visit 24 hours before the surgery. During the visit, the patient was informed about the type and possibilities of anesthesia.
Pentraxin 3 determination
The concentration of PTX3 in serum blood was determined using a commercially available ELISA kit according to the manufacturer’s instructions (PTX3, SanRed, range: 0.08–20 ng mL–1, sensitivity 0.051 ng mL–1).
Statistical analysis
The results presented in the graphs were prepared using the GraphPad Prism program. Statistical differences between PTX3 concentrations before and after surgery were determined using the Mann-Whitney U-test. In the case of other analyses, the type of statistical analysis used was included in the description of the results and figure legends. Interaction between investigated parameters was performed using Spearman’s rank correlation method.
RESULTS
Changes in PTX3 concentration before and after surgery and operative time
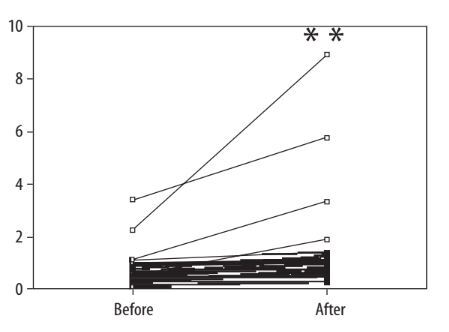
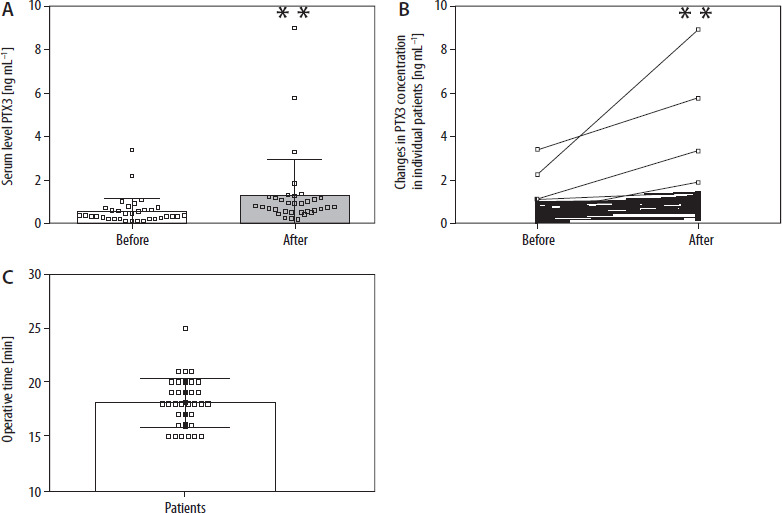
First, we decided to investigate the effect of CEA on PTX3 concentration in blood serum. We noted that the concentration of PTX in serum was statistically significantly higher in patients after surgery compared to PTX level before surgery (Figure 1A–B, P < 0.01). This figure also presents operative time changes in individual patients (Figure 1C).
Changes in MMSE before and after surgery
We also investigated the effect of surgery on MMSE test results 1 and 30 days after the procedure, as shown in Figure 2.
FIGURE 2
Score changes in Mini-Mental State Examination (MMSE) test in individual patients. For this purpose, patients were divided into groups depending on the score changes in the MMSE test (–4, –3, –2, –1, 0, 1, 2, 3, 4 points) compared to the preoperative result
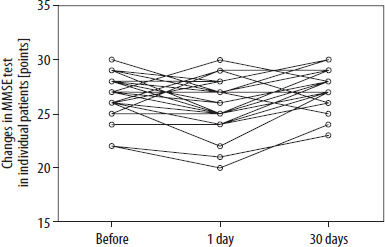
For this purpose, patients were divided into groups depending on the score change in the MMSE test compared to the preoperative result (–4, –3, –2, –1, 0, 1, 2, 3, 4 points) in comparisons regarding changes between hospital admission (before) and 1 day after the procedure (1 day after). Patients were grouped according to score changes of –2, –1, 0, 1, 2, 3, 4 points in comparisons regarding changes between hospital admission and 30 days after the procedure. We noted that a decrease occurred in 23 cases out of 34 patients, which constitutes 67.6% of cases; no changes in the test result were noted in 7 patients, which constitutes 20.6% of the total; an increase occurred in 4 patients (11.8%). Due to the lack of normality, non-parametric tests were used to determine the significance of the change in the MMSE score before and immediately after the procedure: the sign test and Wilcoxon signed-rank test. Next, we examined changes in the test result between one month after the procedure and the day of admission to the hospital. We noted a decrease in the MMSE score in 2 cases out of 34, representing 5.9%; an increase occurred in 26 patients (76.5%), and the score did not change in 6 cases (17.6%). The sign test and Wilcoxon signed-rank test were again used to determine the significance of changes. The comparisons clearly showed that there were statistically significant differences between the MMSE test results in both compared periods: in the case of MMSE before and 1 day after, we noted a statistically significant decrease in MMSE score, while in MMSE before and 1 day after, we showed a statistically significant increase (P < 0.01; Table 1). The decrease (in the case of comparison: MMSE before and 1 day after) and increase (in case of comparison: MMSE before and 30 days after) are shown in the descriptive statistics in Table 2.
TABLE 1
Results of the paired test and the Wilcoxon test comparing changes in the Mini-Mental State Examination (MMSE) test result in the studied periods
Correlations between the duration of the procedure and changes in the MMSE test result and changes in the PTX level
Spearman’s rank correlation coefficients and the standard Pearson’s linear correlation coefficient were used to detect the relationship between the duration of the procedure and the MMSE and PTX results. Spearman’s rank correlation coefficient has the advantage due to the lack of normality of the MMSE change variable and its abrupt nature (small number of adopted values). Nevertheless, both coefficients had similar values, leading to the same conclusions (Table 3). A significant result was the negative correlation between the duration of the procedure and the change in MMSE 24 hours after the procedure. However, the P-value for this relationship was approximately 0.1. Therefore, there was no long-term effect of treatment duration on MMSE. Moreover, the analysis also showed that the duration of the treatment did not affect the concentration of PTX3. It was also found that PTX3 concentration did not affect the MMSE test result.
TABLE 3
Interaction between investigated parameters
DISCUSSION
In this study, we analyzed the effect of CEA on PTX3 concentration after surgery and the potential relationships between PTX3, treatment time, and the MMSE test. We found that the concentration of PTX3 increased after surgery. Moreover, we noted that the concentration of PTX3 significantly negatively correlated (P < 0.05) with changes in MMSE (an increase in PTX3 concentration was associated with a significant decrease in MMSE). These changes were observed both one day and one month after the procedure.
Postoperative cognitive decline (pCD) occurs frequently (6 to 30%) after CEA, although there are no exact estimates, and risk factors are still unclear [19]. Hyperperfusion seems to be a risk factor for pCD, whereas the use of statins is associated with a lower risk of delayed neurocognitive recovery (dNCR). An increased cross-clamping duration could be a risk factor for dNCR [19].
However, an inflammatory parameter such as PTX3 has never been examined directly from blood collected from the carotid artery before and after clamping. PTX3 is an acute-phase protein that is highly sensitive when inflammation occurs, and the factor causing inflammation may include intentional tissue hypoxia during the clamping [20].
A prospective study conducted in China investigated the alterations in cognitive function among patients diagnosed with severe (> 70%) carotid artery stenosis who were presented with three treatment options: CEA (n = 77), carotid artery stenting (n = 81), or medical management alone (n = 77). The cognitive function of all participants was evaluated using the MMSE, the Montreal Cognitive Assessment (MoCA), and the event-related potential P300 at the beginning of the study and again at the 3-month follow-up. Initial MMSE, MoCA, and P300 scores did not differ across the three treatment groups. However, at the 3-month follow-up, patients who underwent either CEA (P < 0.001) or carotid artery stenting (P < 0.001) showed significant improvements in MMSE, MoCA, and P300 scores compared to their baseline values. In contrast, no significant differences were observed in the conservatively managed group. Based on these findings, the authors concluded that both CEA and carotid artery stenting lead to significant enhancements in cognitive function compared to conservative treatment and that the impact of these procedures on cognitive performance is similar.
According to our study, cognitive functions were compared in three time periods: the day before the procedure, the day after the procedure, and 30 days after the procedure. The MMSE scale was used. In our study, a decrease in MMSE occurred in 23 out of 34 patients, constituting 67.6% of cases. No change in test results was noted in 7 patients, accounting for 20.6% of the total, and an increase was observed in 4 patients (11.8%). Changes in MMSE did not follow a normal distribution, according to Shapiro-Wilk test results. Due to the lack of normality, non-parametric tests were used to determine the significance of changes in MMSE scores before and immediately after the procedure: the sign test and Wilcoxon signed-rank test. However, when comparing MMSE scores the day before the procedure and 30 days after the procedure, a decrease in MMSE scores was noted in 2 out of 34 cases, which accounts for 5.9%, an increase was observed in 26 patients (76.5%), and there was no change in 6 cases (17.6%). Both tests unequivocally indicate an increase in MMSE scores one month after the procedure compared to the day of admission to the hospital.
This means that our research, like studies from China, Japan, and Italy, confirms that CEA surgery affects cognitive functions while also indicating that the procedure itself may decrease cognitive functions immediately after the surgery – results of the MMSE scale 1 day after CEA surgery under regional anesthesia. However, a study with a larger group of patients would be necessary to confirm this result.
PTX3 is the archetypal protein within the extended pentraxin subgroup [21]. It consists of a 381-amino acid glycoprotein, characterized by a C-terminal pentraxin domain and a distinctive N-terminal domain [21]. Initially identified in human umbilical vein endothelial cells and human FS-4 fibroblasts during the 1990s, it has since been observed in various cell types, including smooth muscle cells, myeloid dendritic cells, epithelial cells, and tumor cells [22]. The expression level of PTX3 can be modulated by miRNAs, cytokines, transcription factors, and pharmaceuticals [22, 23].
PTX3 plays crucial roles in innate immunity regulation by exerting opsonic activity, modulating complement activation, and forming and regulating neutrophil extracellular traps [24, 25]. Mice with PTX3 overexpression have shown protection against severe inflammatory responses such as lipopolysaccharide-induced endotoxic shock and polymicrobial sepsis induced by caecal ligation and puncture [24, 26]. PTX3 exhibits high affinity and specificity for fibroblast growth factor 2, an angiogenic factor from the fibroblast growth factor family, thereby acting as a natural angiogenesis inhibitor [27]. Furthermore, PTX3 can bind to fibrinogen/fibrin and plasminogen at acidic pH, promoting increased plasmin-mediated fibrinolysis, which is essential for proper repair [28]. Intriguingly, cumulus cells synthesize PTX3 before ovulation, contributing to the organization of the hyaluronan-rich provisional matrix necessary for successful fertilization [29].
We compared the levels of PTX3 before and after carotid artery clamping during CEA surgery. It was found that the level of PTX3 significantly increased in the blood collected after removing the clamp from the common carotid artery. This indicates that even a short period of ischemia to the central nervous system, such as an average of 18 minutes, affects the level of this protein. This may indicate that PTX3 could be a marker for acute cerebral artery ischemia. We also compared the duration of the procedure with changes in MMSE and PTX3 scales.
The duration of the procedure did not affect the change in the MMSE scale or the level of PTX3. This means that PTX3 increases independently of the duration of cerebral hypoxemia/hypercapnia after clamping the carotid artery, and it rises as an inflammatory marker independently within the central nervous system. Regarding the impact of the duration of the procedure on the MMSE scale, the results, however, surprised us. We expected that the duration of the operation might affect cognitive function; however, this assumption proved to be incorrect in our study.
We are also aware of the many weaknesses of our study, which include, among others, a small research group, the absence of a control group undergoing a different surgical procedure, which makes it challenging to attribute observed changes solely to CEA, and the fact that changes were assessed only one month after surgery without a more extended time reference. Despite this, we believe that the manuscript provides new information in understanding the function of pentraxin in metabolism and its changes accompanying CEA treatment.