
Dear Editor,
Pheochromocytoma (PCC) is a rare tumour that develops from the chromaffin cells of the adrenal medulla, resulting in excessive catecholamine production. This tumour can be associated with hereditary syndromes, such as neurofibromatosis type 1, or it can occur sporadically due to genetic mutations [1]. Clinical manifestations of PCC primarily occur because of the overproduction of catecholamines and its mass effect on surrounding tissues. The only definitive effective treatment of PCC is surgical resection. However, preoperative management is crucial to mitigate perioperative risks. According to guidelines, patients undergo pharmacological preparation with a-adrenergic and, in the case of tachycardia, the addition of b1-selective adrenergic blockade to achieve optimal blood pressure (BP) control and to minimise the risk of intraoperative haemodynamic instability. The alternative pharmacological treatment includes phenoxybenzamine and labetalol. In preparing the patient, it is crucial to correct hypovolaemia to ensure haemodynamic stability before further medical procedures. This preoperative regimen is essential to ensure a safer surgical outcome and to prevent potentially life-threatening complications during the tumour removal. We would like to present an uncommon patient with bilateral PCC lesions and an episode of intraoperative haemo-dynamic instability. Written informed consent was obtained from the patient for the study and for the publication of this case report.
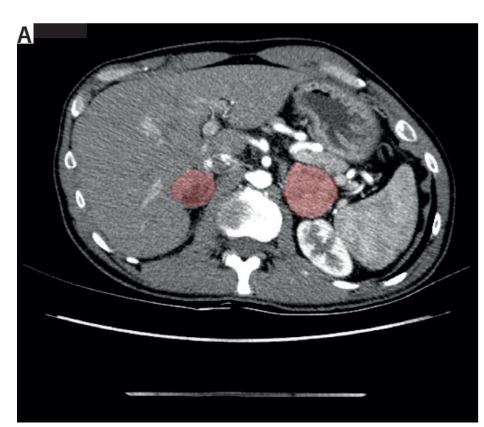
A 34-year-old male with von Recklinghausen syndrome was admitted for diagnosis of bilateral adrenal lesions. The lesions were found on abdominal computed tomography due to newly diagnosed hypertension and episodes of sudden diaphoresis. The lesions were solid, with strong, heterogeneous enhancement after contrast injection, and density above 100 Hounsfield units in the arterial phase, measuring 42 × 35 mm on the left and 26 × 36 mm on the right adrenal gland (Figure 1A). Physical examination revealed numerous café au lait spots, Lisch nodules, and several neurofibromas. Laboratory tests showed full cortisol suppression, elevated urinary metanephrines, increased chromogranin A serum concentration, and hypercholesterolaemia. The patient’s blood pressure (BP) was consistently under 140/90 mmHg on primary hypertension treatment with telmisartan and amlodipine. Suspected of PCC, he was given an initial dose of doxazosin and referred for adrenalectomy. Three months after PCC diagnosis, the patient was admitted to the surgical ward. He was prepared with 8 mg doxazosin twice daily and 2.5 mg biso prolol once daily, maintaining a BP of 120/70 mmHg. On surgery day, he had a brief BP spike to 220/110 mmHg, which then subsided.
FIGURE 1
A) A computed tomography scan of the abdomen with red-highlighted bilateral adrenal lesions. B) A view during the laparoscopic adrenalectomy; the arrow indicates the tumour mass
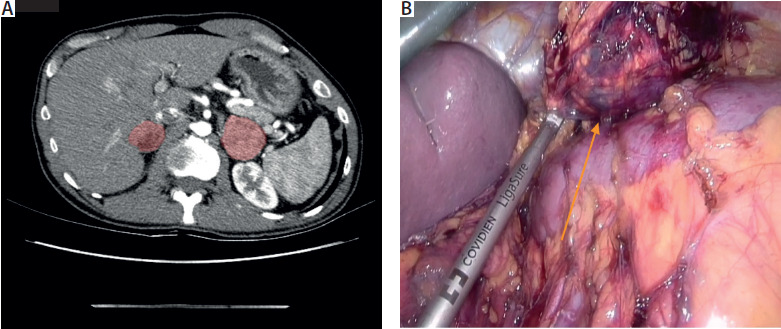
During the induction of anaesthesia, the patient presented with another sudden episode of hypertension and pulseless ventricular tachycardia, resulting in sudden cardiac arrest. After cardiopulmonary resuscitation and 2 defibrillations, nitroprusside diluted in 0.9% NaCl was administered via peripheral venous access, and the return of spontaneous circulation was achieved. Following this event, extended diagnostics were conducted, including echocardiography, computed tomography scan of the heart, and Holter BP and electrocardiography monitoring. The final decision was to postpone surgery. The patient began his second preparation, with 10 mg of doxazosin thrice daily and 6.25 mg of bisoprolol. Three months after cardiac arrest, he was admitted to the surgery again. Left laparoscopic partial adrenalectomy was performed (Figure 1B). After the surgery the patient was haemo-dynamically unstable, requiring high doses of noradrenalin and argipressin infusion. On histopathological examination, PCC was confirmed. The patient was discharged from the hospital in good condition and is currently scheduled for right adrenalectomy for the remaining lesion.
In PCC, released catecholamines induce vasoconstriction and increase the heart rate, leading to hypertension and circulatory instability, making tumour resection high risk [2]. Preope rative a blockade is a standard preparation before surgery [3]. There are specific criteria for adequate a blockade and, in the case of tachycardia, b-blockade, typically initiated 7 to 14 days preoperatively to minimise haemodynamic fluctuations [4]. However, some recent studies suggest no significant advantages of such an approach, prompting questions about the necessity of the blockade [5, 6]. Additionally, it proves to be ineffective in some cases, highlighting the significance of other aspects such as the duration of surgery or conduction of anaesthesia, and their influence on haemodynamic instability [2, 7]. Intraoperatively, phentolamine – a short-acting non-selective a-1 and a-2 antagonist – can be employed for the rapid management of hypertensive episodes associated with PCC [8]. This medication is available in Poland through targeted import. In the presented patient, significant haemodynamic fluctuations persisted despite administration of the maximum tolerated doses of a blockers during preoperative preparation. Consequently, a sodium nitroprusside infusion was initiated prior to the induction of anaesthesia to manage these challenges effectively.
To conclude, this case demonstrates that while a and b blockade can be beneficial, they may not completely prevent haemodynamic fluctuations, further exposing patients to complications related to postope rative hypotension. In similar cases, appropriate management and preparation of anaesthesia are crucial. Gathering similar cases should prompt a revision of current standards.