
In pediatric anesthesia, psychological anxiety and trauma induced by maternal deprivation are significant challenges. Pre-anesthesia medication in pediatric patients should facilitate the induction of anesthesia while concurrently reducing anxiety and psychological trauma to avoid impeding recovery. Numerous pharmaceutical agents have been tested to identify the most effective sedative and route of administration for pediatric patients. Such agents should be administered via an appropriate, nontraumatic route to prevent additional stress. Currently, midazolam, dexmedetomidine, ketamine, transmucosal fentanyl, and meperidine are the most frequently prescribed medications [1].
Ventricular septal defects (VSDs), accounting for approximately 30% of congenital heart diseases, are the most prevalent [2]. Percutaneous device closure has recently replaced surgical repair as the preferred treatment option due to its favorable outcomes and fewer complications [3].
Administering sedative drugs via injection may not be optimal in pediatric cases, as it can exacerbate anxiety and fear associated with needle puncture. Moreover, it requires a higher level of technical expertise, and the child’s lack of cooperation may increase the risk of accidental needle injury to healthcare professionals [4].
The intranasal route has proven to be a reliable, noninvasive, simple, safe, and effective alternative. The nasal mucosa is well vascularized, allowing direct entry into the central nervous system, bypassing the first-pass effect and resulting in rapid onset of action, comparable to the intravenous route [5, 6]. Additionally, this method is highly tolerable, eliminating the need for patient cooperation when swallowing medication or holding it under the tongue. Furthermore, it lacks pungency or a bitter taste [7].
This research aimed to assess and compare the sedative effects of intranasal dexmedetomidine and intranasal midazolam as premedication in pediatric patients undergoing transcatheter closure of VSD.
Methods
After obtaining approval from the Research Ethics Committee of the Faculty of Medicine, Ain Shams University (reference number FMASU R55/ 2023), and registering the study in the Pan African Clinical Trial Registry (PACTR202305793236698), this randomized (using simple randomization), doubleblinded (participants and staff, including data collectors), prospective trial was conducted between April 2023 and March 2024 at the pediatric cardiac catheterization unit of Ain Shams University Hospitals.
Inclusion criteria
The study included children of either sex, aged 3 to 6 years, with hemodynamically significant VSDs, anatomically suitable for transcatheter perimembranous VSD closure, with no coexisting cardiac or medical problems, and with normal ejection fraction and pulmonary artery pressure.
Exclusion criteria
The exclusion criteria comprised parental refusal, uncooperative patients, allergy to the study drug, mental retardation, obesity, and any nasal disease (e.g., recurrent nasal hemorrhage, nasal masses, laryngeal pathology, or obstructive disease of the pharynx) that may impede nasal drug administration.
Study groups
The study enrolled 40 pediatric patients who met the inclusion and exclusion criteria. These patients were randomly divided into two equal groups of 20 using a sealed envelope technique. The groups were initially named Group 1 and Group 2, but were renamed Group M and Group D at the end of the study.
In the Group D (dexmedetomidine group) (n = 20), patients received intranasal dexmedetomidine (0.5 µg kg–1 body mass) 20 minutes before induction (Medrelaxmidine 50 mL vial, 4 µg mL–1, Arabcomed Pharmaceutical Company, Cairo) [8].
For Group M (midazolam group) (n = 20), patients received intranasal midazolam (0.2 mg kg–1
body mass) 20 minutes before induction (Midathetic 5 mg ampoule, Amoun Pharmaceutical Company, Cairo) [9].
All study drugs were prepared by the investigator anesthesiologists. The dexmedetomidine syringe was labeled 1, and the midazolam syringe was labeled 2. They were administered by the attending anesthesiologists, who were blinded to the drugs administered.
The anesthetic plan, including information about fasting hours, current medications, and written consent, was communicated effectively to the child’s guardians. Each patient underwent a thorough assessment of their medical history, clinical examination (including body weight), and airway evaluation. Laboratory tests included a complete blood count, liver and kidney function tests, coagulation assessment, serum electrolyte analysis, and blood sugar level measurement.
All patients were brought to a preparation room outside the catheterization laboratory 30 minutes before the procedure in the presence of one parent. The study medication was administered to the children after measuring their initial mean arterial blood pressure, heart rate, and oxygen saturation in the preoperative room.
The study medication was administered using a 2 mL syringe, with the child in a recumbent position, by trickling the drug into both nostrils. Maximum sedation was achieved within 10–15 minutes in both groups, with no differences in time to sedation and no cases failing to achieve sedation within the expected time frame.
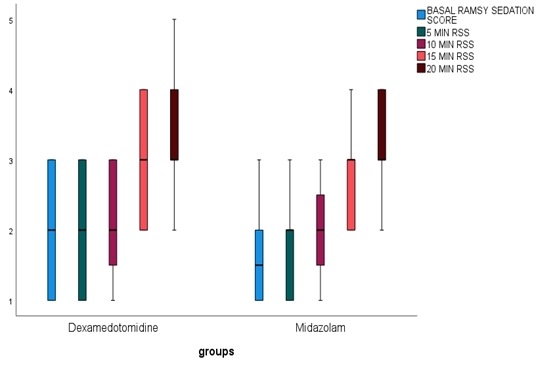
Heart rate, mean blood pressure, and oxygen saturation (SpO2) were recorded every 10 minutes after drug administration until the patient was transferred to the operating room (OR). The level of sedation was assessed by an impartial observer every 5 minutes from the time of drug administration until the child was transferred to the OR, using the Ramsay sedation scale (RSS), a four-point scale measuring the level of sedation. A score of 1 indicated that the patient was alert and awake, while a score of 2 indicated sluggishness and lethargy. A score of 3 indicated that the patient was asleep but responsive to mild prodding or shaking, and a score of 4 indicated unresponsiveness to mild prodding or shaking [10].
The child-parent separation score (CPSS) was assessed during the transfer of the patient to the OR. The child-parent separation score measures a child’s emotional response to separation from their parent. A score of 3 indicates that the child is crying, frightened, and cannot be comforted with reassurance; a score of 2 indicates mild crying or fear that can be comforted with reassurance; and a score of 1 indicates that the child is unafraid, cooperative, or asleep [11].
Perioperative anesthesia plan
Inhalation induction was initiated using a mixture of 4–8% sevoflurane and 100% oxygen. After confirming adequate anesthetic depth, an intravenous cannula was inserted. Fentanyl (1–2 µg kg–1 body mass slow i.v.), propofol (1–2.5 mg kg–1 body mass), and atracurium (0.5 mg kg–1 body mass) were then administered consecutively to induce neuromuscular blockade and facilitate tracheal intubation. Patients were mechanically ventilated with 50% oxygen, and end-tidal CO2 was maintained between 30 and 35 mmHg using a mainstream capnograph. Standard monitoring included ECG, noninvasive blood pressure measurement, pulse oximetry, and capnography. Mean blood pressure, heart rate, and oxygen saturation were assessed at 10-minute intervals during surgery until the patient regained consciousness.
Following the procedure, anesthetic gases were discontinued and replaced with pure oxygen at a flow rate of at least 4 liters per minute. Upon awakening, the endotracheal tube was removed, and the patient was transferred to the postanesthetic care unit (PACU), where vital signs were monitored until discharge to the ward. In the PACU, an anesthetist unaware of the child’s treatment assessed emergence agitation using a three-point scale: 1 = easily awakened, calm, and able to follow instructions; 2 = crying or restless but able to be calmed by verbal commands; and 3 = displaying aggressive, combative, or disoriented behavior [12].
The primary outcome was the effect of preoperative sedatives on the RSS. The secondary outcomes included the effects of preoperative sedatives on hemodynamics and oxygen saturation, child-parent separation score, and child emergence agitation level.
Sample size
The sample size was determined using the STATA program, with a type I error (a) set at 0.05 and a power (1-b) set at 0.9. Based on these parameters, each group’s required sample size was calculated to be 18 cases. To account for potential dropouts, the study included 20 cases in each group, resulting in a total of 40 cases.
Statistical analysis
The data were analyzed using version 27 of IBM SPSS Statistics. The normality of continuous variables was assessed using the Kolmogorov-Smirnov test. Descriptive analyses were conducted to obtain means and standard deviations for normally distributed quantitative data and medians and interquartile ranges (IQR) for skewed data. Qualitative data were presented as numbers and frequencies. Various types of graphs, including box plots and error bars, were used.
Bivariate analyses were performed using the independent samples t-test and the paired Student’s t-test for normally distributed data; while nonnormally distributed variables were analyzed using the Mann-Whitney U-test. The c2 test was used to analyze categorical data. A P-value of < 0.05 was considered statistically significant.
Results
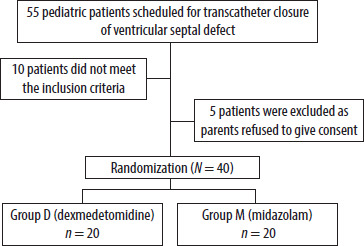
Fifty-five pediatric cases scheduled for transcatheter closure of VSD were evaluated for inclusion in the study. Ten cases did not meet the inclusion criteria, and five were excluded due to parental refusal to consent (Figure 1).
No statistically significant difference between the two groups was observed as per demographic data and procedure characteristics (Table 1). Furthermore, VSD size (5 ± 1/5 ± 1), peak pulmonary artery pressure (27 ± 4.5/26.5 ± 4.3), and ejection fraction (61.5 ± 5.1/61.2 ± 4.2) were not significantly different between Group D and Group M (P-value > 0.05).
TABLE 1
Comparative analysis of Group D and Group M as regards procedure characteristics and demographic data
No significant statistical variation was observed between the two groups concerning pulse rate at various time points (basal, 10, and 20 minutes) during the preoperative (Table 2), intraoperative, and postoperative measurements (P-value > 0.05) (Figures 2–4, Tables 3–5).
TABLE 2
Comparison between Group D and Group M regarding preoperative heart rate (beats min–1), mean arterial blood pressure (mmHg) and oxygen saturation
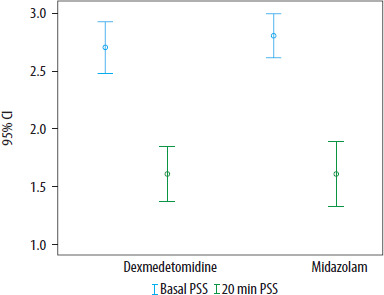
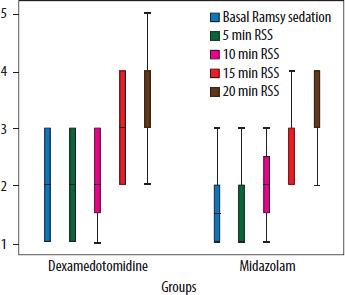
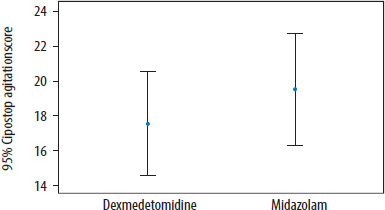
TABLE 3
Comparison of Group D and Group M as per the child parent separation score (CPSS)
| Group D: dexmedetomidine | Group M: midazolam | P-value U-test | |
|---|---|---|---|
| Basal CPSS, median (IQR) | 3 (2–3) | 3 (3–3) | 0.478 |
| 20 min CPSS, median (IQR) | 2 (1–2) | 2 (1–2) | – |
TABLE 4
Comparison between Group D and Group M as per Ramsay sedation score (RSS)
DISCUSSION
The preoperative phase is highly anxiety-inducing for most surgical patients, especially pediatric ones. Alleviating preoperative anxiety is, therefore, a significant priority for anesthesiologists. Various anesthetic premedications are employed to mitigate this stress response. Among these, sedatives such as midazolam and dexmedetomidine are frequently used in conjunction with premedications [13].
The intranasal administration method offers several advantages, including the non-requirement of the child’s cooperation, non-invasiveness, convenience, and lack of unpleasant taste. This method is a painless way to administer premedication drugs to children, with rapid action due to the drug’s fast access to the circulatory system through the highly vascularized nasal cavity. Additionally, it can bypass the hepatic first-pass effect, allowing direct entry into the central nervous system [14].
A study by Messeha and Elmorsy [15] demonstrated that sedation scores were significantly higher in the group receiving dexmedetomidine than in the midazolam group 25 minutes after administration (P < 0.05). However, our research revealed no significant difference between the two groups concerning sedation scores.
Dexmedetomidine, a potent and specific a2-adrenoreceptor agonist, has anxiolytic, sedative, and analgesic effects, primarily exerting its sedative effects by acting on the locus coeruleus, producing a state of consciousness akin to natural sleep. Intranasal administration of dexmedetomidine is less intrusive and anxiety-inducing for pediatric patients, with a lower risk of respiratory and hemodynamic depression [16].
Although its oral bioavailability is low (16% with a peak at two hours), research has shown that the intranasal route is more effective than the buccal route when comparing equivalent doses in pediatric cases. Administering dexmedetomidine intranasally results in a peak blood concentration after 38 minutes, compared to 90 minutes when administered buccally [17].
Midazolam, a benzodiazepine frequently used in pediatric anesthesia, functions as an anticonvulsant, muscle relaxant, and water-soluble GABA receptor agonist [18]. It is fast-acting, with hypnotic effects, and induces anterograde amnesia and anxiolysis without significant adverse effects. Midazolam can be administered intranasally, intramuscularly, intravenously, rectally, or orally [19].
Our results indicated no statistically significant differences in hemodynamic parameters between the two groups at different time points. This finding aligns with the research by Sheta et al. [20], which also found no significant differences between intranasal midazolam and dexmedetomidine as premedication in children undergoing complete dental rehabilitation. Furthermore, there were no cases of bradycardia or hypotension during our work.
In contrast, Saad [14] found significant hemodynamic differences after a 30-minute premedication period in pediatric cases undergoing adenotonsillectomy, where the dexmedetomidine group had reduced heart rates and blood pressure compared to the midazolam group (P < 0.05). However, our study did not reveal such differences.
Both groups in our study maintained stable peripheral arterial SpO2 levels during the perioperative period, consistent with previous findings indicating that dexmedetomidine does not significantly affect respiratory function [21]. Additionally, our trial found no significant differences between the groups’ RSS and child-parent separation score.
Similar results were reported by Akin et al. [22], who found that dexmedetomidine and intranasal midazolam were equally effective in reducing anxiety during parental separation in pediatric patients undergoing adenotonsillectomy.
Our results also found no significant differences in postoperative agitation between the midazolam and dexmedetomidine groups, consistent with findings reported by Akin et al. [22] and Bergese et al. [23]. However, other studies, such as those by Mizrak et al. [24], found that dexmedetomidine was more effective than midazolam in reducing postoperative agitation.