
There is probably no person in the world who has not been affected by the COVID-19 pandemic. Although the impact may have been negligible for the majority, it significantly disrupted the lives of certain individuals. The pandemic profoundly affected both personal and professional lifestyles, eli-citing stress, sadness, fear, and anger. Furthermore, it underscored the fragility of daily life, prompting many to adopt a more short-term perspective. Interestingly, although on balance the pandemic was a negative event, it was one that some feel led to some positive change, such as promoting the possibility of remote work and encouraging a reevaluation of one’s life and its balance.
One of the areas most affected by the COVID-19 pandemic is, of course, the healthcare system. While some countries tackled the pandemic well, others appeared completely unprepared. In a given country, the approach taken to dealing with the crisis was strongly influenced by its social and economic situation, as this translated into specific behaviors that were conducive, or not, to limiting the effects of the pandemic. Some countries responded with few restrictions, while others introduced a range of controls, some of which may not have been reasonable. For example, Sweden took a relatively light touch when applying restrictions, which arguably it could afford to do, due to its low population density, relatively good initial general health, high degree of trust in the authorities, and the tendency of Scandinavian citizens to comply with rules and naturally observe social distance.
Given the disturbing data about numerous excess deaths in Poland during the pandemic, there is a need to understand how this extraordinary state of affairs influenced the occurrence of medical errors in the country and to compare the findings with those from other countries. No such analysis could be found of the situation in Poland, and the studies focusing on other countries tend to be quite general, lacking any in-depth analysis of the problem, most likely because the subject is so recent [1]. Most of them focused on the general causes of mistakes made during the COVID-19 pandemic, with the most common findings implicating work overload and fatigue, lack of sleep, poor delegation of duties, insufficient staff, or lack of experience among junior staff [1–7]. Many also raise the issue of the importance of healthcare workers taking care of themselves and supporting each other (support group); they also highlight the need for the workers to have the opportunity to talk to others, get adequate sleep, and participate in training to improve professional qualifications [4, 8].
Many of the articles took a pharmacological perspective. For example, an Iranian study examined the incorrect administration of drugs, or incorrect doses by nursing staff [9]. French research focused on the issue of pharmacies and the lack of availability of life-saving drugs or those used in intensive care caused by advanced panic buying [10]. The Institute For Safe Medication Practices from Canada highlighted the incorrect dosing of remdesivir, a drug that prevents the multiplication of SARS-CoV-2, resulting from a mistake in the packaging; it also examined the incorrect dosing of oncology drugs resulting from the lack of personal contact with the patient (teleconsultation), and the failure to notice that patients were losing weight and required dose reduction [11]. A Dutch study reported that incorrect drug dosing resulted from incorrect prescriptions caused by fatigue [7]. An American study described, among other things, the problem of incorrect drug dosing during the pandemic, resulting from work overload and insufficient staff numbers. It also criticized the organization of work during the pandemic, in which nurses were isolated together with patients; this resulted in the nurses taking everything that could potentially be useful to them during patient care, and sometimes leaving excess drugs in patient rooms, which could lead to errors [5].
An Iranian study addressed the issue of patients being mistakenly diagnosed with SARS-CoV-2 and the consequences of such incorrect diagnoses [12]. Similarly, an American publication based on eight large medical centers reviewed cases of missed or delayed diagnosis caused by COVID-19; it was found that 257 cases of medical errors were identified in the period February-June 2020, and only 36 of them were classified as caused by COVID-19 [13].
Most articles present general comments on improving the healthcare system [14]. For instance, a study conducted in the United States investigated the reasons behind the decline in emergency room admissions during the pandemic. The study suggested that patients avoided seeking care in the Emergency Department due to concerns about SARS-CoV-2 infection, prolonged waiting times for admission, and fear of potential errors committed by overburdened medical staff. Additionally, some individuals perceived their medical conditions as less urgent compared to those diagnosed with COVID-19. Interestingly, this smaller number of patients may well have contributed to the observed decrease in the number of such errors [15]. Another study in the USA highlighted a major problem associated with teleconsultations resulting from system overload, cancellation of operations and planned visits, and delayed or unimplemented therapies; in particular, its use was associated with poorer cancer screening and a resulting increase in deaths [16]. Finally, the pandemic had also a dele-terious impact on prophylactic programs, for example: according to the WHO, in 2022, as many as “20.5 million children missed out on one or more vaccines delivered through routine immunization services” [17].
It was also highlighted that staffing problems resulted in employing junior staff with less experience, who were more likely to make mistakes [5]. The Institute for Safe Medication Practices drew attention to the exploitation of nursing staff [6]: they were often burdened with more work than other medical professionals and were often blamed for irregularities occurring in therapy.
None of the studies on medical errors during COVID have attempted to comprehensively determine the influence of the conditions of the epidemic on their occurrence. Therefore, this study aimed to determine how the COVID-19 pandemic affected the number and type of medical errors in Poland during the COVID pandemic, as well as the medical facility where the irregularity occurred, and then compare the results with those obtained from other countries.
Methods
The research material comprised inquiries regarding the correctness of medical proceedings related to COVID-19; these were received by our department from prosecutor’s offices throughout Poland during the pandemic and after its end, i.e. from the beginning of January 2020 to the end of December 2023.
In cases involving allegations of medical malpractice, upon receiving notification of a potential criminal act, the prosecutor’s office is obligated to initiate an evidence-gathering process. Subsequently, the prosecutor seeks a forensic medical evaluation (expert opinion) to assess the occurrence and nature of the alleged malpractice. The prosecutor directs inquiries to relevant institutions or individual experts, asking about their willingness to provide forensic opinions, the estimated timeframe for the issuance of them, as well as the associated costs. Such inquiries include a short description of the case.
Due to the nature of the work, concerning the statistical analysis of the examined material, obtaining the consent of the Bioethics Committee, as well as written informed consent from any of the subjects, was not unnecessary. The analyzed material was anonymized.
The present analysis focused on the following information: the date of the event, the date of receipt of the inquiry to the department, and the characteristics of the case concerned:
the stage of the proceedings at which medical error was supposed to have occurred: primary health care, medical dispatchers/emergency medical teams, hospital, nursing home/care facility, sanatorium, or other,
whether a teleconsultation took place during the medical procedure,
whether the case was related to vaccination,
whether the case concerned COVID-19 directly (resulting from the broadly understood incorrect diagnosis or treatment of COVID-19) or indirectly (resulting from health protection problems associated with the pandemic),
whether the injured party died,
whether the case involved a child.
Results
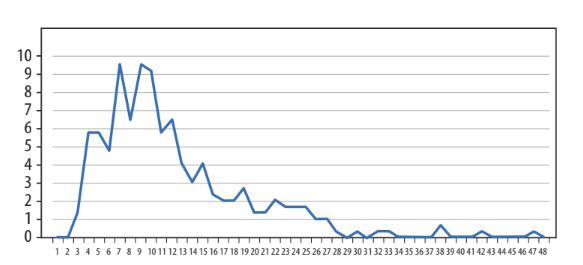
The examined period lasted 48 months, i.e. approximately 1,000 working days. During this time, the department received a total of 4,483 inquiries (approximately 4.5 per day). Of these, 293 were related to the COVID-19 pandemic (6.54%). These 293 data queries were analyzed according to the selected criteria. Figure 1 shows the monthly number of inquiries received according to the event date, and Figure 2 shows the number of inquiries received according to the date of receipt.
FIGURE 1
Monthly number of inquiries by event date. The number of inquiries is indicated on the vertical axis and the event date on the horizontal axis
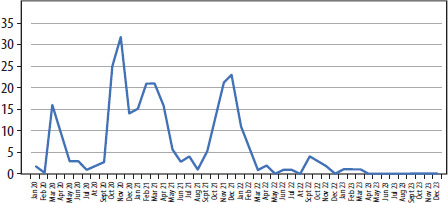
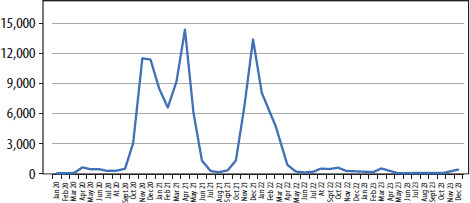
FIGURE 2
Monthly number of inquiries by date of receipt. The number of inquiries is indicated on the vertical axis and the receipt date on the horizontal axis
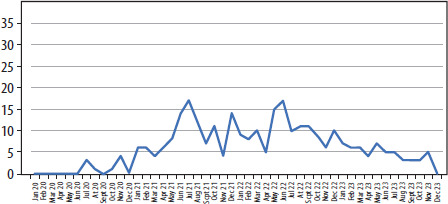
The period between the date of the incident and the date of receipt of the inquiry was also assessed. Typically, seven to nine months passed between the event and the impact date, although some inquiries took two months or four years. Figure 3 shows the time in months between the event date and the date the inquiry was received.
FIGURE 3
Time in months between the date of the event and the date the inquiry was received. The number of cases is indicated on the vertical axis and the period on the horizontal axis
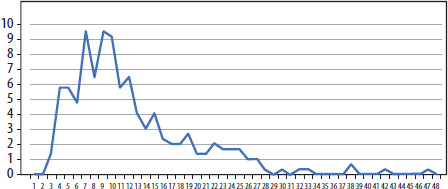
Figure 4 presents the number of infections due to COVID-19 in the period in question, and Figure 5 the number of deaths.
FIGURE 4
Number of SARS-CoV-2 infections. The number of infections is indicated on the vertical axis and the period on the horizontal axis
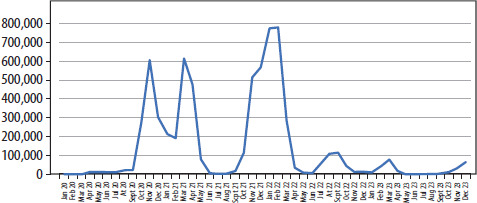
FIGURE 5
Number of deaths from COVID-19. The number of deaths is indicated on the vertical axis and the period on the horizontal axis
Figures 4 and 5 indicate that the pandemic had three peaks: the first in the fall of 2020, the second in the spring of 2021, and the third from the fall of 2021 to the winter of 2021/2022.
Regarding location, most cases concerned a hospital setting (243 cases), especially in ICUs, but many were associated with pre-hospital medical care, i.e. primary health care and EMS (in a total of 91 cases). Unusual situations regarding exposure to direct danger of loss of life or serious damage to health were classified as “other”, e.g. during social protests, such as those related to the Constitutional Tribunal’s judgment on the admissibility of terminating a pregnancy in certain conditions, or due to the opening of catering establishments during lockdowns. Many inquiries concerned the correctness of procedures at multiple stages, i.e. from primary care through emergency medical services to the hospital. Twenty-four out of 41 cases related to primary care concerned teleconsultation, and in such cases, the most common question was whether there should have been a traditional in-person medical consultation, either in the clinic or at the patient’s home. The location of the medical service is given in Table 1.
TABLE 1
Location of medical service. The total number of events is greater than the number of cases because one injured party, i.e. each case, may have been provided with medical assistance by several medical entities
| Medical entity | |
|---|---|
| Primary Health Care | 41 (including telephone consultation) |
| Ambulance | 50 |
| Hospital | 243 |
| Nursing home/MCE | 11 |
| Sanatorium | 4 |
| Other | 4 |
TABLE 2
Data including several deaths of the aggrieved, their age (adults or minors), the occurrence of vaccination, the number of the aggrieved per case (inquiry), and the type of relation to COVID-19
| Death | Child | Vaccination | More than 1 person | Type of relation with COVID-19 |
|---|---|---|---|---|
| Yes, n = 281 | Yes, n = 10 | Yes, n = 23 | Yes, n = 11 | Direct, n = 218 |
| No, n = 16 | Indirect, n = 75 | |||
| Lack of data, n = 2 |
Most of the analyzed cases were fatal (281 cases); however, death was uncertain (lack of data) in two cases. Only 10 cases concerned a child, but some inquiries concerned newborns and 17-year-olds. Twenty-three cases concerned qualification for vaccination, and a possible causal relationship between vaccination and deterioration of health or death. Only 11 cases concerned more than one person, with the number of people ranging from two to 180. These typically concerned the conduct in nursing homes, emergency medical teams, and sanatoriums, as well as the correctness of isolation procedures and liability issues when a resident developed SARS-CoV-2. The vast majority of the cases discussed concerned people who were suspected or diagnosed with COVID-19 at some stage of the medical procedure (218 cases). Nevertheless, quite a few (75 cases) were related to indirect aspects of the pandemic; these typically concerned failure to provide help, failure to admit to various medical facilities, admission to the wrong ward, failure to perform diagnostics, or failure to implement planned or emergency treatment.
Discussion
The pandemic has resulted in numerous changes and has impacted many aspects of our lives. Considering that medical personnel who often did not have the necessary qualifications were assigned to anti-epidemic activities, there was a real risk that they would make medical errors resulting in criminal liability for the aforementioned acts. In addition, the risk of error was caused by an extraordinary situation in which medical personnel had to take care of a large group of patients in a short time. Therefore, even if they had the appropriate experience and qualifications, organizational reasons could lead to conduct inconsistent with the adopted standard, and therefore to liability for a medical error. It was therefore decided to introduce a regulation to eliminate the risk of liability. The legislature responded to the effects of the pandemic by introducing Article 24 of the Act of October 28, 2020, amending certain acts in connection with counteracting crises related to COVID-19 (Journal of Laws of the Republic of Poland, item 2112, as amended), which formally came into force on November 29, 2020, but in practice from March 14, 2020. In those regulations, a provision was introduced excluding the criminal liability of persons providing health services in connection with COVID-19 for unintentional offenses against life or health specified in this provision (e.g. involuntary manslaughter or serious injury to health). The condition for using the regulation in question is to state that the perpetrator acted “in special circumstances”. The act does not define this concept and does not indicate, for example, situations that could be so qualified. However, taking into account its purpose and the circumstances of introducing this construction, it can be assumed that these special circumstances may be caused by, for example, capacity constraints within the hospital, inappropriate equipment, resource shortages, or increased morbidity resulting in the need to provide health services to many patients simultaneously. A medical worker may avoid liability if he or she has not caused a gross failure to exercise diligence required in the given circumstances. The essence of this regulation is therefore to state that there was a breach of the rules of caution required in the given circumstances, which is a premise for attributing negligence, and thus liability for the listed acts – a medical error occurred. Liability is excluded at the stage of assessing whether this breach of the rules was gross. However, this is a very ambiguous concept and requires assessment in concreto with the participation of experts.
The application of the discussed regulation therefore requires the following circumstances to be determined:
Did the medical employee’s conduct meet the legal/statutory definition of the given crimes, including whether negligence can be attributed to them (i.e. did they commit a medical error)?
Did the medical employee’s conduct take place during a state of epidemic threat or epidemic state (and in a place where such a state was declared)?
Did the medical employee act in special circumstances?
Did the medical employee not “grossly” violate the caution required in the given circumstances?
From a procedural point of view, the body responsible for prosecuting crimes should therefore determine whether the perpetrator’s conduct exhausted the features of the aforementioned crimes, and in particular whether unintentionality can be attributed. Determinations in this respect require an examination of whether the perpetrator violated the rules of caution required in the given circumstances. Considering that the assessment in this respect requires specialist knowledge, it is necessary to seek the opinion of experts. As a consequence, such cases were administered to experts.
According to the National Prosecutor’s Office, a total of 9,178 proceedings regarding suspicion of medical error were initiated in the period 2020-2023, with roughly half (48.8%) of all such cases being processed by our department. As such, the corpus of cases included in the present study is very much representative of the picture of the entire country. Articles do not include the cases reported to the Voivodship Commission for Adjusting Medical Events (these stopped their activity on 30.06.2024) as well as district and supreme medical courts run by medical self-governments. We focused on prosecutorial cases, as this is the main way of explaining cases related to the suspicion of a medical error in our country. With regard to the activities of the above-mentioned committees, it should be pointed out that their dissolution confirmed their negligible importance in the context of the consideration of such cases.
A clear correlation was found between the monthly number of SARS-CoV-2 infections and deaths due to COVID-19 (Figures 4 and 5). It was found that Poland experienced three peaks (waves) of the pandemic; the first took place in the fall of 2020, the second in the spring of 2021, and the third lasted from the fall of 2021 to the winter of 2021/2022. As expected, most deaths were related to the largest waves of infections, and these data correlated with the number of inquiries received about the event date (Figure 1). However, it should be noted that no clear correlation was observed regarding the date of receipt of inquiries; this is to be expected as interested persons report cases at very different times, and prosecutors need varying amounts of time to collect evidence. The first clear peak in the number of such cases was noted in the spring and summer of 2021, about half a year after the first wave of the pandemic.
The cases concerned all aspects of medical procedures, all medical professions, and all healthcare entities. Inquiries regarding the following topics were received:
diagnostics (hospital, clinic, teleconsultation),
referrals to hospital (no referral, delayed referral to the hospital),
hospital admissions (waiting too long for admission, not being admitted to hospital),
treatment (all aspects, including e.g. death due to oxygen depletion),
no possibility of “normal” hospitalization because the ward was changed to a “COVID” facility,
no possibility of “COVID” hospitalization because the wards were “ordinary” and the patient was transported further,
improper conduct/care in nursing homes, sanatoriums, and hospitals (cases sometimes involving hundreds of patients),
inappropriate isolation procedures in nursing homes, sanatoriums, and hospitals (“he came in healthy, left sick”),
administration of the vaccine despite contraindications (according to the family), deaths after vaccination,
diagnosis of COVID-19, and there was another disease that was not treated,
exposure due to being sent to work in a “COVID” hospital,
opening of premises/street demonstrations during lockdowns and exposure to many people.
It should be emphasized that most of the types of errors cited above also occurred before and after the pandemic. Therefore, these are not errors “specific” to the circumstances related to COVID-19. Before, during and after the pandemic, the experts had to deal with reservations about diagnostics (except for the issue of teleconsultation, as this form appeared in practice in Poland in the period in question), the issue of referrals and hospital admissions, reservations about treatment, and the conduct of medical staff in a number of different medical entities, in matters not related to COVID-19.
It is difficult to compare the obtained data regarding the domestic situation with those reported in other countries. Firstly, this is due to the state’s criminal policy regarding medical errors which has dominated Poland in recent years. This policy resulted in criminal rather than civil proceedings, as is the case in most countries worldwide. As such, the Polish prosecutors’ offices have been deluged with cases of criminal malpractice, and it was not possible to identify comparable medical errors related to COVID-19; the foreign articles focused on general systemic issues and were aimed at preventing future errors rather than prosecuting medical personnel. It should also be noted that most foreign publications could draw their conclusions without data analysis, as they were quite general and intuitive. They also focused on the general causes of errors during the COVID-19 pandemic, such as system overload or staff fatigue, which even laypeople with no connection to medicine could recognize without needing specialist research.
To sum up, the COVID-19 pandemic undeniably harmed the healthcare system in Poland and abroad. These consequences included limited access of patients to medical care, characterized by routine use of teleconsultations and limited admission of patients to hospitals and specialist cli-nics. The medical services themselves suffered from poor organization and insufficient and overloaded medical staff. As such, both the diagnosis and subsequent implementation of appropriate diagnostic and therapeutic procedures were delayed, both in COVID patients and those with other conditions. Such delays resulted in the deterioration of the condition of the patient, and possibly death.
Despite introducing legal regulations intended to decriminalize the consequences of medical errors related to the COVID-19 pandemic, such cases were still submitted to prosecutors’ offices. These regulations are not perfect. They were adopted ad hoc, in response to the expectations of the medical community, which counted on the exclusion of liability for acts committed during an epidemic. However, due to the structure of the provision in question and the procedural conditions, the bodies responsible for prosecuting crimes must carefully analyze whether there was a violation of the rules of caution and, if so, whether it was a flagrant violation. In addition, they must determine whether the features of the listed types of crimes have been exhausted, e.g. determine whether the perpetrator exposed the patient to a direct risk of loss of life or serious damage to health. As mentioned, assessments in this regard require specialist knowledge – hence the need to involve experts. It is therefore not surprising that the procedural bodies request their opinions, which naturally prolongs the proceedings in such cases. The complaints associated with COVID-19 concerned all aspects of medical proceedings, all medical professions, and all healthcare entities.